
Abstract
This audit aimed to measure the impact of introducing and then modifying an electronic patient record (EPR) system on the uptake of HIV testing at a level 3 genitourinary medicine service. It was a retrospective case note review of all new and rebook patients attending our service in 2007 (paper records) and 2010 (EPR), and a prospective review in 2012 (following modification of the EPR). The uptake of HIV testing increased significantly from 72.8% to 78.1% following introduction of the EPR (p = 0.009), and increased further to 86.6% (p < 0.0001) following modification of the EPR. Clinics using paper notes should consider switching to EPR as a means of increasing HIV testing uptake.
Introduction
The BASHH/MEDFASH Standards for the Management of Sexually Transmitted Infections (STIs) 2010 recommend that 100% of genitourinary medicine (GUM) patients should be offered an HIV test with a minimum uptake of 60% at their first STI screen. 1
Electronic patient records (EPRs) are being increasing utilised within GUM, and there is evidence that using an EPR may improve patient care. Studies have shown that a prompt on the EPR could increase screening of bacterial STIs in men who have sex with men (MSM)2,3 and decrease the ‘time to treat’ for patients diagnosed with chlamydia. 4
The use of a prompt within the EPR has been identified as a possible facilitator for increasing HIV testing, 5 but its potential impact on actual HIV testing rates in GUM clinics has not been assessed.
The aim of the audit was to assess whether the introduction of an EPR resulted in an increase in uptake of HIV testing in a level 3 GUM service, and whether EPR modification could further increase uptake of HIV testing.
Methods
This audit was a retrospective case note review of all new and rebook patients attending our service (venue 1) in October 2007 (paper record) and October 2010 (following introduction of an EPR, with a prompt for HIV test offered), and a prospective case note review in April 2012 (following changes to the EPR with prompts for reasons for declining an HIV test, and for offering point of care testing [POCT] to needle-phobic patients).
The paper notes were made on blank lined paper (i.e. no proforma existed), the EPR consisted of a series of fields to be completed by the clinician, some of which were compulsory (a bespoke EPR using Blythe Lillie software). The EPR was introduced in September 2009 and at inception contained a compulsory field for ‘HIV test offered – yes/no’. In March 2012, the ‘HIV test offered field’ was altered to ‘HIV test offered – yes/declined/recent test (3 months)/antenatal/blood donor/needle phobic/doesn’t want to know’, and a further compulsory field added for ‘If needle phobic, POCT offered – free text response’. The clinician was required by the software to complete all compulsory fields before the EPR could be saved. There was free space in the EPR for other comments regarding any discussions with patients to be entered and these were also reviewed when relevant to a discussion regarding HIV testing.
Patients accepting HIV testing were identified by the SHHAPT codes S2, T4 or P1A and those declining by the code P1B. Patients with a SHHAPT code H (indicating an HIV diagnosis) or P1C (HIV test inappropriate) were excluded. The notes of patients without one of these codes were reviewed to assess whether they had accepted HIV testing.
In order to attempt to assess the impact of the EPR in comparison to other factors, we reviewed the coding for patients at an alternative level 3 GUM service at a local district hospital (venue 2) with paper notes throughout the audit period. The same methods were used to analyse patient codes. Notes of patients without a code were not further analysed.
Statistics
Data were analysed using Fisher’s exact test.
Results
Effect of change in patient record type on patients’ acceptance of HIV testing.

Assuming those not coded were tested for HIV.
Patients declining HIV testing in 2010 and 2012 at venue 1 were further analysed. There were no significant differences in the gender of patients refusing an HIV test in 2010 (p = 0.43) or 2012 (p = 0.21).
Reasons for patients declining HIV testing.

When a reason for declining HIV testing was documented, the most common reasons were the patient having had a recent HIV test and believing they had not had a subsequent risk, or believing they were too low risk to justify testing (see Table 2). Despite this, 51% of patients had factors placing them at a potentially increased risk of HIV compared with the general population (see Figure 1).
Factors indicating possible HIV risk in patients declining HIV testing in April 2012 (n = 124).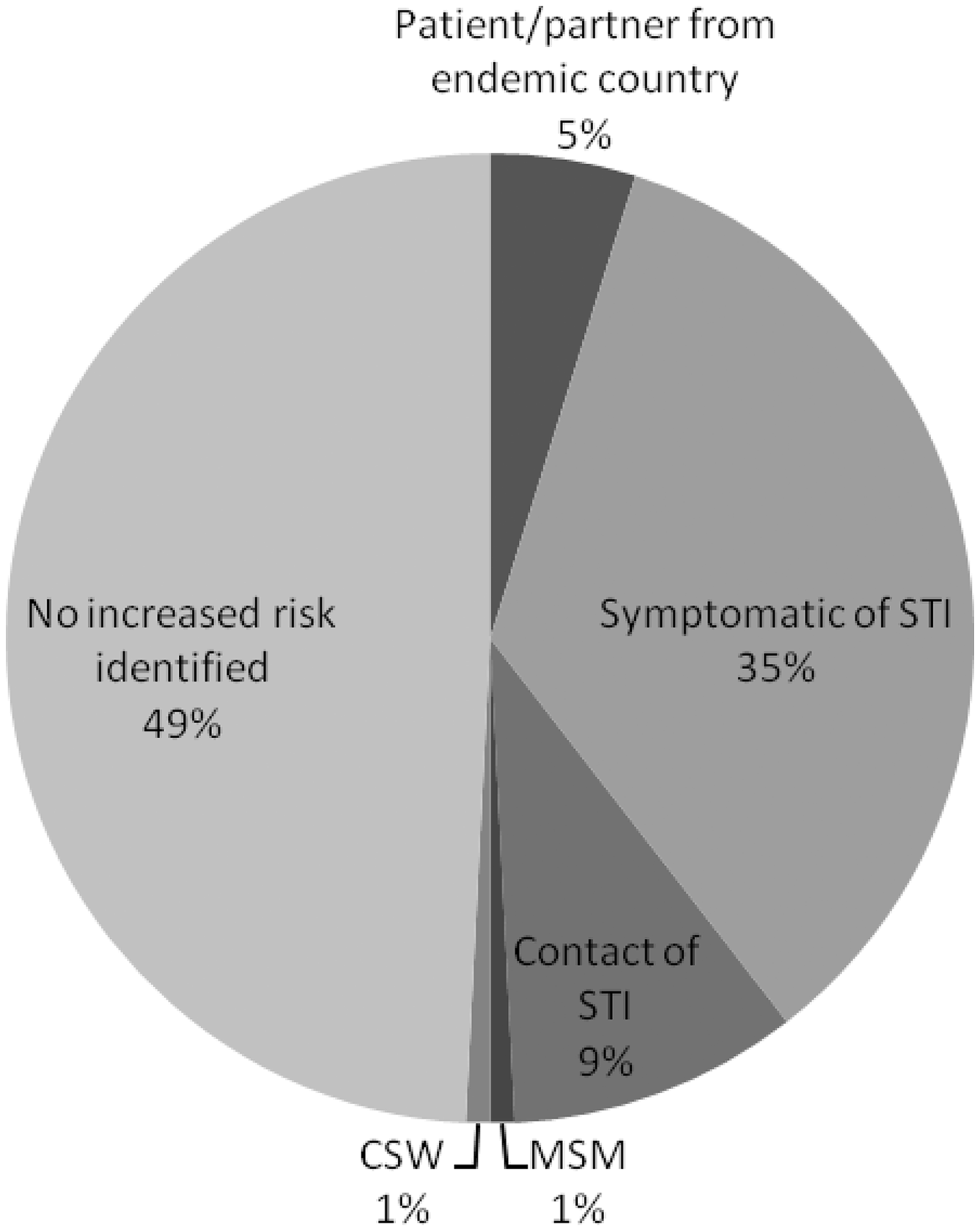
The use of POCT within our service has risen over time, and done so more rapidly since 2011 (see Figure 2).
Increase in use of POCT in our service over time.
Discussion
The use of an EPR in HIV care is becoming increasingly recognised and has been used in identifying patients eligible for HIV testing in emergency departments, 6 and to improve care of patients with HIV in developing 7 and developed 8 countries. A further study looked at a real-time electronic clinical reminder which encouraged HIV testing and improved testing rates in at risk patients in the Veterans Health Administration at two sites from 4.8% to 10.8% and from 5.5% to 12.8% (p < 0.001), in comparison with no change in testing at control sites. 9 The introduction of the EPR with a prompt for HIV testing has significantly improved uptake of testing at our clinic, further improved by small changes to the EPR with prompts requiring staff to explore patients’ decision making and offer POCT to needle-phobic patients.
In order to attempt to quantify the potential level of contribution of the EPR to the increase in HIV testing, we reviewed HIV testing at an alternative local level 3 GUM clinic (venue 2). This clinic had paper records throughout the audit periods and showed a statistically significant decrease in acceptance of HIV testing. It is beyond the scope of our audit to comment on the reasons for this as we did not analyse patient notes from this centre, but it provides some ecological evidence of the possible contribution of the EPR to an increase in testing in our service.
It is possible that the EPR alone is not solely responsible for the increases in HIV testing seen. The BHIVA UK National Guidelines for HIV Testing were introduced in 2008 10 and the BASHH/MEDFASH Standards for the Management of Sexually Transmitted Infections in 2010, 1 both of which reiterated the need for universal testing of all patients attending GUM clinics and may have contributed to the increase in acceptance of HIV testing between our audits in 2007 and 2010. However, there were no meetings or education sessions within the department between the audit dates in 2007 and 2012 encouraging an increase in HIV testing – it has been clinic policy for several years prior to 2007 to offer HIV testing to all patients attending our clinic. It may be inevitable over time that increasing staff awareness leads to an increase in encouraging reluctant patients to accept HIV testing, and also that with increased health promotion in the community, patients are more willing to accept HIV testing over time. Again, these alternative explanations seem less credible considering they were not seen at the alternative local level 3 GUM service.
6.0% of patients declined HIV testing in October 2010 due to needle phobia, and 9.7% in April 2012. In March 2012, clinic policy changed and needle-phobic patients declining venesection for HIV testing were offered a POCT. At the same time, a prompt was added to the EPR reminding clinicians to offer a POCT to all needle-phobic patients. The use of POCT in our service has been rising since introduction in 2008, and rising exponentially since 2011 (see Figure 2). However, many patients declined this also due to extreme needle phobia, and it may be beneficial to consider the introduction of a saliva-based test for these patients to encourage a further increase in testing.
Given that our audit found that using paper to take patient notes with no proforma achieved an HIV testing rate of 72.8% in 2007, the BASHH MEDFASH Standards recommending a minimum uptake of 60% 1 for HIV testing appears to be too low. We believe that a higher target of at least 70% should be set in order to encourage clinics to improve their testing rates.
There is still considerable scope for improvement, with many patients declining HIV testing having factors which may place them at an increased risk of HIV, and so continued efforts are required to further increase acceptance of testing. Possible methods to further increase HIV testing could include ongoing patient education and health promotion both within clinic and in the community. The prompt could also be further improved with the removal of the ‘declined’ option as a reply to the field ‘HIV test offered’ and a free text box inserted requiring a specific reason for declining to be given when it differs from one of the other reply options.
Services still using paper notes should consider changing to an EPR and those services using an EPR should continue to evaluate its effectiveness and consider modifications to improve patient care.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.