
Abstract
This study investigated whether a Chlamydia diagnosis was associated with relationship breakup or physical violence from partners when compared to other attenders at a sexually transmitted infections (STIs) clinic. Patients diagnosed with Chlamydia and who had a regular partner at the time of diagnosis, were contacted 3–12 months later and completed a questionnaire on relationship history. A comparison group of gender-matched non-STI patients were also interviewed. About half of Chlamydia cases (exposed) and non-cases (unexposed) had broken up with their partner since diagnosis (52% vs. 47%; p = 0.42), but cases were more likely to have split up within one week of diagnosis (48% vs. 24%; p = 0.003), and somewhat more likely to resume the relationship (24% vs. 15%; p = 0.24). The prevalence of reported physical violence in the past year was slightly higher in cases than the unexposed group (9% vs. 4%; p = 0.09). Cases that saw a health adviser were less likely to report experiencing physical violence than those who had not seen a health adviser (7% vs. 12%: p = 0.31). Patients with Chlamydia are more likely to suffer relationship breakup soon after diagnosis than STI clinic attenders without an STI. Health advice should include reassurance about sexual relationships as well as safer sex.
Keywords
Introduction
Physical violence between sexual partners has received increasing attention in the medical literature in recent years. Most reports have identified women as the victims and men as the perpetrators of violence. However, men are also frequently identified as victims of violence from their regular female partners.1,2 Some studies have shown an association with sexually transmitted infections (STIs),3–6 more specifically with Chlamydia. 7 Most of these have been in the USA and there is only limited information in the UK among STI clinic attenders. Other studies have focused on domestic violence in sexually transmitted disease (STD) clinic attenders8,9 and sexual violence 10 in women in the general population.
Little is known in the UK about what happens to relationships if one partner is diagnosed with a STI. In the case of Chlamydia, most cases diagnosed in STI clinics are interviewed by health advisers in the acute follow-up period. This is usually to identify partners at risk of infection, assess compliance both with medication and abstinence from sex until completion of the course of treatment.
The aim of this study was to compare the prevalence of physical violence amongst STI clinic attenders with and without Chlamydia, and to estimate whether relationships were more likely to dissolve after a Chlamydia diagnosis compared with patients without an STI.
Methods
This was a retrospective cohort study in which patients diagnosed with Chlamydia who had attended an STI clinic in London and had a regular partner at time of diagnosis were contacted 3–12 months after their attendance and asked to complete a questionnaire either over the phone or in a face-to-face interview. An equal number of gender-matched controls were selected from repeat attenders to the clinic who had not been diagnosed with any STI at their last attendance and who also reported a regular partner at their previous attendance between 3 and 12 months previously. Participants were aged 16 and over and consented that they could be contacted by phone before being asked about the study. Questions were asked about sociodemographic variables, recent partners, contact with health advisers, whether they had either experienced physical violence from a sexual partner in the past year, broken up with a partner just after their attendance when diagnosed with Chlamydia or, in the case of the non-exposed cases, immediately following their previous attendance. Most of the Chlamydia cases were contacted for interview by phone and a few when they reattended the clinic for another reason. In addition, subjects were asked whether, if they split up with their partners, did they get back together and if so, was it on a regular basis or just for a very short time. Subjects were also asked if they had experienced difficulties in establishing subsequent relationships or whether they carried on as normal as though there was minimal impact from their Chlamydia diagnosis (exposed) or subsequent attendance (non-exposed).
Most of the non-Chlamydia cases were interviewed when they attended the clinic as a repeat attender and a few by phone. Only one of the Chlamydia cases and one of the non-exposed group declined the study.
The sample size was calculated as 150 cases and 150 controls, to provide 80% power to detect a difference in prevalence of breakup of 35% among cases and 20% among non-cases. The estimate of 35% was made by doing a pilot study look-back of case notes of 20 patients attending the clinic with Chlamydia who had attended subsequently with a new problem. Logistic regression was used to estimate odds ratios (OR) and 95% confidence intervals (CI) for associations between exposure status (Chlamydia cases vs. non-cases) and outcomes of interest.
Chlamydia testing was performed with the BD VIPER system (Becton Dickinson, Franklin Lakes, New Jersey, USA) using strand displacement amplification for qualitative detection of C. trachomatis DNA.
Patients diagnosed with Chlamydia in our clinic are referred routinely to a health adviser for further counselling. This may involve a face-to-face interview or discussion over the phone to confirm that treatment has been given, partners treated and sexual abstinence has occurred until completion of a course of treatment and documentation that partners have finished a course of treatment.
Results
Sociodemographic variables, history of physical violence, contact with health advisers and relationship breakup amongst Chlamydia cases and non-cases.
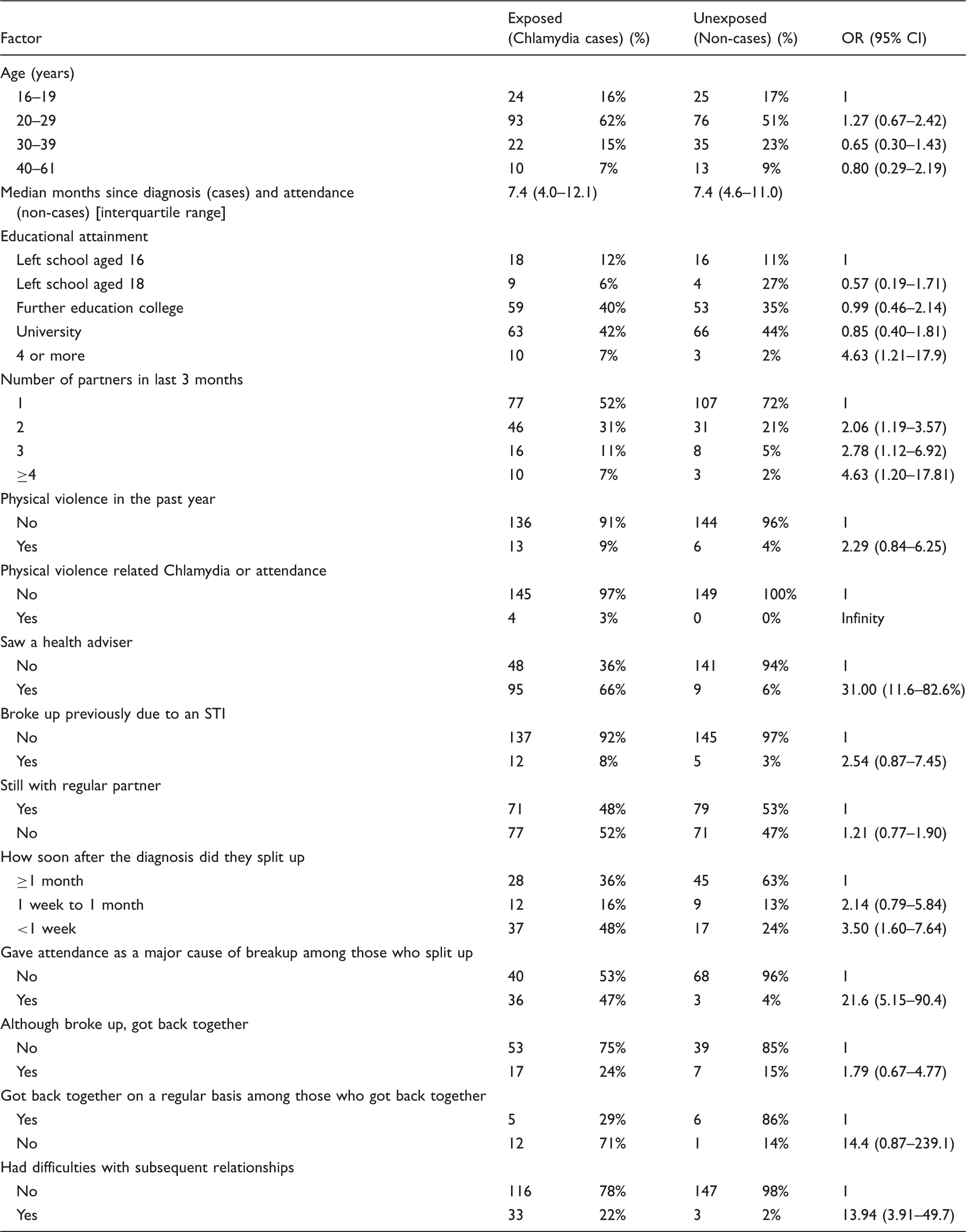
Chlamydia cases were more likely to get back together again than non-cases but this reconciliation was short lived, with the majority of cases back on an irregular basis (71%). Twelve of the cases and five controls had broken up previously because of a STI (OR 2.54, 95% CI 0.87–7.45). Regarding subsequent relationships, Chlamydia cases were more likely than non-cases to report difficulties with subsequent relationships (22% vs. 2%, OR = 13.94, 95% CI 3.91–49.7).
Chlamydia cases were more likely to report physical violence in the past year than non-cases (9% vs. 4%; OR = 2.29, 95% CI 0.84–6.25). This was similar by gender (p = 0.82). Among Chlamydia cases, the proportion experiencing physical violence was slightly lower among those that saw a health adviser (7.4% vs. 12.5%; p = 0.31). There was no difference in the proportion who reported difficulty in establishing subsequent relationships by whether or not they saw a health adviser (23.4% vs. 20.8%, p = 0.71).
Discussion
Relationship breakups soon after diagnosis were more common in Chlamydia patients than non-cases. Our study found that 48% of Chlamydia cases had broken up within a week of their diagnosis, a much higher rate than in a general practice setting in Denmark where 10% broke up as a consequence of their positive test result. 11 Chlamydia cases were more likely to get back together again initially, but then more likely to break up again. This pattern could reflect length of relationship, 12 a variable that we did not enquire about, or the fact that Chlamydia cases had more sexual partners than non-cases and may have had less inhibition in sexual activity following a Chlamydia diagnosis. Not surprisingly, partner change has been associated with both acquisition of Chlamydia, gonorrhoea and trichomoniasis in a US study 13 and higher risk-taking behaviour in France. 14
We also found a subgroup that experienced difficulties with subsequent relationships after Chlamydia despite seeing a health adviser. Clearly it would be beneficial for all cases to have access for further discussion so that those with more frequent partner change can be advised about the personal and public health risks of STIs. In our study, one-third of Chlamydia cases did not see or discuss their diagnosis with a health adviser although all were given the opportunity to do so. Clearly this group requires a different approach to counselling in the limited time that is available although how this is done is unclear. It may be that a few standard questions are asked at the beginning of the consultation so that the best outcome is achieved for both the individual and the public health. Relationship dissolution has a significant health and quality of life impact 15 and in view of the significant breakup rate in our study, this issue should be addressed so that vulnerable individuals can be forewarned about what may lie ahead. Further studies should investigate optimal ways of delivering health adviser advice to subjects with STIs.
We acknowledge there may be limitations in the reporting of relationship difficulties, including on/off relationships that could reflect different sexual mixing patterns. However, any potential bias would be expected to occur in both cases and non-cases.
Overall prevalence of physical violence was low compared to other studies. There may be a number of explanations for this. The definition of violence is open to considerable variation. In our case, we used an open-ended enquiry leaving it up to subjects if they felt they had suffered physical violence and did not include psychological, financial or emotional aspects of abuse. We used a relatively short recall period of one year, whereas some other studies have used a lifetime history of violence in their enquiry. Variation in sociodemographic variables, ethnicity and socioeconomic factors may also have accounted for our low prevalence of violence.
Finally, a study of antenatal attenders in the USA found that women who reported more sexual abuse were more likely to have experienced STIs than non-victims 16 and the design of our study does not allow for a causal relationship between Chlamydia and breakup and violence to be established. Further prospective longitudinal studies should be undertaken to identify the relative timing of events between these variables and examine additional possible confounding factors that might be relevant.
Footnotes
Acknowledgements
The authors thank Julie Githiri-Goko and Adina Wineman for assistance with the project. The study was supported by the Ealing Hospital NHS Trust Research Fund. The study was approved by both the Northwick Park Hospital and London School of Hygiene and Tropical Medicine ethics committees.
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.