
Abstract
In Iran, the HIV/AIDS epidemic is growing during an era of scaling up the national surveillance system and antiretroviral therapy programs. We examined the early loss to follow-up and mortality rates in a retrospective cohort of 1495 HIV-infected patients by survival proportional hazard Cox model. We also conducted a data abstraction sub-study in a systematic random sample of 147 patients to assess the association between mortality and predictor factors. Overall, 17.3% patients were not seen after their first visit and 17.4% more were lost by 6 months. The overall mortality rate was 7.0 (95% CI 6.1–8.1) per 100 person-years. Moreover, crude mortality rate was higher in men (8.6) than in women (1.7), with an age-adjusted hazard ratio for men compared to women of 4.55 (95% CI 2.31-8.93). Lastly, history of tuberculosis and not being on antiretroviral therapy were significantly associated with higher mortality in the patient sub-sample.
Keywords
Introduction
Unlike the world as a whole, the prevalence and the incidence of HIV have grown over the last decade in the Eastern Mediterranean Region (the WHO designation roughly corresponding to the Middle East and North Africa or MENA), doubling to approximately 500,000 people living with HIV.1,2 We fear that early diagnosis, supportive care, and antiretroviral therapy (ART), and, as a result, survival may also be lagging behind the industrialized world. It is very encouraging that in the USA and Europe, a person acquiring HIV in 2005 who started ART without delay is expected to survive as long as an uninfected person. 3 Moreover, the causes of death begin to resemble those of people without HIV and not the previous AIDS-related causes such as opportunistic infections or specific cancers.4,5
Unfortunately, the estimated ART coverage in MENA is only 8% of persons eligible according to current WHO guidelines. 6 Without wide ART coverage, the mortality rate of HIV-infected patients is likely high. In the region, the availability, access, and quality of prevention and care interventions are mixed, although many MENA countries (including Iran) have made some progress over the last few years. 2 Given the low and concentrated epidemic patterns of HIV in MENA, the burden of disease disproportionately affects vulnerable groups, including injection drug users (IDUs), men who have sex with men (MSM), and female sex workers (FSW). Based on the most recent modes of transmission estimations, every year an estimated 10,000 new HIV infections occur in Iran; 56% are in IDUs. 7 In addition, HIV testing and counselling, and thus early diagnosis, present a serious challenge in the region where these populations are highly stigmatized and their behaviours illegal with potential severe punishments. Such high levels of stigma leads to denial and under-reporting of high-risk behaviours in case reporting, low HIV testing rates, and wide gaps in linkage to care and treatment services. 8 Finally, the population-level beneficial effects of ART on viral load suppression and subsequent onward HIV transmission are also unrealized in this regional of low coverage. 2
Based on the country progress/universal report 2011, the reported number of adults and children with HIV infection who are currently receiving antiretroviral therapy (ART) was 1800 in 2010, with an estimated ART coverage of 7% (6–8%). 2 Current projections indicate continuing increases in the number of HIV-infected people, AIDS cases, and AIDS-related death in Iran. 9 However, direct measures of mortality of persons diagnosed with HIV infection are lacking for the region. We therefore undertook a retrospective study of mortality rates and predictors among patients in the national referral clinic of Iran, focusing on those persons diagnosed after 2004 – the period following scale up of ART – to see if the benefits of treatment are effectively and equitably reaching persons living with HIV in Iran. In addition to mortality rate and its predictors, we also looked at the early loss to follow-up rate as an indicator of retention and link to care services in HIV-infected patients in Iran.
Methods
We examined data originating from the national referral centre for HIV/AIDS testing, counselling, and treatment in Iran – the Iranian Research Center for HIV/AIDS (IRCHA), situated in the Imam Khomeini hospital in Tehran, the capital and largest city of the country. Established in 2004, IRCHA serves as the nation’s highest level public referral centre for HIV/AIDS. It provides prevention, care, and treatment services free of charge. For every newly-identified HIV patient, demographic data, the most plausible route of transmission, medication history, laboratory tests, co-infections, and the date of diagnosis are recorded. Such data are collected by trained physicians in the centre and entered into an electronic medical record database. There is a follow-up review for each patient who is on ART at least every 3 months. There is also an HIV-positive support group and hotline in place to provide social and networking service referrals for patients and to answer questions patients may have regarding their disease or treatment.
Patients who are HIV positive are also seen, in principle, at least every 3 months by infectious diseases specialists, when CD4 counts are performed. At the time of the study, ART initiation was offered when the CD4 count fell below 200 or for other clinical indications. By the time of the study, 1645 patients were registered, while 1495 were eligible for this study and their data were extracted from their registered medical records. Then, a random sub-sample of 147 patients were contacted by a trained research assistant to collect additional complementary data about their risk behaviours, ART as well as the end-point outcome, mortality.
We used STATA v. 12 for data analysis. t-Test and chi-square tests were applied for comparing male and female HIV patients according to numerical and categorical variables, respectively. For the early loss to follow-up and mortality, we estimated the rates per 100 person-years follow-up. Since the proportionality assumption was not violated, we used the proportional Cox model to explore the predictors of mortality. We did not observe any significant interaction between the predictors. The study protocol was reviewed and approved by the IRB – at Tehran University of Medical Sciences. All medical record data were treated as confidential and analysed anonymously. For those who participated in the sub-sample, verbal informed consent was obtained.
Results
Of all HIV-positive patients diagnosed after 2004 (N = 1495), the majority was male (81.6%) and the average age for men and women was 34.6 (SD = 9.3) and 30.7 (SD = 11.1) years, respectively (t test = 3.86, p = 0.001). Overall, 259 (17.3%) patients were not seen after their first visit and 260 (17.4%) were lost in the first 6 months following the first visit. More men were lost after the first visit compared to women (18.5% vs. 8.8%; p value = 0.001). The maximum follow-up was 7 years and the most recent visit was recorded on 1 December 2010. Overall, 188 (12.6%) patients died during the study period; in 96 (6.3% of patients) the deaths were observed within the first 6 months of follow-up.
The overall mortality rate was 7.0 per 100 person-years (95% CI 6.1–8.1) during the total 2652.0 person-years of follow-up. The crude mortality rate was significantly higher in men (8.6 per 100 person-years, 95% CI 7.3–9.9) compared to women (1.7, 95% CI 0.9–3.16). One- and five-year adjusted survival rates were 88% (95% CI 86%–90%) and 73% (95% CI 69%–77%) in men and 96% (95% CI 93%–98%) and 95% (95% CI 91%–97%) in women. Figure 1 also illustrates the significantly worse survival rate among men compared to women (chi-square 26.6, p = 0.001). Male mortality was higher than that of female for all age groups. In Cox proportional hazard analysis, the hazard ratio (HR) for men compared to women, adjusted for age, was 4.55 (95% CI 2.31 − 8.93). Although older age was significantly associated with increased mortality in bivariate analysis, it was borderline in multivariate analysis when included with gender (HR 1.11, 95% CI 0.94 − 1.31, p = 0.06). The predicted median survival time was 10.1 years. The predicted median survival time (adjusted for age) was 43.6 (95% CI 42.9−44.3) years for women and 9.0 (95% CI 8.9−9.1) for men.
HIV mortality, percentage event-free (survival curve) by gender, adjusted for age at diagnosis; HIV clinic patients, Tehran, Iran (N = 1495).
Characteristics of HIV-positive patients stratified by gender, Tehran, Iran, 2004–2010 (n = 147).
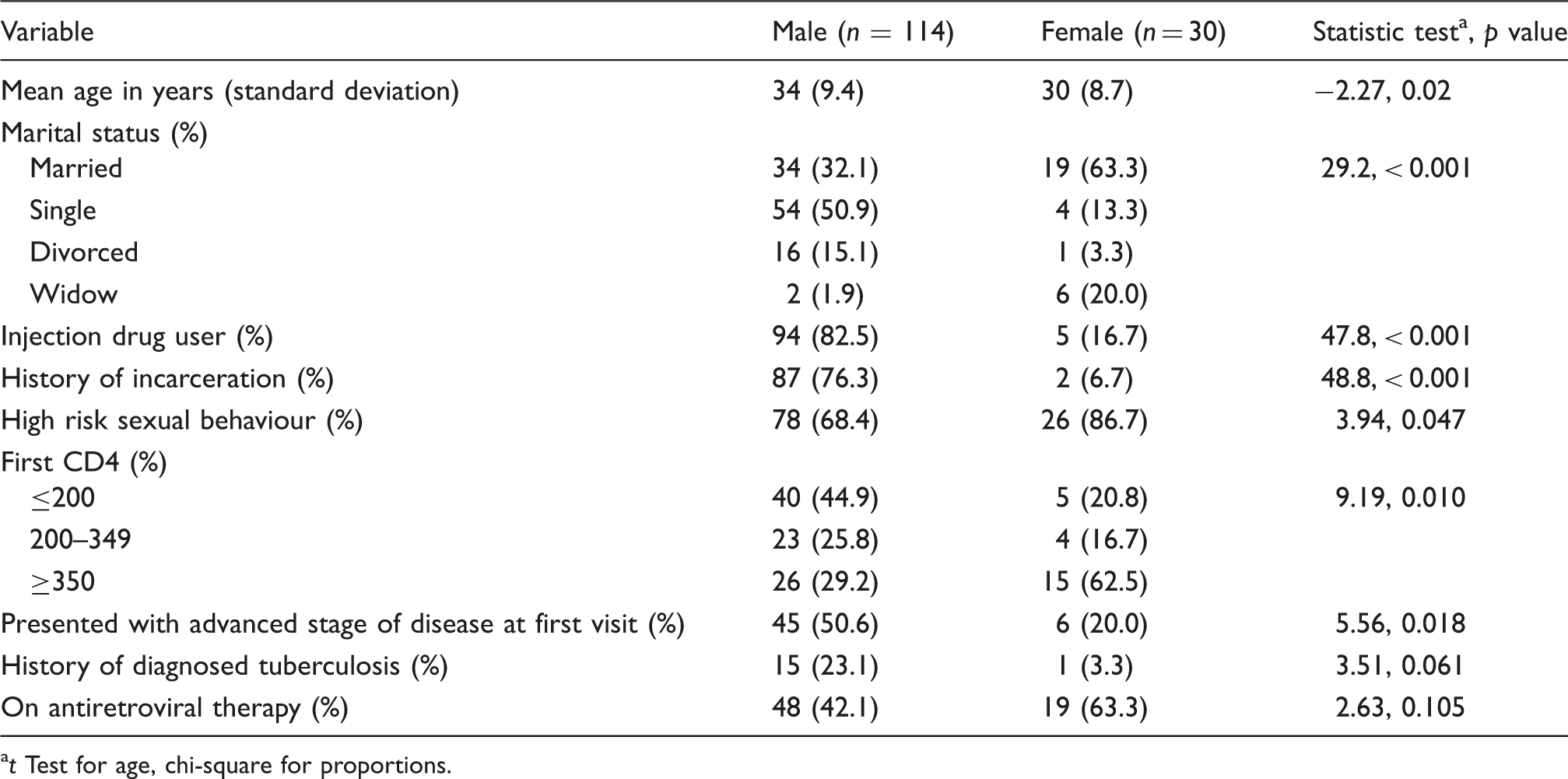
t Test for age, chi-square for proportions.
Discussion
Overall mortality in our retrospective study in Iran appears higher than other clinic populations worldwide, likely due to the late diagnosis and advanced stage of disease at presentation. These factors are particularly poignant for men, in whom we observe a greater than four-times higher hazard rate of death compared to women. Partially explaining and compounding the difference, men also had older age at diagnosis, later stage of disease, were less likely to be on ART, and have history of injection drug use (associated with other causes of mortality). We observed the higher mortality rate in men in all age groups and during the whole period of follow-up.
The mortality of HIV-infected patients in the first year of ART in low- and high-income countries has been reported as 5.5 and 2.0 per 100 person-years, respectively. 10 Our observed mortality rate of 7.0 per 100 person-years is therefore considerably higher than high-income or even low-income countries. Part of this may be explained by differences in the patient populations. Our study subjects included all infected patients and were not limited to those on ART. Nonetheless, such a high mortality rate can be prevented by diagnosis of patients at earlier stages of disease and initiating infected patients on treatment as soon as possible. These should also be addressed by updating national ART guidelines to be more in line with earlier initiation, if not initiating all patients.10–12
Brinkhof et al. 12 in their study of 5491 HIV-infected patients on ART in 15 treatment programmes in Africa, Asia, and South America report that 3.8% of patients were not seen after their first visit and 16% were lost in the first 6 months of follow-up. Based on our data, we lost one in five patients after the first visit, increasing to one in three by 6 months. This high level of loss to follow-up might be explained partly by the nature of IRCHA as a referral centre serving the whole country. Patients may just receive their first visit and then subsequently return or are linked to other treatment centres located close to their residential area. In our records, however, we found no data indicating such linkage taking place. To the extent that this process might occur, loss to follow-up may be over-estimated, although we have no way to adjust for it. Considering the fact that IRCHA, in comparison to other peripheral centres, have better resources and capacities to record and follow registered patients, loss to follow-up might be even higher in other centres. These possibilities need to be carefully assessed within and across other centres providing ART services in Iran. Meanwhile, effective interventions to improve adherence and linkage to services are required. The first step could be a systematic assessment of (individual, structural, and contextual) factors associated with poor adherence among HIV-infected patients, not only in the capital city but also in other periphery centres in Iran.
Taken together, we conclude that HIV care and treatment needs to be substantially improved in order for Iran to realize the full benefits of the latest advances. Men in particular may face barriers to early diagnosis and care. For example, those who inject drugs, are in prison, and not in a marital relationship may also pay less attention to their health, are less likely to test for HIV, less likely to be treated for HIV when diagnosed, and less likely to have good adherence when treated. Similar factors may result in less-effective diagnosis and treatment of tuberculosis.
We acknowledge the limitations of our study. We did not have access to all predictors for all of the 1495 cases. As a result, the sample size and power were low for the more detailed analysis. The medical records also had very limited details of other factors that may be associated with mortality. Moreover, we had collected data on first CD4 and presence of advanced stages of disease at first visit to IRCHA. These might be different from those measured at the time of diagnosis.
Nonetheless, our snapshot of mortality provides a rare and rapid assessment of the survival situation of persons with HIV/AIDS in the region. We observed that the early loss to follow-up of the patients initiated on ART is very high. We identified that male mortality is higher than that of women and ought to be addressed by interventions to increase HIV testing in populations of men at risk, perhaps starting with those in incarceration or substance use treatment. In addition to serving as a call for re-invigorating HIV prevention and care in Iran, our analysis highlights the need for rigorous longitudinal studies in order to better understand and help achieve the maximum level of the benefits of care and treatment already enjoyed by other countries.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.