
Abstract
As a concentrated epidemic, human immunodeficiency virus (HIV) is spreading rapidly in one or more groups in Iran, but in the general population its prevalence is relatively low. Female sex workers (FSWs) and their partners are at greater risk for HIV infection. To determine the prevalence of HIV and sexually transmitted infections (STIs) including gonorrhoea, Chlamydia, herpes simplex type 2 and syphilis among FSWs. We conducted a cross-sectional study of 278 FSWs in Shiraz, by using respondent-driven sampling, from June to March 2010. The recruitment chain started with 14 seeds, and FSWs were tested for HIV, syphilis, herpes simplex type 2, gonorrhoea and Chlamydia. HIV prevalence was 4.7% (13/278); the most prevalent STI was herpes simplex type 2, 9.7% (27/278), followed by Chlamydia 9% (25/278), gonorrhoea 1.4% (4/278) and syphilis (0/278). The FSWs reported drug use (69.9%) of which 16.4% had history of injecting drug use. Unprotected sex in the past month was reported by 24.4% of FSWs. Urgent education and risk reduction programmes are needed in this population.
Keywords
Introduction
Human immunodeficiency virus (HIV) continues to be a challenging pandemic which involves more than 30 million people worldwide. More than 95% of the infections have been reported from low-to-middle income countries since 2003. Reports from 135 countries show that 97 (71.8%) of such countries are afflicted with low or concentrated epidemics. According to a UNAIDS report, for every two subjects who start on antiretroviral therapy (ART), there are five new infections. 1
As a concentrated epidemic, HIV is spreading rapidly in one or more sub-groups of injecting drug users (IDUs), prisoners, sexual partners of IDUs and female sex workers (FSWs), and men who have sex with men (MSM), but in the general population, its prevalence is relatively low. The crucial threat posed by high-risk populations is bridging the concentrated epidemic to a more widespread population. FSWs and their partners are at greater risk for HIV infection. The sexual partners of FSWs, acting as a bridge, can spread HIV to the general population. Prevention programmes should focus on this epidemiological bridge. A successful comprehensive HIV surveillance programme should include surveys of HIV and sexually transmitted infections (STIs) prevalence and risk behaviours. 2 Previous work has confirmed the association between STIs and HIV acquisition. 3 STIs substantially affect populations with a low prevalence of HIV, thereby enhancing its dissemination. 4
In this context, a study reported from Panama showed the prevalence of HIV in FSWs to be 0.7%, and in regard to STI, the prevalence of antibodies to syphilis and herpes simplex type 2 (HSV-2) were 3.8% and 74.2%, respectively. 5
Another study on genital tract infection prevalence, among FSWs, showed HSV-2 80.1%, syphilis 9.4% and HIV 2.4%. The prevalence of condom use with client and husband/regular partner were 98.3% and 7.3% respectively. 6
The two recent surveys reported HIV and STIs prevalence by using respondent-driven sampling (RDS). The first study showed HIV and syphilis prevalence in Somalia as 5.2% and 3.1%, respectively. 7 The second investigation conducted on 596 FSWs revealed the prevalence of HIV, syphilis, gonorrhoea and Chlamydia in Kenya as 29.3%, 0.9%, 3.1% and 1.1%. 8
Another study reported from Moscow on FSWs showed 4.8% HIV prevalence of which 31.3% had at least one STI accompanied by HIV. 9
The two most recent regional studies among FSWs were from South India and Afghanistan. In southern India, the initial prevalence of HIV, syphilis, Chlamydia and/or gonorrhoea were 19.6%, 5.9% and 8.9%, respectively. A preventive patient education programme associated with FSWs improved condom use from 66.1% to 84.1% for repeat clients and from 82.9% to 88.0% for occasional clients but it remained unchanged for regular partners (32%) in connection with their last intercourse. Prevalence of HIV, syphilis, Chlamydia and/or gonorrhoea changed to 16.4%, 3.4%, 7.0%, respectively, after an educational programme. 10 The second study from Afghanistan with 520 FSWs reported the prevalence of HIV as 0.19% with no cases of syphilis. 11
According to a bio-behavioural survey of various populations in Iran, HIV prevalence among IDUs was 15% across the country, which was highest in Tehran, Fars and Lorestan provinces. HIV prevalence among sex partners of IDUs was 3.7% around the country; 10.8%, 4.6% and 0%, in Shiraz, Tehran and Mashhad cities, respectively. The prevalence among FSWs was 4.5% throughout country and differed from one province to another (0–28%), with the highest number reported from Kermanshah and Hormozgan provinces. The prevalence among FSWs with a history of drug injection was 13%. 12
Currently in Kerman, a mid-size city in Iran, HIV and STIs prevalence among 177 FSWs determined by RDS was 7.2% for syphilis and 18% for HSV-2. No cases of HIV were detected. In that study, 17% of FSWs did not use a condom at last intercourse with a commercial partner. However, the prevalence was 22% with their non-paying partners. 13
In Iran, the AIDS epidemic is a complex integrated epidemic involving subgroups of IDUs, partners of IDUs, prisoners and more recently FSWs. According to a report in 2010, 20.8% of new cases were sexually transmitted, which is significantly higher than previous years. The trend is toward sexual transmission. Currently national AIDS programmes are oriented toward the new high-risk key population of FSWs, 13 which is the subject of our study.
On this basis, prevalence of HIV and STIs (gonorrhoea, Chlamydia, HSV-2 and syphilis) was studied among FSWs by using RDS in Shiraz, the capital city of Fars province, in order to plan appropriate interventions.
Materials and methods
Sampling methodology
We designed a cross-sectional study by using RDS to recruit 278 FSWs in Shiraz, south of Iran, from June 2010 to March 2011. The National Ethics Committee approved the survey. RDS is used for hidden populations with high-risk behaviours (IDUs, FSWs and MSM). This method eliminates non-random selection bias.
The FSWs who were 17 years or older and had performed sexual intercourse for money, drugs or other goods for at least six months during their lifetime or at least once within the last 12 months were recruited in this research. Three centres were chosen from different parts of the city. The centres started working simultaneously for better accessibility. Our study started with 14 seeds with maximum eight waves. Three seeds did not recruit additional participants. The number of waves for the other 11 seeds ranged from one to eight waves. We considered FSWs as a finite population, so a sample size of 395 was calculated. Finally, the 11 remaining seeds recruited 278 FSWs. Overall, the equilibriums with respect to the HIV prevalence were obtained during 10 months.
Consenting participants completed a face-to-face interview, and after completing the interview, seeds received a monetary incentive. These women also received another incentive for each referred participant who qualified and completed the study. Participants interested in serving as a peer recruiter received three recruitment coupons. At the end of the interview, a free gynaecological examination was done by a midwife. The questionnaire consisted of questions about socio-demographic information, history of sexual contact, drug and alcohol use, knowledge and attitude about HIV and STIs.
After the participants responded to questions about HIV/STI risk behaviours, blood samples were collected from them for testing HIV, syphilis and HSV-2, along with vaginal swabs for testing Chlamydia and gonorrhoea.
We checked the study samples for independency by using a unique code in their coupons and participants were not permitted to participate more than once in the study.
Laboratory procedures
Blood samples and vaginal smears were delivered within 1–2 hours to the Microbiology laboratory of Shiraz Medical School. Serum was separated from blood samples and half of that was used for serologic testing of herpes simplex type 2, based on the detection of IgM antibodies by sandwich Elisa kits (IBL, Germany). The other half of serum samples was frozen at −20℃ and once a week sent to the Blood Transfusion Bureau for HIV and syphilis tests. The serum samples were tested for HIV by enzyme-linked immunosorbent assay (ELISA) (Blott MP, USA) and the results were confirmed by Western blot assay (BioMérieux, France). All participants were tested for syphilis using VDRL test (Bionic, Iran) and positive samples were confirmed by FTA-ABS (Euro immune, Germany).
Vaginal samples were tested for Chlamydia trachomatis by polymerase chain reaction (PCR) using specific PCR kits (Genekam, Germany). To detect Chlamydia trachomatis, DNA was extracted (Bioneer, Korea) from vaginal samples and a specific PCR was carried out. Amplified PCR product was assessed electrophoretically by using agarose gel 2% with ethidium bromide staining. All above-mentioned tests were performed according to instruction of kit manufacturers.
Vaginal swabs were also studied for the detection of Neisseria gonorrhoeae by microscopic examination of Gram-stained direct smears and culture in chocolate agar and modified Thayer-Martin selective medium, and finally confirmed by standard biochemical tests.
Data analysis
Data were prepared and entered in Excel software and then imported into RDSAT version 6.01 for descriptive analysis.
Results
Socio-demographic and behavioural characteristics
Demographic characteristics of the 278 female sex workers in Shiraz, 2010.
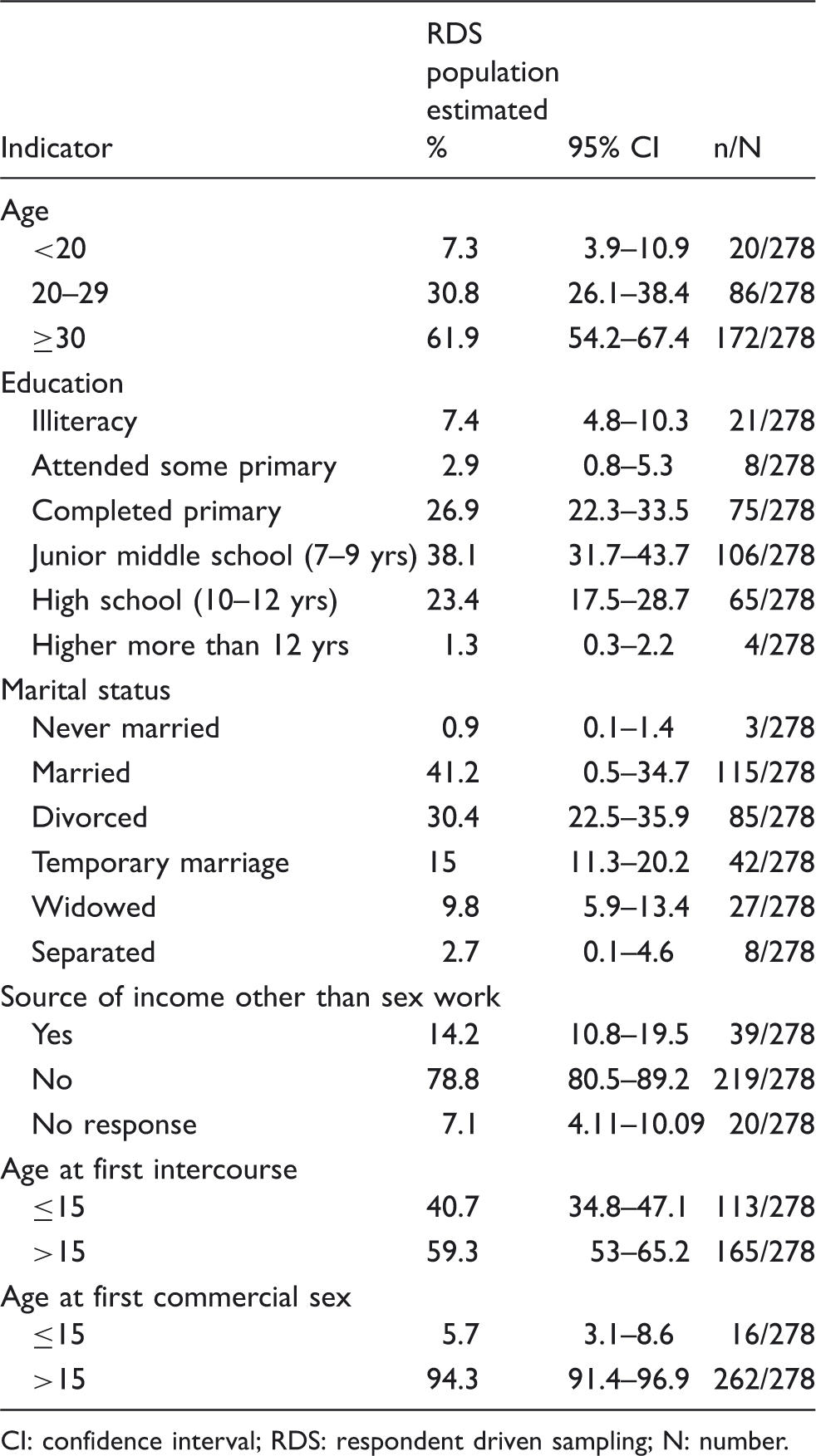
CI: confidence interval; RDS: respondent driven sampling; N: number.
Condom use with clients and non‐paying sex partners among 278 female sex workers in Shiraz, 2010.
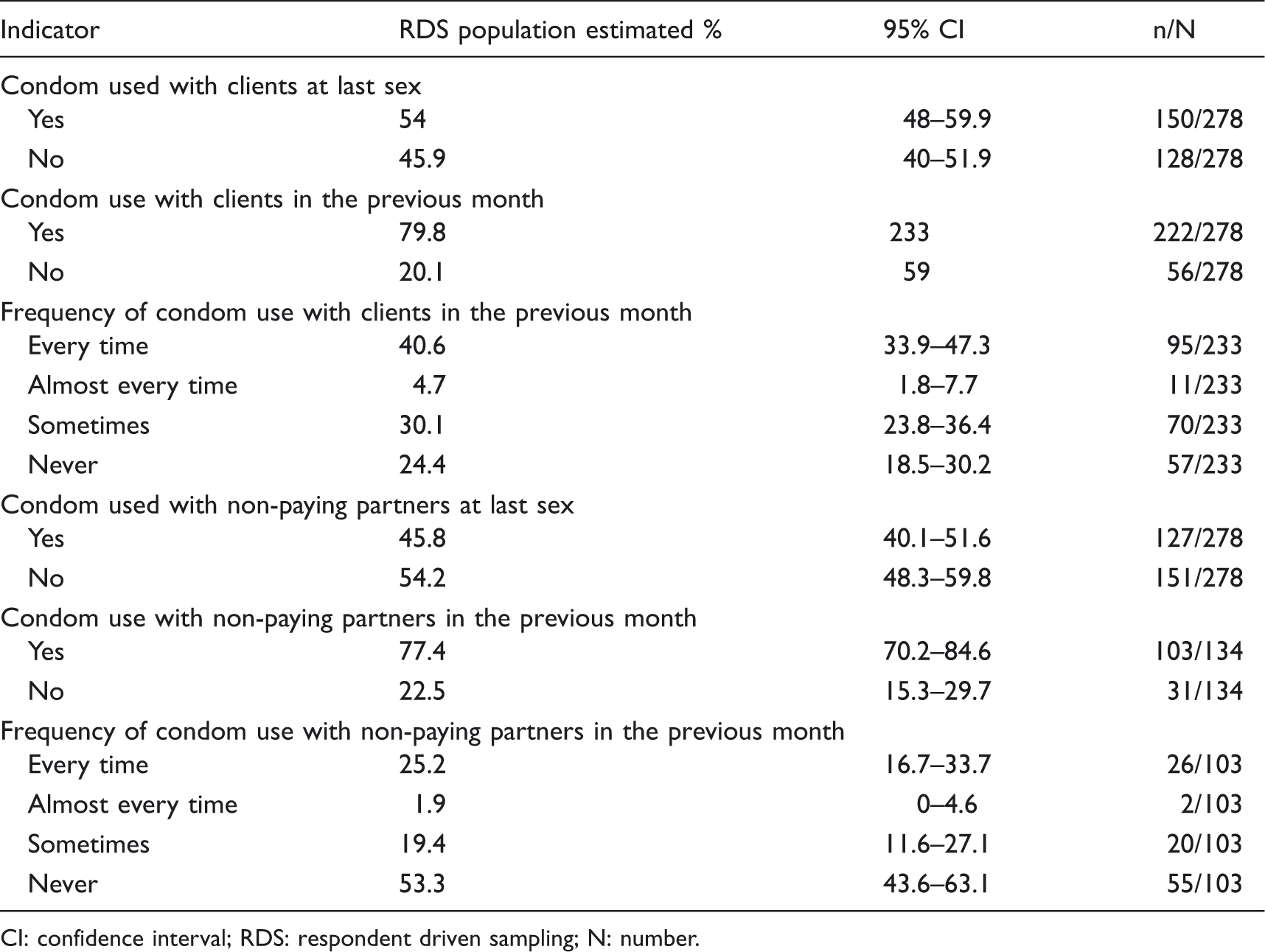
CI: confidence interval; RDS: respondent driven sampling; N: number.
Knowledge about STI symptoms, self-reported symptoms and treatment-seeking behaviours among 278 female sex workers in Shiraz, 2010.
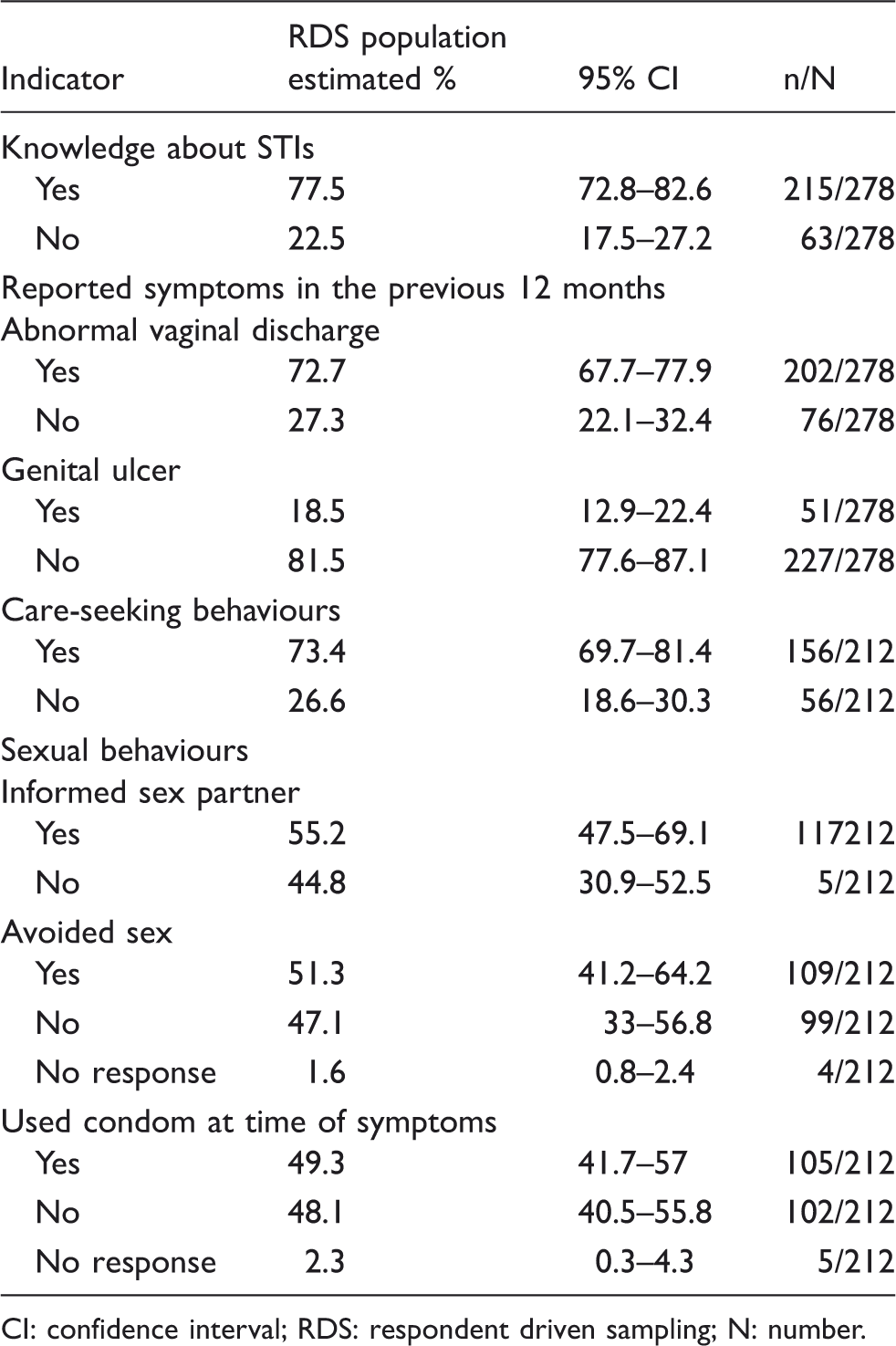
CI: confidence interval; RDS: respondent driven sampling; N: number.
Drug abuse
The FSWs reported a history of drug abuse (69.9%) and among them, 16.4% had history of drug injection. Of these, 4.3% used unsterile needles; 43.8% used drug and alcohol together; 13.7% of them used only alcohol, as whole 57.6% consumed alcohol.
HIV and STIs prevalence
HIV prevalence was 4.7% (13/278); but in respect of STIs, the most prevalent was HSV-2, 9.7% (27/278) followed by Chlamydia, 9% (25/278), gonorrhoea 1.43% (4/278) and syphilis (0/278). Two subjects tested positive for syphilis for RPR but were not confirmed by FTA-ABS.
Association of HIV with socio‐demographic and behavioural characteristic among 278 female sex workers in Shiraz, 2010 – results from logistic regression.
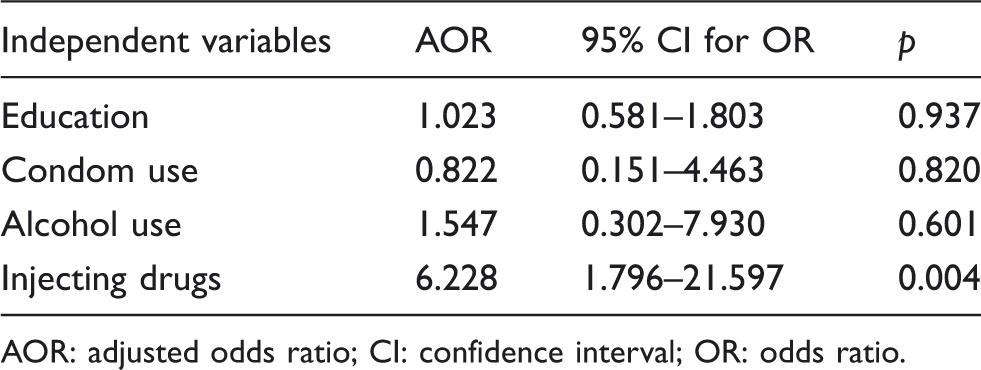
AOR: adjusted odds ratio; CI: confidence interval; OR: odds ratio.
Discussion
The number of HIV cases in Iran was estimated to be 89,000 and 106,000 for 2009 and 2014, respectively. As estimated, 7000 new cases emerge annually. The main groups infected by HIV in 2009 were a low-risk population, presumably via unprotected sex. Modeling HIV/AIDS showed the pattern of transmission will change from unsafe injection to unprotected sex. 14
The 2010 bio-behavioural survey reported HIV prevalence among different populations in Iran. Fars was one of the provinces with highest prevalence among IDUs in Iran. The prevalence of HIV/AIDS among sex partners of IDUs was highest in Shiraz among the cities where the study was conducted (10.8%). The prevalence among FSWs differs from province to province (0–28%) with an estimated mean 4.5% across the country. A rising prevalence of HIV/AIDS among FSWs (13%) was reported, based on the history of injecting drugs. 12
Our study showed high prevalence of HIV among FSWs, which was identical to the estimated mean by the bio-behavioural survey. HIV is higher among sex workers than the general population in Iran. This group has the potential to convert a concentrated epidemic to a more widespread one through their clients. 12
In contrast to syphilis and HSV-2, the prevalence of HIV was higher in Shiraz than in Kerman. As indicated by the history, IDU and unprotected sex with commercial partners was lower and higher among FSWs in Shiraz than in Kerman, respectively. 13 IDUs and sex partners of IDUs had the highest infection prevalence in Shiraz. 12 Talbott claimed that the prevalence of HIV among sex workers in a country could explain HIV prevalence levels across countries. 15 FSWs are associated with other high-risk groups such as IDUs and the general population.
Our study showed a higher prevalence of HIV compared with a study from three cities in Afghanistan. Syphilis was not detected in either studies. 11 Although higher reports of condom use and treatment-seeking behaviour were seen, higher rates of drug use and IDU were reported among the participants in our study compared to that in Afghanistan.
A survey from China, the most populated country in the world, showed no case of HIV among participants but higher levels of syphilis and gonorrhoea and a lower level of Chlamydia compared with our study. This also indicates that transmission of HIV from IDUs to FSWs depends on IDU FSWs and those who have IDU partners. In that study, no cases of HIV and IDU were reported, although a high prevalence of STIs was found due to risky behaviours. Condom use with paying clients and non-paying partners was higher than in our study, but the rate of consistent condom use was low. 16 We emphasize that injecting drug use and inconsistent condom usage are two important predictors of HIV/STIs prevalence among FSWs.
The prevalence of HIV and syphilis in Somalia was higher than that of our study. This is described by the high number of sexual contacts and low awareness in Somalia. 7 HIV, syphilis, gonorrhoea prevalence among FSWs in Nairobi were higher, but that of Chlamydia was lower than in our study. 8
Another study showed higher prevalence of HIV, gonorrhoea and Chlamydia compared with our study. 17
HIV prevalence in Moscow was almost identical with that of our study, but other STIs including Chlamydia, syphilis and gonorrhoea were higher. 9 We found an association between IDU and HIV, although in Moscow IDU was not associated with STIs/HIV. 9 But this association was reported in another investigation. 18
A study from south India reported a high prevalence of HIV, syphilis and gonorrhoea before intervention in which a HIV prevention programme reduced HIV and STIs prevalence and increased condom use by commercial clients. This interventional experiment indicated a high level of coverage and condom usage by follow-up time. 10
RDS was used to recruit FSWs in this study. RDS is the generalized form of snowball sampling. However, snowball sampling is a non-probability sampling method; one of the advantages of the RDS method is that it supplies more externally valid probability samples. A major advantage of RDS is that it does not need a comprehensive mapping process.
Data collection during RDS proceeds through successive ‘waves’ until the sample reaches ‘equilibrium’ with regard to the measured variable. ‘Equilibrium’ can be interpreted as a stage in which estimates that integration around a field of sampling is stable that does not change during successive recruitment cycle. 19 In our study, we reached to equilibrium with respect to HIV prevalence (4.7%) in FSWs after 10 months.
This is the first descriptive study on FSWs in Shiraz to assess the prevalence of HIV/STIs. It contains socio-demographic information, high-risk behaviours that could lead to future interventional research. The subjects were from hidden populations in Iran, that because of cultural and religious limitations were difficult to access. However, our interviewer was selected from persons with strong communication skills in recruiting participants and attracting their cooperation. This study has some limitations. In the beginning of the study, monetary incentive was little; so referred FSWs were from low economic levels that needed more money. Then we increased the monetary incentive and we recruited FSWs from all classes. Due to official holiday during the project, we encountered slow progression. The temporal relationship between dependent and independent variables is difficult to provide by a cross-sectional study. We recommend a cohort study among FSWs.
Our results underline the urgency of implementing a preventive intervention programme. The results will be helpful in planning future harm reduction programme. According to a survey, knowledge and attitudes of FSWs towards STIs and protective sex are still insufficient. 20 Educational programmes on mode of transmission of HIV/STIs, STI syndromes and HIV/STIs counseling, testing and reproductive healthcare should be included in FSW-oriented programmes.
Despite our awareness about some existing limitations in approaching this high-risk group, their presence could not be overlooked in our country. Firstly, the aim of an educational programme is to increase knowledge and improve the attitude of FSWs about high-risk behaviours and their association with STIs and HIV. Secondly, such improved knowledge and attitudes must be sustainable and reflected in practice. The capacity of FSWs to demand consistent condom use will be fulfilled through an efficient educational programme. Appropriate environments should be created to provide empowerment for FSWs to protect themselves, sexual partners and the general public.
Conclusions
According to the results of this study, the necessity of implementing preventative intervention programme is an urgent issue. Educational programmes on mode of transmission of HIV/STIs, STI syndromes and HIV/STIs counseling, testing and reproductive healthcare should be included in the FSW-oriented programmes.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.