
Abstract
The burden of HIV/AIDS in China has been disproportionately concentrated in Yunnan Province, where in Dehong prefecture, the HIV prevalence rate among pregnant women reached 1.3% in 2003, a rate that is indicative of a generalized epidemic. Since then, there have been extensive efforts to expand prevention to reduce mother-to-child transmission (MTCT) in this high-prevalence region. These intensified MTCT reduction efforts and their impact on MTCT are yet to be examined. We described the changes in access to HIV screening and antiretroviral therapy (ART) among pregnant women from 2005 to 2010 in this region and the corresponding reduction in MTCT over this period. Between 2005 and 2010, the annual number of pregnant women screened for HIV in Dehong Prefecture more than doubled. The proportion of pregnant women screened for HIV rose from an estimated 15–20% to 99.8%, and the proportion of HIV-infected pregnant women receiving ART increased from 63% to 99%. We estimate that the proportion of children born with HIV to HIV-infected mothers decreased from 15.4% to 7.2% over this period. Sustained low-level MTCT following comprehensive interventions in this region is encouraging. Over the last decade, comprehensive PMTCT efforts, coupled with national and local government policy support in this area appear to be effective.
Keywords
Background
According to China's HIV/AIDS Prevention and Control Joint Evaluation Report, there were an estimated 780,000 surviving people living with HIV/AIDS (PLWHA) in China as of the end of 2011 and 28,000 HIV/AIDS-related deaths in 2011. It is estimated that approximately 1.1% of PLWHA and 0.8% of HIV/AIDS-related deaths were due to infections from mother-to-child transmission (MTCT). 1
In 1989, the first indigenous AIDS cases were reported as an outbreak in 146 infected heroin users in Dehong prefecture, Yunnan province. Subsequently, HIV spread steadily from this province into neighbouring areas and along the major drug trafficking routes, then from injecting drug users (IDUs) to their sexual partners and children. The first case of MTCT was reported to the Chinese Center for Disease Control and Prevention (CDC) in Yunnan province in 1995.2,3 Data from China CDC reports have shown that the proportion of reported cases of HIV and AIDS attributed to MTCT has increased from 0.1% in 1997 to 0.4% in 2002. 4 Meanwhile, studies have shown a high prevalence of HIV infection among children born to HIV-infected mothers in certain areas of China, especially in Yunnan province (HIV prevalence reached 34%). 5 The burden of HIV/AIDS in China has been disproportionately concentrated in Yunnan Province, where in certain areas, such as Dehong prefecture, HIV prevalence rates among pregnant women has reached 1.3% in 2003, a rate that is indicative of a generalized epidemic. 6
Since then, this prefecture has become the epicentre with the most severe HIV epidemic in China and attracted a considerable level of attention, both domestically and internationally.7,8 Over the last decade, there have been extensive efforts to expand interventions to reduce MTCT in this high-prevalence region.
9
In 2004, expansion of prevention of mother-to-child transmission (PMTCT) services was initiated in Yunnan province and Dehong prefecture through ‘The First Round of Implementation Plan for Combating HIV/AIDS (2005–2007),’ which sought to increase access to antiretroviral therapy (ART) among HIV-infected pregnant women to 90%, alongside increasing access to HIV testing services in this population. After 2004, HIV screening of pregnant women in Dehong Prefecture was expanded across Women and Children’s hospitals at both the county and prefectural level. Then, these efforts were further strengthened by the Yunnan AIDS Prevention and Control Act passed in 2007, which made provisions for access to free HIV screening for all pregnant women, and subsequent waves of funding and infrastructure development for expansion of PMTCT services. In 2007, ‘The Second Round of Implementation Plan for Combating HIV/AIDS (2008–2010)’ was issued. In this programme, PMTCT work was required to be added to local routine Mother and Children’s Health (MCH) work and it set an even more ambitious goal – to expand treatment coverage among HIV-infected women to at least 98%.10,11 Followed by this programme, a series of policy and technical guidelines have been continuously issued. These include ‘The PMTCT Work Guidance Manual in Yunnan Province’, ‘The Assessment Framework and Indicators System For PMTCT Work in Yunnan Province’, ‘Mother and Child Health Services Manual in Yunnan Province’, ‘PMTCT Data Quality Control Programme in Yunnan Province’, and ‘Ten Action Plans For AIDS Prevention and Control Work in Yunnan Province’ (see Figure 1). The specifications emphasize the key aspects of PMTCT work in Yunnan province, such as health education, HIV testing during the early period of pregnancy, prevention and referral, preventive antiviral therapy of MTCT, care and support, HIV maternal and infants’ follow-up, staff training, family planning, supervision and evaluation, and data quality control.
Temporal relationship between key HIV policy documents issued and HIV MTCT rate in Dehong prefecture, 2004–2010.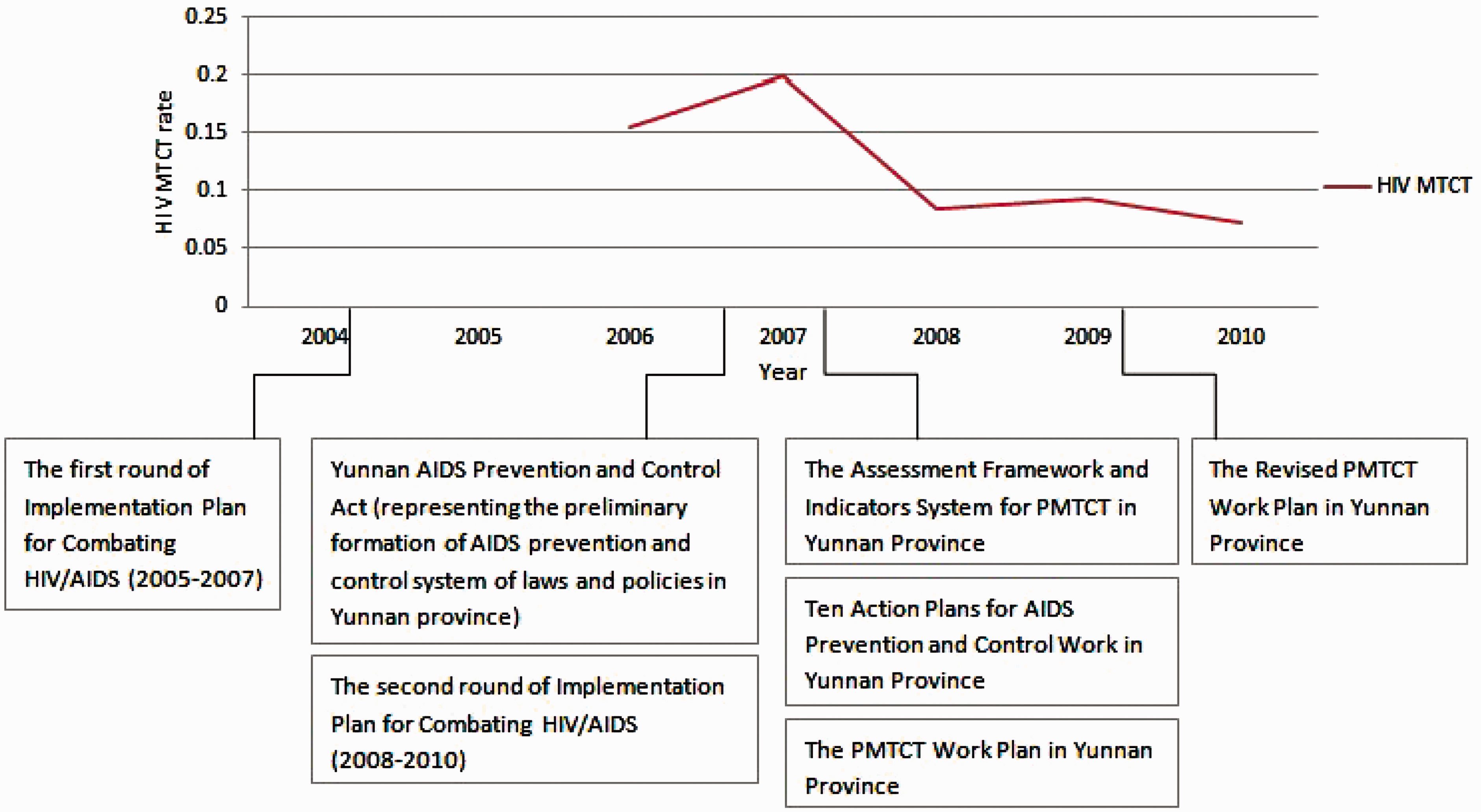
These intensified MTCT reduction efforts and their impact on mother-to-child-transmission rates in this region are yet to be examined. We describe changes in access to HIV screening and ART among pregnant women from 2005 to 2010 in Dehong Prefecture in Yunnan Province, China and the corresponding reduction in mother-to-child HIV transmission over this period.
Materials and method
Data sources
Data were first obtained from the National HIV/AIDS Comprehensive Response Information Management System (CRIMS). 12 This unified, web-based platform includes subsystems, such as HIV/AIDS Case Reporting, HIV Testing and Counseling, HIV Sentinel Surveillance and ART for Adults, etc. Then, data were linked to the local obstetric surveillance network maintained by local CDCs. Local pregnancies in women with diagnosed HIV and children with HIV infection and infants born to infected women were notified through this active obstetric surveillance network. As Dehong prefecture has attracted a considerable level of attention, its obstetric surveillance network was built early from 2003, and seven related health centres were reported to this network, including four maternal and child health centres, two comprehensive hospitals and one antenatal clinic in Dehong prefecture, which could cover over 90% HIV-infected women giving births in this region from 2005 to 2010. HIV-infected women giving birth at home or other places were not included in the surveillance network.
HIV counseling and testing
Follow-up services, including counseling and testing were provided for HIV-positive women before, during, and after delivery. A woman was considered to be HIV-infected if she was screened HIV-positive, and then confirmed by Western Blot or two positive ELISA tests (enzyme-linked immunosorbent assay, Vironostika HIV Uni-Form plus O, BioMerieux, Holland). All respondents had been notified of their HIV-positive status, and were entered into the obstetric surveillance system between 2004 and 2010. HIV antibody test was given to infants at 18 months, and a child was considered to be HIV-infected if he or she: (a) had two or more blood specimens that tested positive for HIV by ELISA tests; or (b) had one or more specimens that tested positive by two different assays (e.g. enzyme immunoassay or rapid test), drawn at age 18 months or greater; or (c) died and a diagnosis of HIV had not been excluded by laboratory tests. Infants were tested by an HIV viral load (VL) assay at 1–3 months after birth (35–180 days, with 93 days in average).
Drug regimens
Before 2005, HIV-infected pregnant women were asked to take nevirapine (NVP) at onset of the labour (200 mg) and the infants took single-dose NVP in 24–48 h after birth (2 mg/kg, ≤6 mg). If the pregnant women gave birth in 2 h after taking NVP, the newborn received its first oral NVP in 60 min after birth, and the second oral NVP at least 48–72 h after birth. In the case of cesarean section, the pregnant women took NVP (200 mg) in 24 h prior to the operation. After 2005, HIV-infected pregnant women were asked to take zidovudine (AZT) + lamivudine (3TC) + NVP (CD4 < 250 cells/mm3), or AZT + 3TC + EFV (CD4 > 250 cells/mm3) after 3 months' pregnancy; and children were required to take AZT + 3TC + NVP. Among them, the infants with a body surface area at 160 mg/m2 were asked to take AZT every 8 h (newborns over 90 days); infants with a body weight at 4 mg/kg were prescribed 3TC twice a day (newborns over 30 days); infants with a body surface area at 120 mg/m2 were prescribed NVP once a day and treated for 14 days (newborns over 60 days), and children less than eight years took NVP at 7 mg/kg, every 12 h while children older than eight years took NVP at 4 mg/kg, every 12 h.
Maternal ART in pregnancy was categorized as none, monotherapy, dual therapy and HAART (three or more drugs); only antepartum treatment was considered in this analysis. The vertical transmission rate is the number of infants infected amongst the infants born to HIV-infected mothers, regardless of type of therapy or mode of delivery.
Infant feeding
While all women were counseled antenatally about infant-feeding options, uninterrupted access to six months’ commercial infant formula was offered free through the national and international PMTCT programmes in this region from 2005, which was expected to result in the lowest risk of disease and death. HIV-infected mothers could choose to access this supply any time in the first 12 months of the infant’s life. For those initiating formula milk from birth, an initial supply was provided antenatally.
Data analysis
As data were collected in paper forms in 2004, they were entered into the web-based system by local level public health workers. Data collected from 2005 to 2010 were directly reported to the system. Maternal sociodemographic and health information was recorded, and key variables in the collected data include: number of pregnant women registered, number of pregnant women screened for HIV, number of HIV-infected pregnant women, number of HIV-infected pregnant women on ART, ART regimens, time of receiving ART, number of live births, number of infected infants born to HIV infected mothers. Statistical analysis was carried out using SPSS 13.0 (SPSS Inc., IL). Data from 2004 to 2010 were analyzed and shown in absolute numbers and proportions.
Results
Access to HIV testing among pregnant women between 2005 and 2010
Proportion of pregnant women screened for HIV in Dehong Prefecture, 2005–2010. a

Total number of pregnant women and pregnant women screened for HIV included women with multiple pregnancies during years 2005–2010; for example, women with three pregnancies were recorded as three pregnant women. ‘–’ indicates that the necessary data were not collected.
Access to ART among pregnant women between 2005 and 2010
Proportion of pregnant women who knew their HIV infection status and women who received antiretroviral therapy (ART) in Dehong prefecture, 2005–2010.

The outcomes and access to ART among children born with HIV to HIV-infected women in Dehong prefecture, 2005–2010
The outcomes of children born to HIV-infected women in Dehong Prefecture, 2005–2010.


Rate of children receiving ART prophylaxis in Dehong prefecture, 2006–2010.
The estimated mother-to-child HIV transmission between 2005 and 2010
Estimated proportion of children born with HIV to HIV-infected women in Dehong Prefecture, 2006–2010 a

The numerator: (Estimated Number of HIV-Infected pregnant women − Reported Number of HIV-Infected pregnant women detected through testing + Reported number of HIV-infected pregnant women who were not on ART) × 34.8%+Reported Number of HIV-Infected pregnant women detected through testing × Proportion of children born with HIV to HIV-infected pregnant women on ART; The denominator: Number of live births × HIV prevalence among pregnant women. 13
The estimated rate of HIV infection of the children born to HIV-positive mothers who have not taken any preventive measures.
Discussion
Our study reveals that between 2005 and 2010, there were concerted efforts to increase access to HIV screening and ART to reduce mother-to-child HIV transmission; nearly universal HIV screening and treatment coverage was attained among pregnant women. We estimated a two-fold decrease in mother-to-child HIV transmission over the same period. Though mother-to-child-HIV transmission remains high at 7.2%, our findings support that owing to expanded HIV testing coverage, timely effective ART and appropriate management of delivery, and related policies in local areas, the transmission could be reduced enormously,14–16 which we believe will continue to be feasible given the vast infrastructure for HIV screening and linkage to treatment and care for this population in this area that has been developed over the last decade.
Sustained low-level mother-to-child-HIV transmission following comprehensive interventions in this hardest-hit region by HIV is encouraging. The issued policies and guidelines, current testing strategy, options for treatment in this area appear to be effective. It is indicated that the two rounds of large-scale action plan for combating HIV/AIDS (2007–2010, 2008–2010), coupled with aggressive national and local policies, may have contributed to the significant reduction in MTCT in this region. Meanwhile, there may be also other factors that can explain the reductions in HIV MTCT, such as the increased financial and technical support from the central, provincial and prefectural government, the strong presence of local and international HIV/AIDS organizations in Yunnan, the well-trained local experts and public health workers. The HIV MTCT reduction could not be attained unless these factors combined.
One of the limitations of our study was selection bias. The study respondents included in the database were registered participants who were already willing to participate in routine health check-ups and HIV testing services. Our study did not include those HIV-infected women giving birth at home or other places; as this proportion is small, we included those non-reported number of infected infants in the estimation and calculation of HIV MTCT. In addition, as the study time was from 2004 to 2010, there were situations when cases got lost of follow-ups, and when drug regimens changed slightly over the years; this might influence the overall estimation. However, it was predicted that with further increased access to screening and linkage to HIV treatment and care among pregnant women and newborns and sustained levels of coverage, over time mother-to-child HIV transmission could be further reduced in this region and perhaps eventually eliminated, as has been achieved in other settings globally.17–19
More evaluation programmes of the prevention efforts in this area should be implemented and focus on specific programmatic elements along the testing and treatment service cascade that can be strengthened and will be critical to sustaining ongoing declines in mother-to-child HIV transmission.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.