
Abstract
We report a case of severe bilateral knee avascular necrosis in a HIV-positive man receiving ritonavir and inhaled fluticasone. This case highlights the need for a thorough medication history in patients on ritonavir-based antiretroviral therapy, especially where multiple prescribers are involved in the patient's care.
Keywords
Case description
A 40-year-old HIV-positive man presented with a three-month history of subacute onset bilateral knee pain and swelling. There was no history of early morning stiffness, preceding trauma, constitutional symptoms, recent intravenous drug use, chronic alcohol abuse or smoking.
His HIV infection, diagnosed in 1996, was well controlled with an undetectable viral load and a CD4 count of 580 cells/µl, on lopinavir/ritonavir 400/100 mg bd, stavudine 40 mg bd and abacavir 300 mg bd. He had received localised radiotherapy eight years previously for Kaposi’s sarcoma, which had resulted in radiotherapy-induced osteodystrophy of the left ankle. His other medical history was notable for mild asthma only.
Clinically, he was Cushingoid with pitting oedema to his knees and bilateral quadriceps wasting. The knees were cool to touch, and there was diffuse joint line tenderness bilaterally. There was a moderate effusion and reduced range of motion in the right knee with no ligamental instability. The rest of the musculoskeletal examination was normal.
The patient’s ESR was 15 mm/h, CRP 6.8 mg/L, with normal renal, hepatic and bone marrow function indices. Connective tissue screening was negative, as were the EPG and IEPG. The serum calcium, phosphate and 25-hydroxy vitamin D3 (tested in autumn) were all within normal range, as were his lipid profile and thyroid function testing. The morning cortisol was undetectable with an ACTH in the normal range at 6.3 pmol/L. A Synacthen stimulation test confirmed adrenal suppression, with a peak cortisol of 450 nmol/L (normal range >550 nmol/L). Gonadal and pituitary function were normal.
Magnetic resonance imaging (MRI) (Figure 1) of the knees showed findings consistent with avascular necrosis (AVN) bilaterally. Bone mineral density readings demonstrated osteopenia.
MRI T1-weighted image of the right knee showing severe avascular necrosis.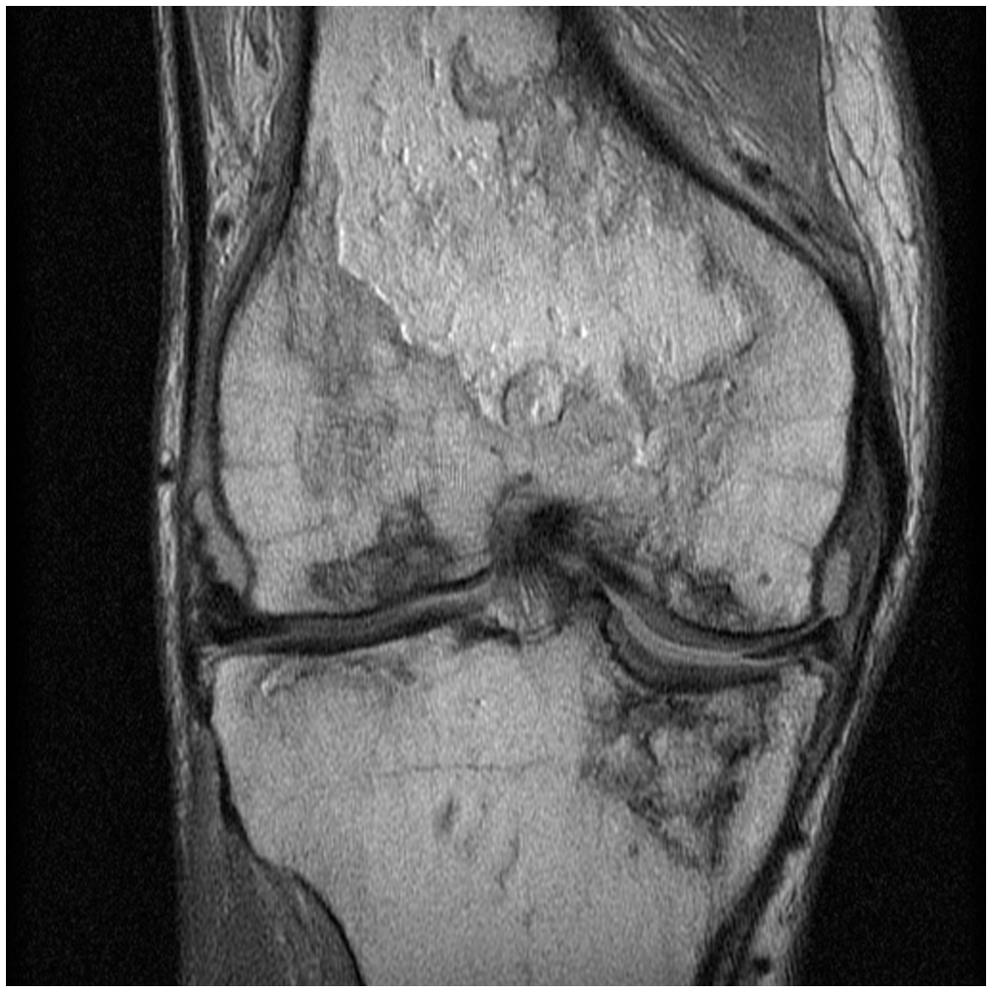
A preliminary diagnosis of excessive exogenous corticosteroid exposure causing Cushing’s syndrome and AVN was made. On revisiting the medication history, the patient recalled that he had been commenced on inhaled fluticasone, 250 µg twice daily, by his general practitioner in the preceding five months for a mild exacerbation of his asthma. The corticosteroid excess was therefore felt most likely due to the significant interaction between ritonavir and fluticasone.
The patient was made non-weight bearing, commenced on cholecalciferol and required significant analgesia. The lopinavir/ritonavir was changed to unboosted atazanavir, and the inhaled fluticasone ceased. However, he developed symptoms of adrenal insufficiency with persistently suppressed cortisol levels, which resolved with weaning doses of corticosteroid replacement.
Discussion
Ritonavir is commonly used for the pharmacokinetic boosting of other protease inhibitors via inhibition of hepatic CYP3A4. Due to extensive first-pass metabolism, 1 plasma concentrations of inhaled fluticasone are usually very low at therapeutic doses; however, this may be augmented via ritonavir inhibition of this pathway. This can lead to the well-described systemic complications of glucocorticoid excess such as iatrogenic Cushing’s syndrome, secondary adrenal insufficiency and osteoporosis. 2 To the best of our knowledge, only one other case of AVN has been reported as being attributed to this interaction. 3
AVN is a rare but disabling condition with a reported incidence as high as 1.3% in some HIV cohorts, 4 contrasting with 0.1% in the general population. 5 A confounding factor in this case is the known association between AVN and HIV. We felt that HIV per se was unlikely to be the underlying cause in this case, given the other clear features of Cushing’s syndrome present at the time of diagnosis. Another potential confounder was the history of radiotherapy; however, areas of avascular necrosis were found well outside the radiotherapy field in our patient. Other known risk factors for AVN were not present in our case, namely smoking, lipodystrophy, hyperlipidaemia, long-term use of systemic steroids and alcohol and the presence of anti-phospholipid and anti-cardiolipin antibodies. 6
Functional outcomes are often poor in patients with AVN, with moderate-to-advanced long-term disability reported in up to 50% of cases some series. 4 The diagnosis is often delayed, as the presenting symptoms may be non-specific and the sensitivity of X-ray imaging is only around 40%.5,6 An MRI is the imaging of choice, with a sensitivity of over 90%, 6 and this should be ordered promptly in those with clinical features and risk factors for AVN.
In HIV-positive asthma patients requiring inhaled corticosteroids, the use of ritonavir-sparing antiretroviral regimens is recommended. 2 Other inhaled glucocorticoids such as beclomethasone and budesonide may be safer alternatives as they are less lipophilic than fluticasone with a much smaller volume of distribution; however, they are also CYP3A4 substrates and have been associated with similar complications.2,7,8 The use of non-steroidal agents (such as oral montelukast) may also be considered.
This case highlights the need for vigilance about the risk of fluticasone-ritonavir interactions. Infectious disease physicians now often serve as the primary care physician for an ageing HIV patient population with non-HIV related co-morbidities and must be familiar with such an interaction. Patients may not identify an inhaled corticosteroid as a ‘medication’ when a drug history is taken. In this case, the treating HIV physician was unaware that fluticasone was being prescribed concurrently by the general practitioner. Good bi-directional correspondence between the HIV physician and other healthcare workers is essential in this era of HIV shared care.
Ethical approval
Not required.
Statement of consent
Patient consented to publication in 2010.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.