
Abstract
The objective of the study was to identify clinical and epidemiological characteristics of patients with infectious syphilis who presented with a high rapid plasma reagin (RPR) titre (≥1: 512) during the year of 2009 at the Miami Dade County Health Department (MDCHD) STD clinic. Potential cases were identified by a search in the electronic database. Among 519 individuals identified with reactive RPR, 190 individuals met criteria for infectious syphilis and 32 of them had at least one RPR titre of ≥1: 512. We found that the majority of individuals with high RPR were men who have sex with men (82%), from ethnic minorities (91%), and HIV infected (75%) but only 3 of them were on antiretroviral therapy. Overall, 50% of these patients with very high RPR titres were symptomatic, and the most common symptom was skin rash (93%).
Introduction
Miami remains one of the epicentres of the syphilis epidemic in the United States. The number of infectious syphilis cases increased from 204 in 2006 to 313 cases in 2009 with 73% of the cases among men who have sex with men (MSM). Among the individuals diagnosed with infectious syphilis in our city, 60% are coinfected with HIV. 1
Diagnostic tools to establish the diagnosis of syphilis are imperfect and diagnosis usually relies on clinical/epidemiological information, and treponemal and non-treponemal tests. Rapid plasma reagin (RPR) is one of the most common non-treponemal tests available and provides both qualitative and quantitative information. 2 Although RPR level does not correlate with disease stage, most cases of infectious syphilis present with levels above 1:8. The significance of very high titres has not been well explored.
The objective of the study was to identify clinical and epidemiological characteristics of patients with infectious syphilis who presented with an RPR titre ≥1:512 during the year of 2009 at the Miami-Dade County Health Department (MDCHD) STD clinic.
Methods
All positive RPR titres of patients seen at MDCHD STD clinic in 2009 were identified in the electronic laboratory database. These tests were performed by the 18-mm circle card test method, by the same group of experienced technicians from the Florida Bureau of Laboratory. Medical records of those individuals were reviewed and collected data included demographics, sexual history, HIV status, HIV treatment and details pertaining to syphilis including symptoms, treatment and follow-ups. Patients were included in the analysis if they had reactive RPR test in addition to positive treponemal test and the clinical diagnoses of primary, secondary, early latent or unknown duration syphilis; primary syphilis diagnosed by darkfield microscopy with negative RPR was also included. Patients were excluded if: (1) RPR represented follow-up serology from prior treated syphilis; (2) Biological false positive RPR; (3) Late latent syphilis. ‘High RPR titre’ included all individuals with an RPR titre ≥ 1:512. Descriptive statistics were used for analysis.
Distribution of RPR values of individuals with infectious syphilis (n = 190).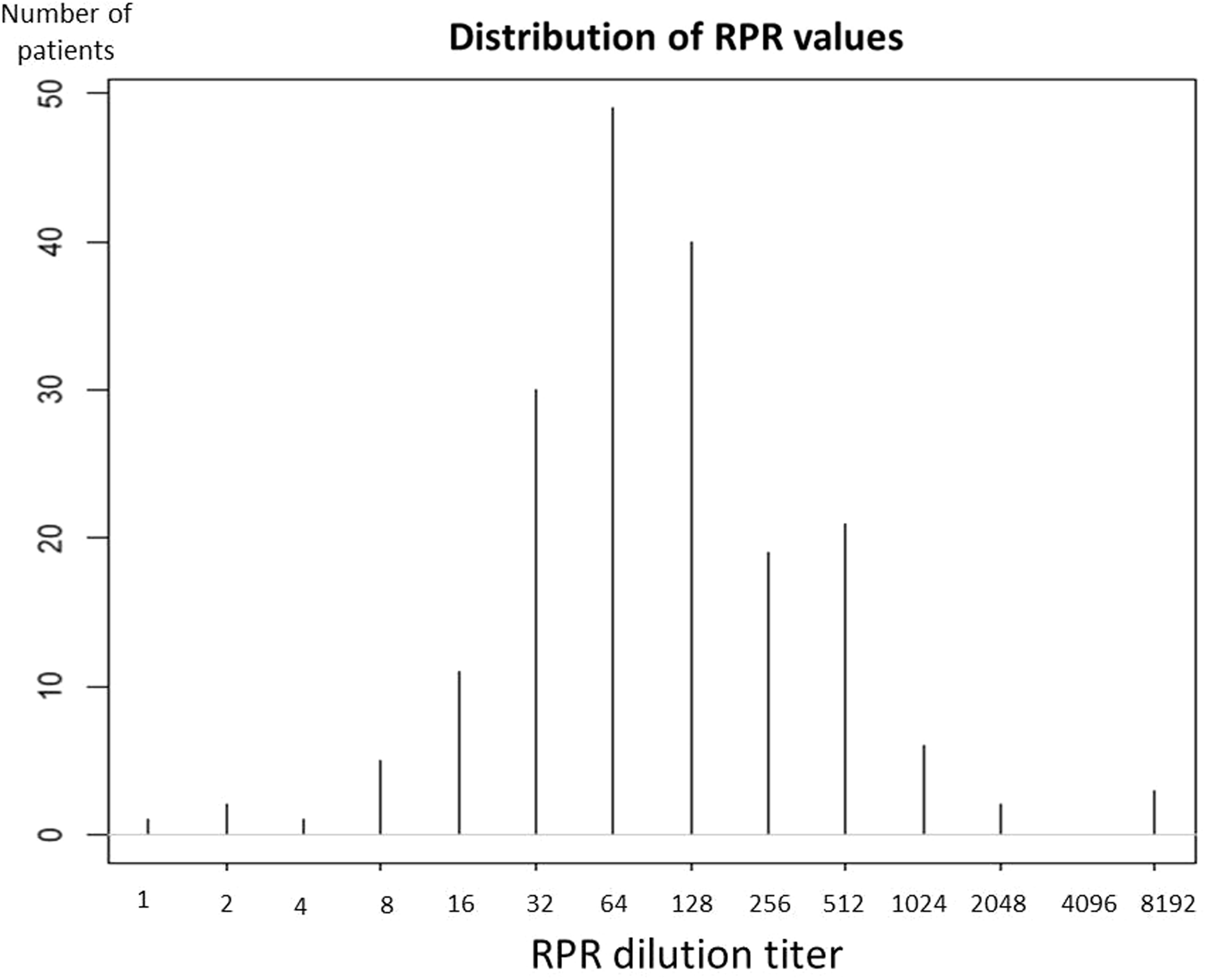
Approval was obtained from both the University of Miami and the State of Florida's Institutional Review Boards prior to implementation of any study procedures.
Results
Demographic characteristics of individuals with very high RPR.
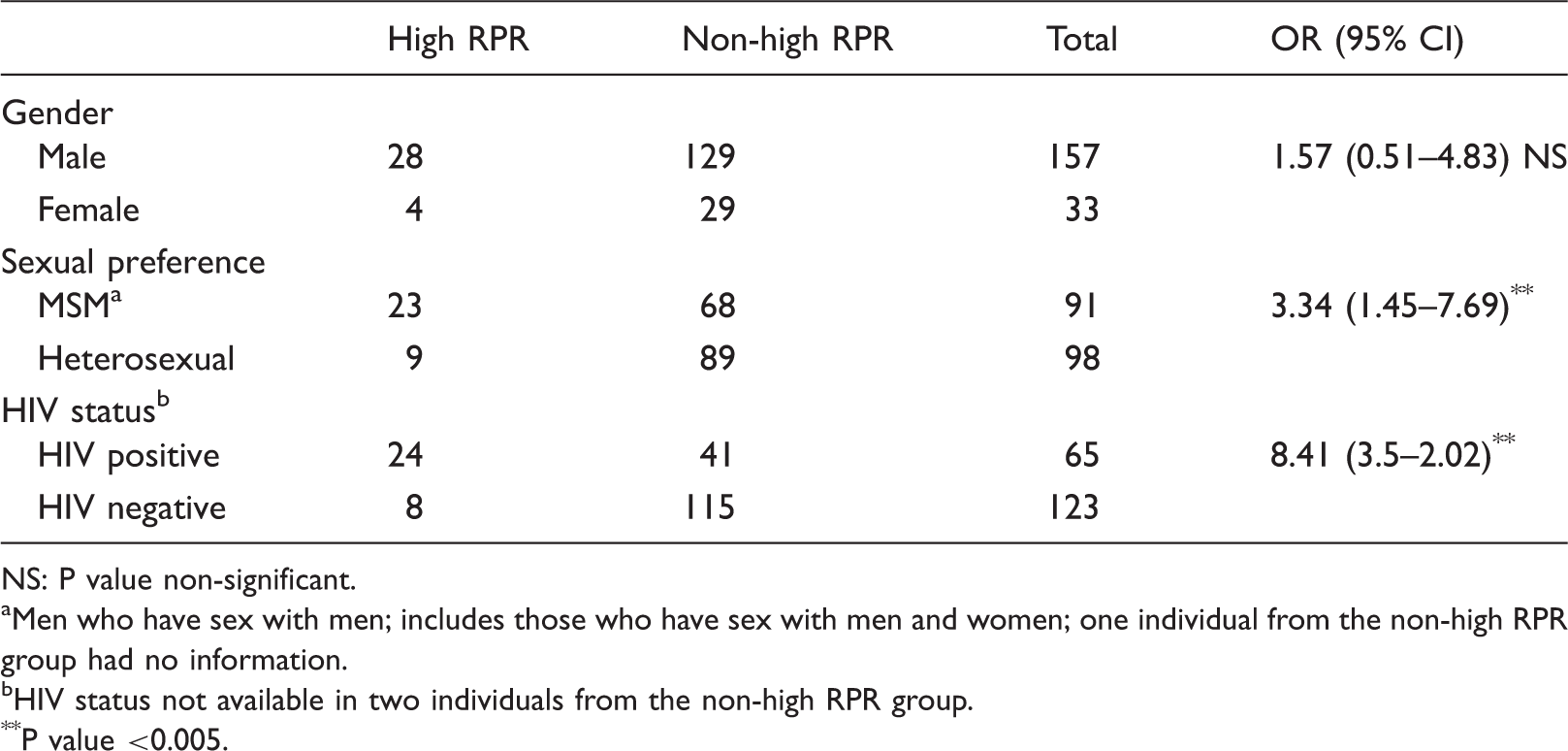
NS: P value non-significant.
Men who have sex with men; includes those who have sex with men and women; one individual from the non-high RPR group had no information.
HIV status not available in two individuals from the non-high RPR group.
P value <0.005.
Fifty per cent of patients with very high RPR titres were symptomatic; the most common symptom was skin rash (93%). Most of them were classified as cases of secondary (16/32), or early latent (13/32) syphilis.
Discussion
We found that in the current epidemic of syphilis in Miami, RPR titres ≥1:512 are more commonly seen in HIV-positive MSM of ethnic minorities.
Our epidemiologic findings are not unexpected as it has been well documented that syphilis in the United States is more prevalent in ethnic minorities, particularly in the South. 3 The current syphilis epidemic in the US has been fueled by cases diagnosed in MSM; many of whom are HIV-positive. 4 Several potential differences in serological testing for syphilis between HIV-negative and HIV-positive patients have been reported mostly through case reports. These differences include an increased rate of negative serological tests in both primary and secondary syphilis, 5 increased false-negative non-treponemal antibody tests due to the pro-zone effect,6,7 high rate of failure to clear non-treponemal antibody after therapy, 8 and sero-reversion to negative specific treponemal antibody tests after therapy in individuals with HIV infection. 9 However, we are not aware of reports specifically addressing high RPR titres in HIV-negative compared to HIV-positive individuals. The reasons for why very high titres are more commonly seen in HIV-positive individuals are unknown. It has been speculated since HIV-positive individuals have more access to health care providers in our city, syphilis could be easily detected during the peak of the RPR titres. However, this report would not support that hypothesis, as most of the individuals with HIV infection were not under care.
There has been only one study analysing the distribution of RPR levels in syphilis infection which included HIV-negative individuals and there was no specific description of the clinical or epidemiological characteristics of the individuals with very high RPR. 10 We believe that given the characteristics of syphilis with phases of complete absence of symptoms, lack of a specific or sensitive test and the absence of a test that can help in the staging of the disease, any additional information regarding RPR values can guide clinicians in the management of the disease.
The main limitations of this report is that it is retrospective, it was conducted in the midst of a syphilis outbreak where MSM are overrepresented, and information regarding HIV care was self-reported. Therefore, these findings may not be extrapolated to the general population.
However, this study has important strengths: all tests were done in the same laboratory and all cases had a confirmatory test and patients were evaluated by the same group of experienced STD clinicians.
In conclusion, we found that very high RPR titres are found in individuals with infectious syphilis who are more likely to be MSM and have concurrent HIV infection.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.