
Abstract
Varicella zoster virus (VZV)-mediated vasculitis is a rare cause of stroke, but should be considered in HIV patients where vasculitis can occur in association with central nervous system – immune reconstitution inflammatory syndrome (CNS-IRIS). A literature search revealed 7 reports of VZV vasculitis over the years with no unifying management strategy, highlighting the difficulty in managing rare conditions in the absence of clear guidelines. This is the first documented case of VZV-mediated vasculitis presenting as stroke in the United Kingdom. Our patient made a full recovery with multidisciplinary input from HIV, neurology and radiology specialists.
Keywords
Introduction
Varicella zoster virus (VZV)-mediated vasculitis is a rare cause of stroke, but should be considered in HIV patients where vasculitis can occur in association with central nervous system–immune reconstitution inflammatory syndrome (CNS–IRIS).
Case report
A 36-year-old Zimbabwean woman was diagnosed HIV positive following development of pulmonary tuberculosis in 2008. She disengaged from care following tuberculosis treatment and re-presented to the tertiary GUM centre with oral candidiasis in April 2012. Her CD4 count was 26 cells/mm3 and HIV RNA viral load (VL) 350,000 copies/ml. She commenced cotrimoxazole as pneumocystis prophylaxis and antiretroviral therapy (ART) with tenofovir/emtricitabine and nevirapine. One month into treatment, she reported severe recurrent headaches accompanied by low-grade pyrexia. Neurological examination was unremarkable and a computed tomography (CT) head scan revealed inflammation of the sinuses. Lumbar puncture (LP) revealed 37 white blood cells with 84% lymphocytes. CSF was PCR positive for VZV with HIV VL of 1300 copies/ml (plasma HIV VL 2300 copies/ml). She was prescribed oral valaciclovir.
Three weeks later she re-presented with severe left peri-orbital headache and facial drooping. Neurological examination revealed right hemianopia and upper motor neurone facial weakness, dysarthria, global dysphasia and dyspraxia. CT brain revealed subacute ischaemia within superficial left temporal and parietal lobes. VZV vasculopathy was suspected and repeat LP revealed 12 white cells (100% lymphocytes) and persistently positive CSF VZV PCR. Repeat CD4 count was 179 cells/mm3.
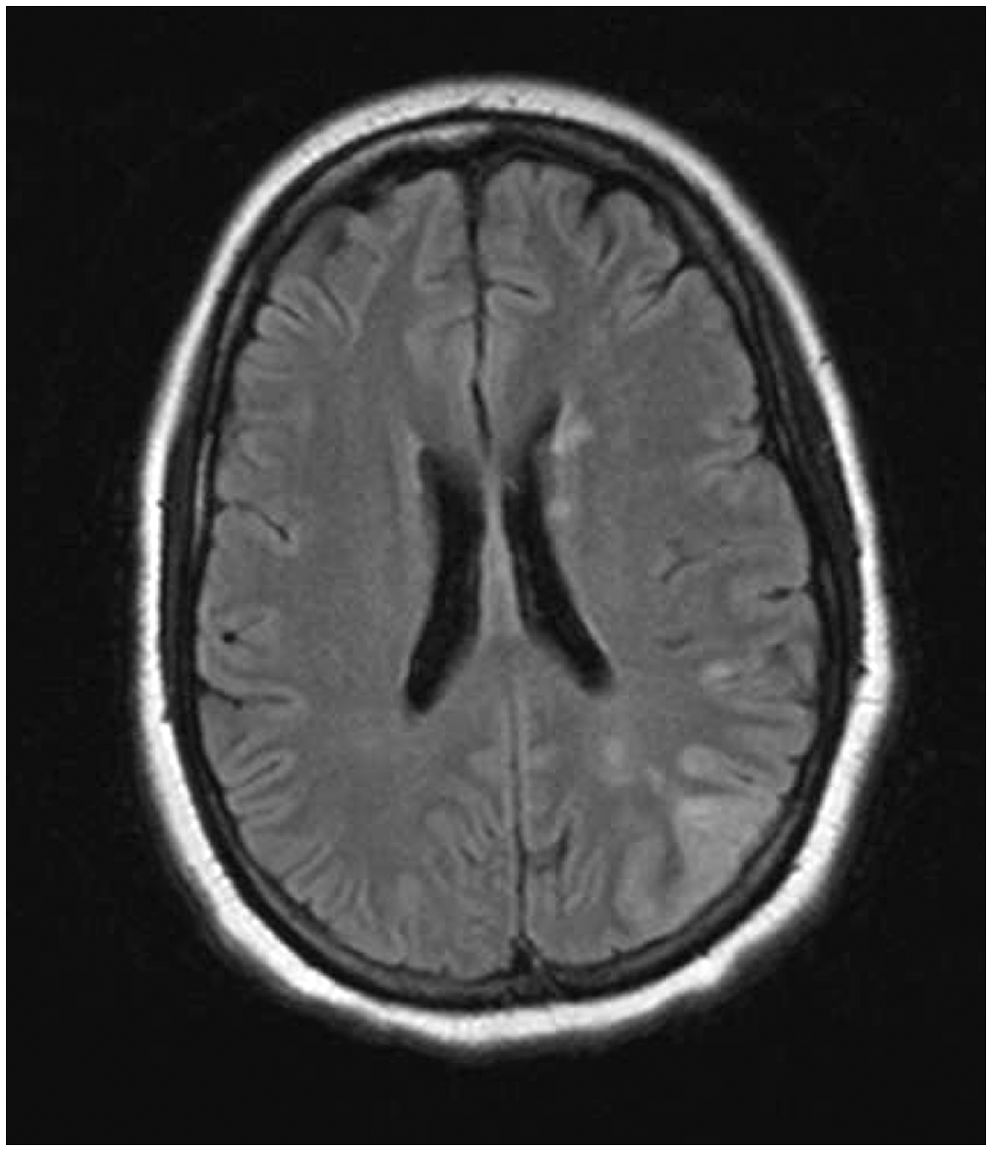
She was commenced on intravenous (IV) aciclovir and aspirin 75 mg. Steroids were withheld at this stage due to worries about infectious vasculitis in the setting of immunocompromise. Magnetic resonance imaging (MRI) brain scan revealed ‘tram lining’ enhancement around the left M1 segment; there were also marked irregularities with multiple focal areas of stenosis within the proximal left middle cerebral artery (MCA) consistent with the clinical suspicion of vasculitis (Figure 1). Flair sequence demonstrated multi-focal areas of left hemispheric infarction within the MCA territory (Figure 2).
Volume rendered magnetic resonance angiography (MRA) of the circle of Willis confirming multifocal beading and stenosis, more marked on the left (see arrows). Flair MRI scan showing corresponding diffusion restriction – consistent with acute left MCA territory parenchymal infarction.
Verapamil 400 mg TDS was commenced as an antivasospastic agent. IV aciclovir was continued for three weeks and followed by a switch to oral valaciclovir.
Unfortunately, she developed new onset right facial droop and slurred speech, with repeat MRI demonstrating progression in the left MCA stenosis with extension of infarcted areas. Repeat CSF showed persistent lymphocytosis but was negative for VZV PCR. This was felt to be VZV IRIS and IV aciclovir was restarted with tapering steroids, over several months.
Although she had some cognitive problems at the time of discharge, follow up at 6 months revealed no residual neurological deficit. A repeat magnetic resonance angiography (MRA) at 1 year was normal.
Discussion
A literature review of VZV vasculitis in HIV-positive individuals yielded seven articles published in the past 16 years; four case reports,1–4 one case series 5 and two systematic reviews,6,7 with a total of 17 patients with HIV VZV vasculopathy.
The prevalence of VZV infection in HIV-positive individuals is unknown, with VZV infection detected in the CNS of 1.5 to 4.4% of post-mortem studies. 8 It most commonly occurs in late HIV infection and can be complicated by the development of IRIS. VZV vasculopathy can affect both large and small arteries resulting in ischaemic or haemorrhagic strokes. Diagnosis is based on a combination of clinical, laboratory and imaging studies.
Clinical presentation can vary, ranging from the development of ophthalmic-distribution herpes zoster followed by acute contralateral hemiplegia weeks and months later, to symptoms of headache, fluctuating mental state, ataxia, aphasia and visual changes. Classic rash was not reported in 37% of VZV vasculopathy.
CSF findings include: a modest pleocytosis (<100 cells, predominantly mononuclear), the presence of red blood cells, elevated CSF protein and normal glucose. Oligoclonal bands are frequently present and specific for VZV immunoglobulin. This can be measured as VZV IgG and is a more sensitive test than VZV PCR but not routinely available in our institution. 9
MRI studies typically demonstrate superficial and deep seated lesions in both grey and white matter, particularly at the grey–white matter junctions. Lesions may be bland or haemorrhagic and may enhance on contrast. MRA demonstrates segmental constriction, often with post-stenotic dilatation. In addition, aneurysms and haemorrhage can also develop. A negative MRA does not exclude the diagnosis of VZV vasculitis, especially if the disease is predominantly in the small vessels. However, in one study, 5 97% of patients had positive findings on CT or MRI, making the diagnosis of VZV vasculitis very unlikely if imaging is normal.
There are no randomised controlled trials to guide the duration of antiviral treatment or use of corticosteroids. Guidelines recommend treatment with IV aciclovir (10 mg/kg) TDS with no comment on duration of therapy. 10 Our patient was treated with three weeks of high-dose IV aciclovir yet relapsed clinically requiring further intravenous antivirals and prolonged steroids, highlighting the difficulty in managing this condition. Despite our initial reservation about use of steroid therapy in this setting, this should be considered in HIV VZV vasculopathy particularly if there is likely to be a significant inflammatory component as in the setting of immune reconstitution. Fortunately, with MDT input, our patient made a full recovery after two months.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.