
Abstract
Summary
Comprehensive testing for asymptomatic sexually transmitted infections in Northern Ireland has traditionally been provided by genitourinary medicine clinics. As patient demand for services has increased while budgets have remained limited, there has been increasing difficulty in accommodating this demand. In May 2013, the newly commissioned specialist Sexual Health service in the South Eastern Trust sought to pilot a new model of care working alongside a GP partnership of 12 practices. A training programme to enable GPs and practice nurses to deliver Level 1 sexual health care to heterosexual patients aged >16 years, in accordance with the standards of BASHH, was developed. A comprehensive care pathway and dedicated community health advisor supported this new model with close liaison between primary and secondary care. Testing for Chlamydia, gonorrhoea, HIV and syphilis was offered. The aims of the pilot were achieved, namely to provide accessible, cost-effective sexual health care within a framework of robust clinical governance. Furthermore, it uncovered a high positivity rate for Chlamydia, especially in young men attending their general practice, and demonstrated a high level of patient satisfaction. Moreover the capacity of secondary care to deliver Levels 2 and 3 services was increased.
Keywords
Introduction
Increasing rates of sexually transmitted infections (STIs) and public demand for STI testing have created access issues for hospital-based genitourinary medicine (GUM) services throughout the United Kingdom. In addition, as the burden of disease falls disproportionally on younger patients from socio-economically deprived backgrounds, frequently the group who need services most are unable to access them because of geographical distance. As a result, different models of care, both in primary care and community-based settings, have been increasingly used as a way of dealing with demand.1,2
This paper outlines the findings from an evaluation of the first six months of a primary care-based Level 1 sexual health service pilot in Northern Ireland. The pilot was situated in 12 practices of one of the five local commissioning areas served by one health and social care trust. Prior to 2010, this area had no specialist sexual health service. In October 2010, a newly commissioned secondary care service, catering for a population of 346,911, was funded for a 0.5 whole time equivalent (WTE) consultant and a 0.8 WTE Band 7 nurse. Recognising that this fell dramatically short of the Royal College of Physicians 3 recommendation of three WTE consultants per 250,000, the service sought to address the capacity issues within the secondary care service by developing a new model of care. In May 2012, the primary care-based Level 1 sexual health service commenced as a pilot in 12 GP practices that serve a population of 60,000 (17.3% of the specialist secondary care catchment population).
Methods
Description of pilot
Training requirements.
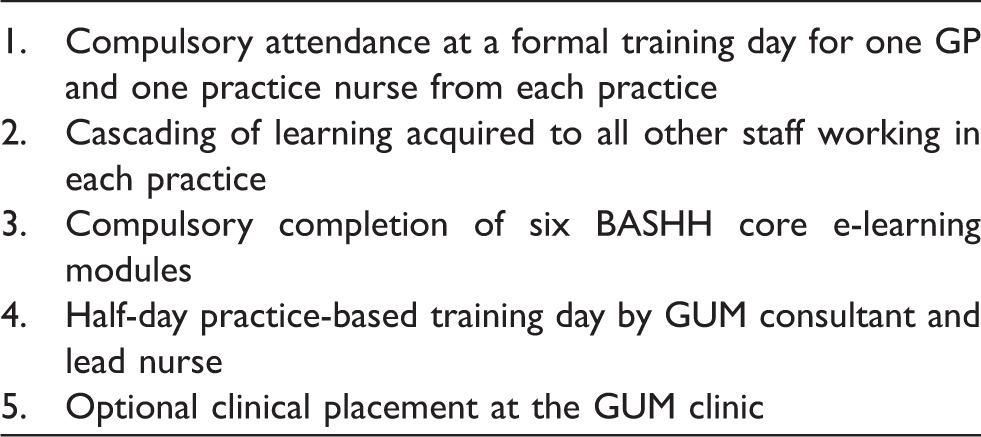
Practices advertised the service by word of mouth, posters and leaflets. Patients booked an appointment with the GP or practice nurse using the practice’s normal booking system. Patients fulfilling the criteria for the pilot who accessed the secondary care service were encouraged to be seen by their GP if applicable.
A sexual health assessment and asymptomatic testing for chlamydia (CT), gonorrhoea (GC), syphilis and HIV were carried out if the patient fulfilled the criteria. GPs instigated treatment and partner notification for positive CT results. A system was put in place to enable GPs to refer patients, found to be positive for GC, syphilis or HIV, directly to the secondary care service.
A Band 5 staff nurse, supported by the lead nurse for sexual health, fulfilled the role of community health advisor (CHA). This role provided a failsafe process for the appropriate management of all positive results received by the GP practices. The laboratory simultaneously informed the GP and CHA of all positive test results from the practices. The CHA then made contact with the practice to ensure appropriate treatment, advice and partner notification had been instituted. The CHA also provided direct support to patients requesting anonymous partner notification.
Data sources
Several data sources including activity recorded by the regional virology laboratory, the LES monitoring forms and the secondary care service informed the evaluation. While laboratory data included information on all testing within the GP practices, the LES monitoring forms only collected information on testing undertaken within the scope of the LES (asymptomatic check up). In addition, a database recording the outcomes of the management of positive CT cases was completed by all practices and a record of all positive tests and details of contact between primary care and the specialist sexual health service was also recorded by the CHA. This was to facilitate an audit of the management of positive cases of Chlamydia, undertaken by the first author. Patient satisfaction surveys were distributed and returned anonymously to the LES monitoring department. An analysis of the cost of providing the service in primary care included the LES tariff and Consultant and CHA costs to support the pilot. The predicted costs for secondary care were calculated by dividing the recurrent funding received by the service by the average number of patients seen per annum.
Results
Patient activity
From the LES data, 293 patients, 69% women and 31% men, were seen by the pilot during the six-month pilot study period. Patient activity increased by 15% as the pilot became established – 157 patients were seen during the second 3 months of the pilot (Aug–Oct) compared to 136 patients seen in the first 3 months (May–July).
Just under half of all patients were aged 16–25 years (142/293; 48%), with men accounting for a quarter of the 16- to 25-year-olds (39/142, 27%).
Testing activity
In the four months of 2012 before the pilot commenced, a mean of 79 CT and GC tests per month were performed by the 12 practices (range 55–97). When the pilot commenced in May 2012, the trend increased monthly to 131 CT and GC tests in the final month of the pilot study period (October 2012), with a monthly mean of 113 (range 101–131).
There was no significant difference between the total number of patients tested in the 4 months before the pilot that were over 25 years of age (203/318, 63.8%) and during the six-month pilot period (422/691, 61.7%) (p = 0.44). The number and proportion of patients under 25 years of age increased from 30/97 (31%) in January2012 to 52/131 (40%) in October 2012, although this increase was not statistically significant (p = 0.2).
The number and proportion of patients that had an HIV test increased from 5/104 (4.8%) test in January 2012 to 61/144 (42.4%) tests in October 2012, which was statistically significant (p < 0.001).
No patients had all four tests (GC/CT/HIV/Syp) performed prior to the pilot. After the pilot started, the proportion of individuals who had all four tests performed increased from 21/121 (17%) in May (pilot commencement) to 48/144 (33%) in October (pilot end), which was statistically significant (p < 0.001) (Figure 1).
Monthly number of tests performed for gonorrhoea (GC), chlamydia (CT), HIV and syphilis, 2012. Source: Regional Virology Laboratory.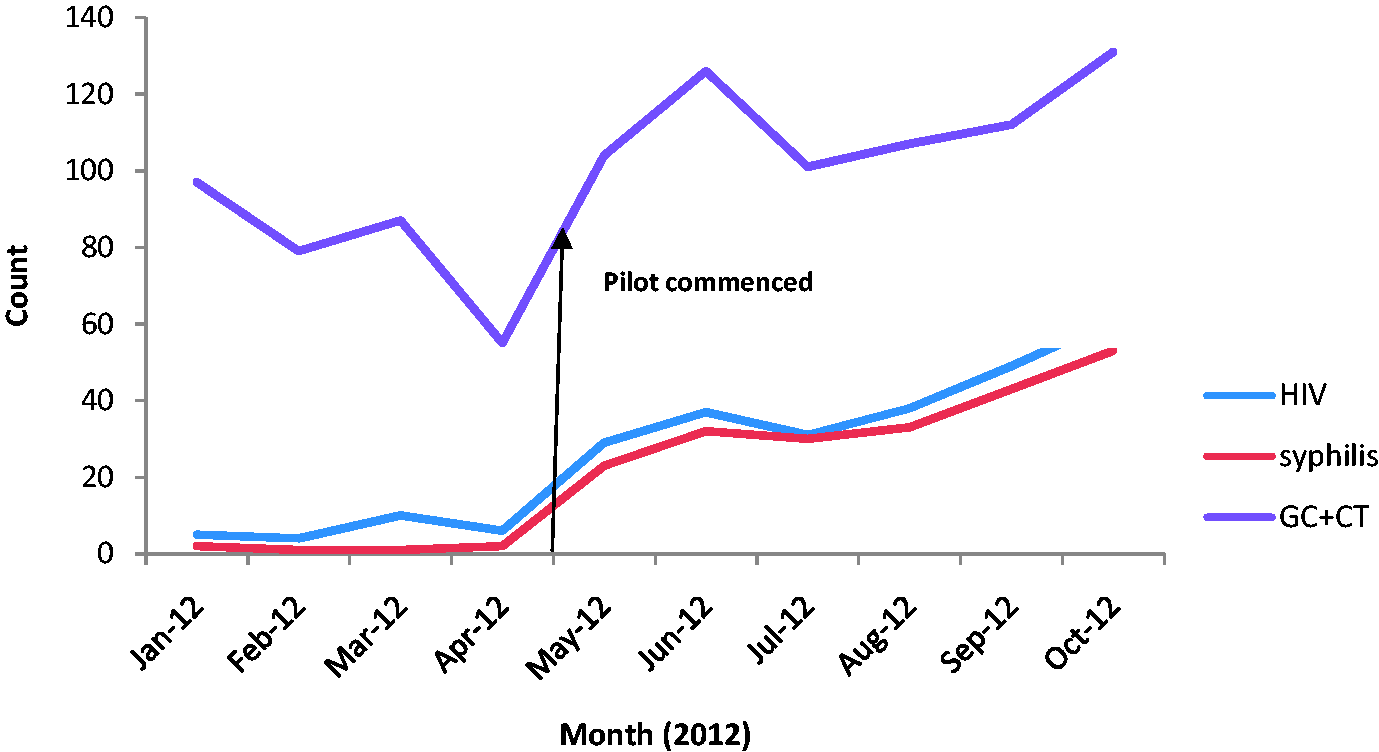
Positivity rates
Number of positive tests from pilot according to gender.
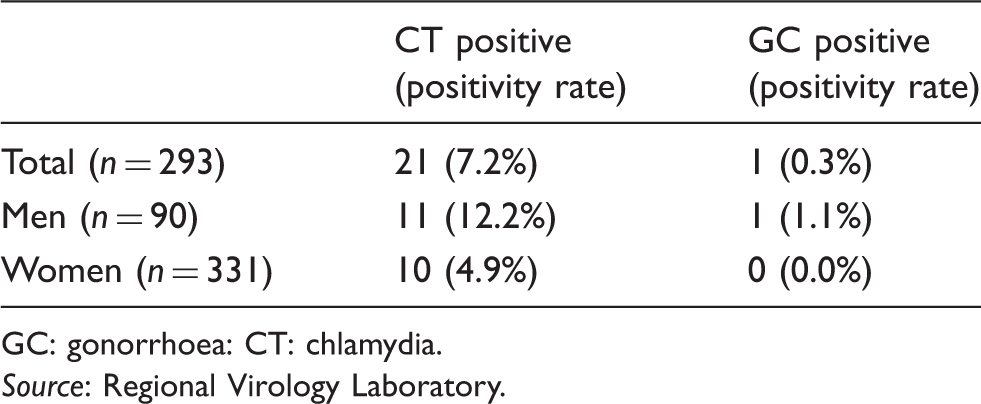
GC: gonorrhoea: CT: chlamydia.
Source: Regional Virology Laboratory.
Comparing the pilot and secondary care service
Positivity rate (PR) of CT in 16- to 25-year-olds attending secondary care service compared with pilot for period May–October 2012.
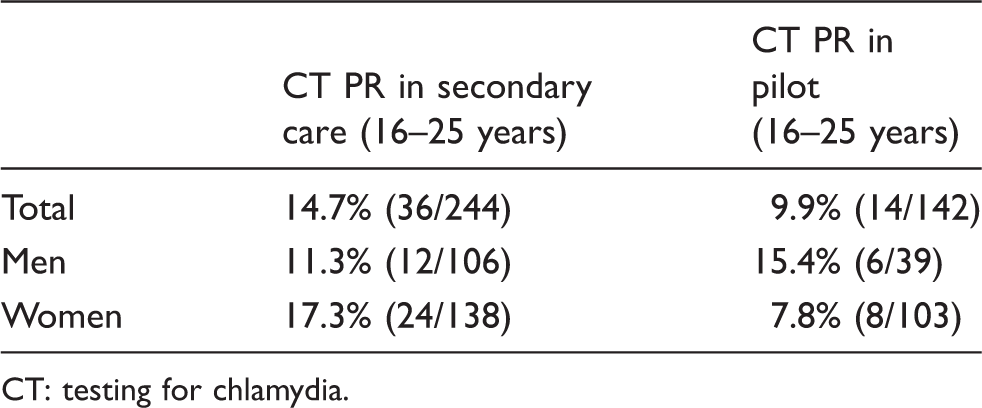
CT: testing for chlamydia.
Patient activity data obtained from the secondary care service in 2011 showed that overall more men were accessing the secondary care service (653/1611; 40%) than the primary care pilot service (91/293; 31%), which was shown to be statistically significant (p < 0.001).
However, the reverse was true for men aged 16–25 years, with only 25.7% (168/485) accessing the secondary care service compared to 42.9% (39/91) accessing the primary care pilot (p < 0.001).
Performance indicators
An audit of the management of CT since the introduction of a CHA providing support was carried out by the first author in collaboration with the practices. The audit sample was all positive CT patients from the 12 practices, whether part of the pilot or not (n = 43). Management of CT patients, including timeliness of results and partner notification, was audited against BASHH standards.
HIV testing
One hundred percent of patients seen in the pilot should be offered an HIV test and 60% should have an HIV test performed (Key Performance Indicator (KPI) for BASHH standard 3)
The LES monitoring returns did not collect information on each test that patients were offered and availed of. Information was available for HIV testing in patients who had a positive CT or GC result with 60% of these patients having had an HIV test performed.
Timeliness of laboratory reporting
One hundred percent of laboratory reports should be received by clinicians within 7 working days of a specimen being taken (KPI for BASHH standard 4)
One hundred percent of patients should receive the laboratory results within 14 working days (KPI for BASHH standard 5)
Information on the time period was only available for less than 8 days rather than the KPI standard of 7 working days. A laboratory result was available to the clinician within 8 days of the specimen being taken for 70% of patients (n = 43). In addition, 91% of patients were informed of their result within 14 days of the specimen being taken.
Partner notification
The rate of partner notification for CT and GC for each provider should be at least 0.4 – 0.6 contacts per index case within 4 weeks (KPI for BASHH standard 5).
Partner notification was not measured using the KPI measure of contacts per index case. However, partner notification was documented as undertaken in 93% of patients positive for CT (n = 43), although two cases were reported as not requiring it. Primary care initiated partner notification in all cases, either using the contact slips provided in the resource pack or directly by the patient. Four patients were also referred to the secondary care service to provide further partner notification, either by telephone or face-to-face consultation.
Partner notification was documented as undertaken in 100% (3/3) of patients positive for GC. Two were seen in the secondary care service for follow-up and partner notification. The third patient had moved away from Northern Ireland so had telephone follow up by the secondary care service.
Reduction in proportion of asymptomatic patients using secondary care
The secondary care sexual health service provides a nurse-led clinic in a local Community Hospital, which is the nearest specialist service that patients from the pilot practices would use prior to the pilot commencing. The proportion of patients attending the secondary care sexual health service at the Community Hospital for asymptomatic STI testing fell from 25% (10/39) in October 2011 to 11% (4/36) in October 2012, although this was not a statistically significant difference (p = 0.14).
Patient satisfaction survey
Forty-two patients in the first three months of the survey (n = 136) completed the patient satisfaction survey from eight of the twelve practices (response rate = 31%).
Ninety percent (38/42) of responders heard of the service from their own surgery. The remaining heard about the service from the local press (5%; 2/42), the secondary care sexual health service (2%; 1/42) or from another source (2%; 1/42). Overall, 98% were either very satisfied (91%) or satisfied (7%) with positive comments highlighting the accessibility of the service.
‘Scheme is an excellent idea as the location of my nearest clinic was over 30 minutes away & waiting times without appointment meant it just wasn't feasible. Having a local clinic makes testing much easier & much more available to everyone.’
Cost of provision of service in primary care
Comparison of costs for providing locally enhanced service (LES) primary care versus predicted cost for same case mix seen in secondary care service.
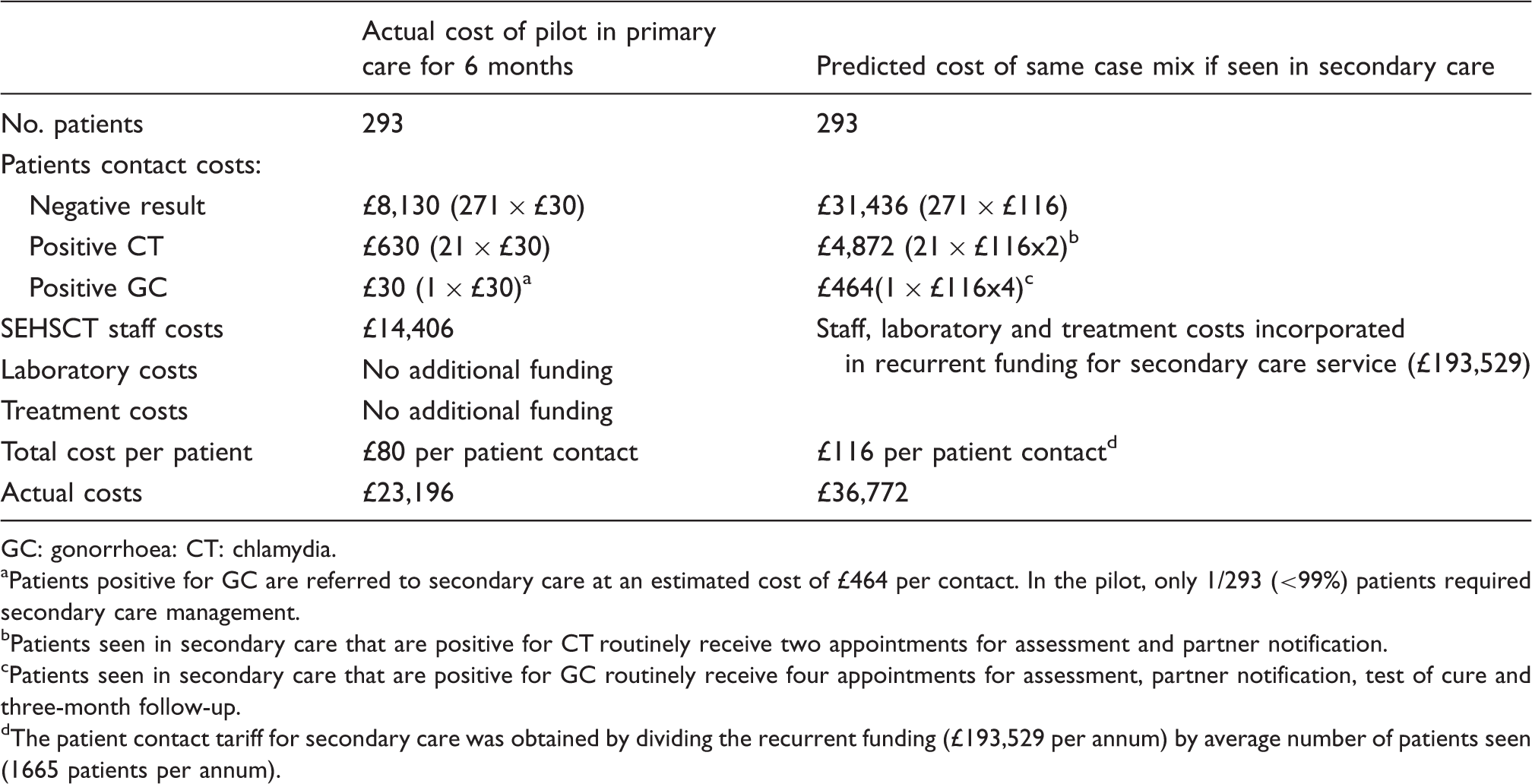
GC: gonorrhoea: CT: chlamydia.
Patients positive for GC are referred to secondary care at an estimated cost of £464 per contact. In the pilot, only 1/293 (<99%) patients required secondary care management.
Patients seen in secondary care that are positive for CT routinely receive two appointments for assessment and partner notification.
Patients seen in secondary care that are positive for GC routinely receive four appointments for assessment, partner notification, test of cure and three-month follow-up.
The patient contact tariff for secondary care was obtained by dividing the recurrent funding (£193,529 per annum) by average number of patients seen (1665 patients per annum).
The overall actual cost for providing the service in primary care for 293 patients was £80 per patient: £23,196. The patient contact cost in secondary care (£116) was calculated by dividing the actual number of patients seen in secondary care in one year (1665) by the recurrent funding (£193,529). In addition, patients with positive results require follow-up appointments for treatment, for partner notification and ongoing care as necessary. The overall predicted cost for providing the service in secondary care for 293 patients was: £36,772.
Discussion
Previous evaluations of LES in sexual health in England have shown that standards relating to accessibility, staff training and competencies were well met, with the exception of partner notification. 4 However, concerns about the effectiveness of partner notification outside the traditional GUM setting were previously proved to be unfounded in another audit of a community service. 5 To date in Northern Ireland, there is no regional chlamydia screening programme and comprehensive STI testing has been exclusively provided by GUM clinics, with little or no communication with colleagues in primary care. This pilot aimed to introduce a new model of care, and as such represents an important step in changing the culture of care provision. This evaluation adds to the evidence that primary care-based services can provide accessible Level 1 asymptomatic testing, treatment and partner notification, when robust clinical governance and training arrangements are in place and supported by a specialist secondary care service.
The sexual health pilot took place in GP practices situated in an area of high population density, where some of the most deprived super output areas (SOAs) and a cluster of children’s homes are situated. For this population, in particular, an accessible service refers not only to availability but also one within easy reach. In the patient satisfaction survey patients praised the service for its close proximity to home, stating that it made STI testing much easier and more available to everyone. As with previous studies our findings showed that patients are happy to seek sexual health services from their GPs6,7 attracting increasing numbers of men and young people. 8 In particular, young men used the service almost twice as much (43% versus 25%) as the equivalent secondary care service.
The positivity rate for CT in young men in the pilot was shown to be higher than the rate in secondary care for the same age group of men, clearly identifying an unmet need in the local area. However, overall the CT positivity rate in both the pilot and the secondary care service was not dissimilar, refuting an often purported concern that incentivising GPs leads to inappropriate opportunistic testing practices.
The findings also suggest that the availability of asymptomatic testing within primary care may help to increase the capacity of the secondary care service to see symptomatic patients, with the findings confirming that patients attending the nurse-led specialist sexual health clinic for asymptomatic testing fell from 25% (10/39) of all attendances in October 2011 to 11% (4/36) in October 2012.
The cost of providing the service in primary care was approximately 1.5 times less expensive than if the same case mix of patients had been seen in the pre-existing secondary care service. It should also be noted that the costs for the consultant support will become proportionally less as the pilot is rolled out more widely because training, competency and clinical governance arrangements will have been established. However, as laboratory costs were not included in the total cost of the pilot, these being absorbed within the laboratory’s recurrent funding budget, any expansion of primary care-based services would incur additional laboratory costs.
Previous studies have shown that LES sexual health services in the UK lacked support from specialist services, resulting in poor specialist input, shared protocols, clear referral pathways and lack of data collection. 4 In contrast, the success of this primary care-based service has been achieved as a result of the strength of the partnership between the secondary care service and GP practices. A core component of this partnership has been the provision of a CHA to the 12 practices, which ensured appropriate treatment, advice and partner notification was instituted. While GPs were testing for CT in symptomatic patients prior to the introduction of the pilot, the introduction of a CHA to support the management and record keeping of all positive results and as an accessible contact within secondary care was welcomed. National outcome standards were measured for some clinical outcomes showing that 91% of CT- and GC-positive patients received treatment within 14 days, 60% received an HIV test and partner notification was documented as completed in 98% of CT- and GC-positive patients. A limitation of the audit was that the KPI measure of contacts per index case for partner notification was not included in the proforma for data collection. The findings clearly show that robust arrangements are in place for training and providing ongoing support for GPs and practice nurses, clinical governance and performance outcome measures, treatment and partner notification of positive cases. However, we acknowledge that any future development of this model will require ongoing assessment of competence of practitioners to deliver a Level 1 service.
This pilot aimed to introduce a new model of care in Northern Ireland, and as such, represented a cultural shift in how comprehensive STI testing is provided and accessed. While our evaluation shows that this model of care is acceptable to patients, GPs and practice nurses, a number of issues have been highlighted in the process. In the beginning, some pre-existing barriers to offering HIV and syphilis serology testing appeared to exist, but this improved as the pilot became established and has continued to become more ‘routine’ as the project continues past the point of evaluation. In addition, whilst our evaluation found the service to be cost-effective, any future roll out of the model would require full economic assessment, including laboratory costs and continuation of enhanced payments. In addition, any roll out of this service in primary care will require a commitment to ongoing training and competency assessment. However, in an area such as Northern Ireland with varied geographical distance between GUM services, this pilot has shown that successful partnerships between primary and secondary care can achieve well-coordinated, integrated care, good working relationships between primary care physicians and secondary care specialists and a general increased awareness of sexual health amongst primary care physicians.
Footnotes
Acknowledgements
The authors thank Dr Conal McCaughey, Consultant Virologist, for the provision of laboratory data. They also thank Dr Bernadette Cullen, Dr Kathryn Booth, Wesley Graham and Claire Rainey of the Public Health Agency and Martina O’Neill, Robert Moore and Roisin Degan of the South Eastern Health & Social Services Trust for their work in supporting and monitoring the pilot.
The authors also thank the anonymous reviewers for their helpful comments.
Conflict of interest
The authors declare no conflict of interest
Funding
The pilot project was funded by the Health and Social Care division of the Public Health Agency for Northern Ireland.