
Abstract
In 2008, nurse-administered HIV oral rapid testing (RT) was introduced at the Veterans Affairs Primary Care Clinic in Downtown Los Angeles. Analysis at five years revealed variable yet increasing rates of HIV RT at that facility despite the fact that no post-launch support was provided by the implementation team. Qualitative interviews among stakeholders conducted at five years revealed the pre-existing implementation practices endemic to this clinic that facilitated this unprecedented success (e.g. history of positive quality improvement implementations, leadership support, clinician involvement at each step of the process to facilitate empowerment, ownership and feasible customisation of the implementation, cohesive communication among clinicians and leadership, training, efficient supply pathway, progressive performance feedback and ongoing encouragement).
Background
Among the approximately 1.2 million persons living with HIV in the United States, it is estimated that 20% of these individuals are unaware of their status. 1 The consequences associated with these (asymptomatic) unidentified individuals are twofold: first, they do not receive the necessary treatment in a timely fashion, and second, they may be unknowingly transmitting the disease to others. 2 Effective antiretroviral therapy has reformed the outlook of HIV from a non-negotiable death sentence to a manageable chronic disease. 3 Since the development and use of highly active antiretroviral therapy, HIV mortality rates are largely associated with late diagnosis, leading to a delay in treatment. 4 In an effort to increase HIV detection, diagnostic guidelines have recently been revised to recommend a shift away from risk-based testing, to universal testing of all patients at least once per lifetime, starting at age 13. 1 The U.S. Department of Veterans Affairs (VA), the largest single provider of HIV care in the country, has recently adopted this recommendation. 5
Current testing methods have been shown to be highly ineffective, however, due largely to the method itself. Conventional HIV testing requires both a blood draw and laboratory analysis, requiring a patient to return days or even weeks later to receive test results. Consequently, a significant number of people simply do not return for their results. This is vitally important, for research shows that when people are aware of their status, they tend to cease or at the very least, lessen their risk-related behaviours, which in turn works to reduce further spread of the epidemic. 6 Lack of return for test results has been shown to be a significant contributor to the HIV epidemic. In a recent study, almost one-third who tested HIV positive did not return for results. This unawareness on the part of so many infected individuals has staggering implications for the spread of the HIV epidemic, for as Centers for Disease Control and Prevention data suggest, those unaware of their HIV-positive status are 3.5 times more likely to infect others than those who are aware of their HIV status. An additional barrier is needle phobia; the formal diagnosis is ‘Specific Phobia, Blood-injection-injury type’, which has a 10% prevalence among children and adults. The symptoms of this phobia go beyond ordinary needlestick anxiety 7 ; as such, these patients tend to resist seeking medical care, placing them at greater risk for a variety of undiagnosed diseases. 8
To address these barriers, same-day HIV oral fluid rapid testing (RT) and nurse-initiated screening have been proposed as remedies to increase screening in general medical and urgent care settings. 2 HIV RT using oral fluid alleviates the need for patients to return for results and the need for a needlestick. Nurse-initiated screening (sometimes called ‘standing orders’) systematises testing into primary prevention priorities. HIV RT has been widely applied in non-primary care settings and is acceptable to both patients and providers.9,10
In addition to being optimal for needle-phobic patients, this instrument is advantageous in that results can be provided on the same visit, as opposed to making this a two-step clinical process (blood draw, then notify patient of results). Additionally, patients are more amenable to such testing in that they need no longer endure weeks of anxiety waiting for test results. 11 In a previous randomised, controlled trial within VA, nurse-initiated HIV rapid testing (NRT) was more acceptable to patients than current venipuncture methods and also significantly increased receipt of test results. 12
Prior to this implementation, the FDA-approved OraQuick® Advance Rapid HIV-1/2 Antibody Test (OraSure Technologies Inc., Bethlehem, PA, USA) was reviewed and approved for use by the Greater Los Angeles laboratory services director, chief of infectious diseases, and medical executive committee. Admittedly, there have been concerns regarding the accuracy of oral testing for HIV; recent evidence suggests that much of the testing error can be attributed to misuse of the device, specifically in the realm of at-home testing. 13 When used properly, the oral HIV test performs essentially equivalently to the blood (ELISA) test.14,15 Each of the tests conducted in this implementation was administered by qualified healthcare professionals who underwent extensive training in the proper protocol for storing, administering and reading this device.
In 2008, practitioners (i.e. nurses and physicians) at two Veterans Health Administration Medical Center primary care clinics in Southern California were trained to administer HIV RT. Practitioners who were interested in becoming certified to administer the HIV RT were required to attend two 90-min in-services. Part I was offered by a clinical social worker and entailed HIV education, therapeutic communication skills, techniques for effectively proposing HIV testing, pre-test counselling, completing the informed consent documentation (which was mandatory at the time), a demonstration of the test instrument detailing test storage, test administration and interpretation, entering the test outcome into the VA electronic medical record and post-test counselling. 16 Part II was administered by the laboratory manager. This hands-on tutorial trained practitioners how to conduct the manufacturer’s specified quality control procedures. Part II training concluded with practitioners demonstrating competency in properly interpreting simulated test outcomes for negative and (preliminary) positive results. Initially, we trained 10 registered nurses (RNs) to administer the HIV RT, eight of whom participated in the launch. In instances wherein the HIV RT rendered reactive results, this was regarded as a preliminary positive HIV test; per existing policy, all initial (ELISA) reactive results automatically triggered an order for a confirmatory Western blot (blood) test.
On 1 April 2008, a six-hour launch event was held during which a team of the trained nurses administered 83 HIV RTs. Following the launch event, the nursing staff offered the HIV RT to primary care patients on a regular basis, regardless of risk factor(s). The research team member who had trained the practitioners did not maintain regular contact with the clinic.
Objective
The objective of this manuscript is to evaluate the long-term sustainability of NRT in a VA primary care clinic in Los Angeles 12 following training and an initial kick-off event. Quantitative testing rate data for the five years following the kick-off event are presented, followed by qualitative data from staff interviews to contextualise the quantitative results.
Methods
Staff interviews
Semi-structured interviews lasting approximately 60 min each were conducted with nine clinic staff. The sample included the medical director, the nurse manager, four RNs and three licensed vocational nurses (LVNs). Two of the RNs and two of the LVNs were selected because they had been involved with HIV RT from the launch date or shortly thereafter. Additional RNs and LVNs were randomly selected from the remaining clinic staff. The Greater Los Angeles VA Institutional Review Board deemed these confidential staff interviews exempt from review as the interviews were considered to be part of a quality improvement initiative to increase HIV testing rates within the Veterans Health Administration.
The British National Health Service Sustainability Index (SI) Model17,18 was used as a guide to construct the semi-structured interview questions. The SI is a quantitative rating scale covering 10 factors found to predict sustainability of new practices. For each factor, the respondent chooses a ‘level’ corresponding to how well their change effort exemplifies that factor. We chose to construct a qualitative interview for this study rather than using the quantitative scale as we were interested in more detailed descriptions of how the factors were operationalised for HIV RT in the hopes of developing actionable recommendations for other clinics. The interview was structured to cover nine of the 10 factors of the SI. The factor ‘Benefits Beyond Helping Patients’ was not covered as implementing HIV RT was not expected to ‘improve efficiency’ or ‘make jobs easier’ for the primary care clinic staff, although presumably it may have had these effects for laboratory staff by decreasing the number of standard HIV (blood) tests run in the laboratory. The resulting interview was pilot tested for question clarity and to ensure that the targeted interview length of 60 min was not exceeded. Following the first participant interviews, the two factors ‘Senior Leadership Engagement’ and ‘Clinical Leadership Engagement’ were combined as interviewees were identifying the same individuals when discussing both of these factors.
Detailed notes were recorded during each interview. Content analysis was used to code participants’ responses into categories reflecting the SI factors and to identify illustrative quotes. For each SI factor, coded content was compared to the factor levels to determine how well the HIV RT implementation exemplified that factor.
Results
Quantitative HIV testing results
HIV RT data were gathered via deidentified queries of the computerised patient record system, wherein only actual ordered tests were recorded. Over the course of the five years following the launch event (1 April 2008 through 31 March 2013), nurses at this site administered a total of 2117 HIV RTs; this works out to a quarterly mean of 106 (SD = 50.6) HIV RTs. Despite the variability of the testing rate, the positive slope of the dotted trend (regression) line depicts the average quarterly increase of 2.6 additional tests per quarter over this timeframe; using a .05 α level, this is considered to be statistically significant (p = .001) (Figure 1).
Quarterly HIV RT counts: April 2008–March 2013.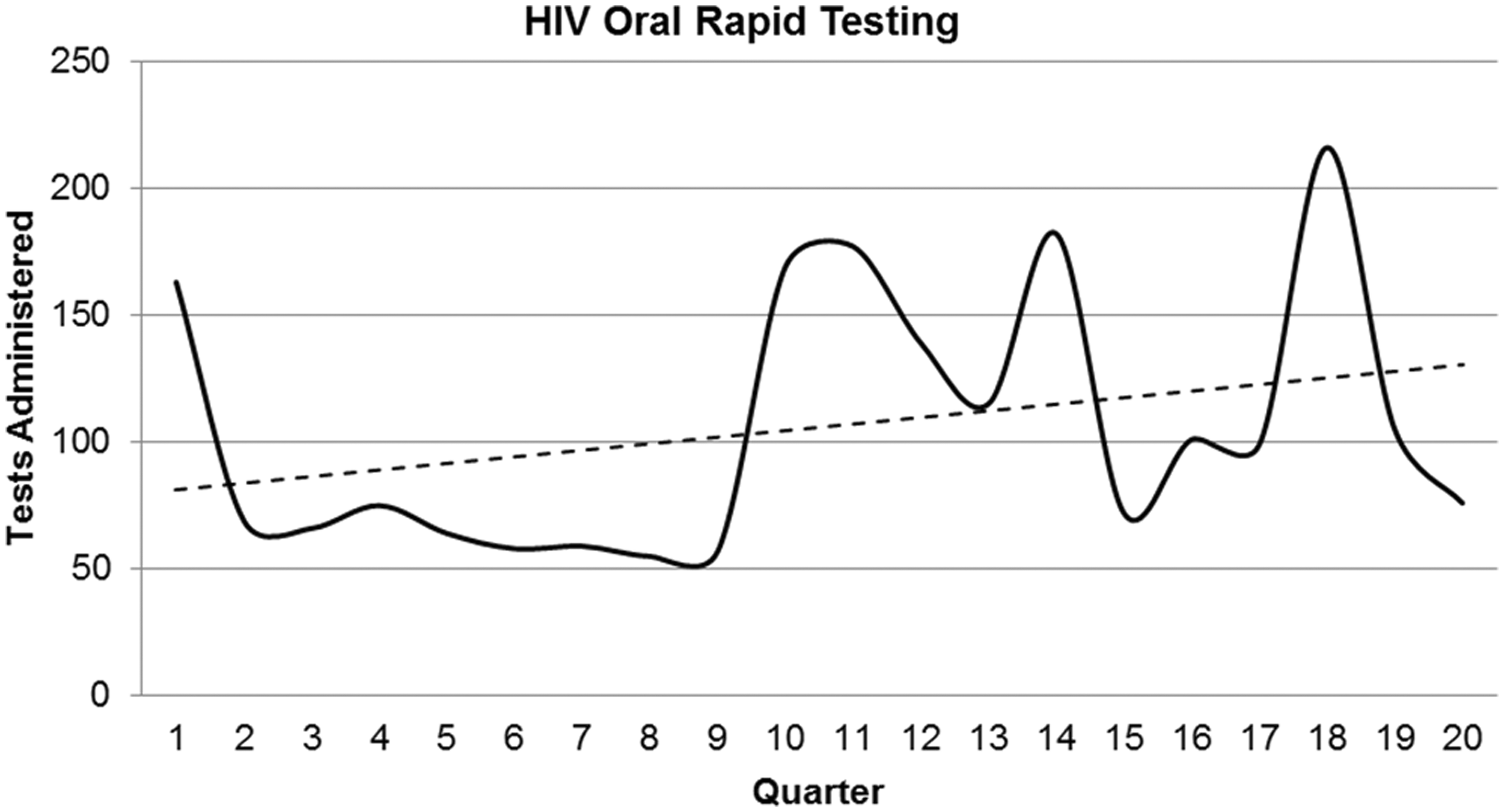
We regard these results as exceptional, considering that the research team member who initiated this implementation was stationed 15 miles from the targeted facility and did not maintain regular contact with that site after the launch event. According to implementation science principles, it was expected that without a persistent supportive presence on site and periodic booster efforts, the success observed early in this process would be short-lived. Contrary to this, we observed a continuous sustainment of this intervention with no outside prompting or support. The remainder of this paper focuses on comprehending the story behind the longitudinal sustainment of this implementation.
Qualitative interview results
Sustainability Index Factors, highest factor level achieved and illustrative quotes.

RNs: registered nurses; LVNs: licensed vocational nurses.
The HIV RT implementation met the criteria for the highest level on every SI factor with two exceptions. ‘Benefits Beyond Helping Patients’ received the lowest rating and was not covered by the interview because HIV RT implementation was not expected to improve efficiency or make jobs easier for the primary care clinic staff. ‘Adaptability of Improved Process’ received a moderate rating. This factor has two components: ‘the process can adapt to other organisational changes’ and ‘there is a system for continually improving the process’. The only major organisational change that was referenced in the staff interviews was staff turnover. A clear protocol was described for training new staff on the HIV RT programme, and the programme was referred to as ‘part of the clinic culture’ that was passed on to new staff as they arrived. However, there was no indication from the interviews that there was a system in place to continually improve the testing programme. The programme that was put in place, was functioning well and had continued in basically the same form from the time of the kick-off.
In considering how this implementation was sustained over five years, several key ingredients appear to have come together in this specific situation. First, it was immediately obvious to the clinic staff that the innovation, rapid oral fluid HIV testing, had benefits over standard HIV blood tests, (e.g. timely results, no needlestick). Second, the geographic location of the clinic in the heart of Los Angeles made the innovation more salient. A high percentage of the Veterans served by the clinic are homeless and engaged in high-risk drug use and sexual behaviours. Therefore, methods to increase HIV testing rates met a need recognised by all of the staff. Third, the innovation was proposed for implementation at a site where there already existed dynamic and well-respected leadership. Probably in large part due to the leadership, the team viewed themselves as high functioning, having good communication and able to achieve success with implementation efforts. The leadership strategy of involving all of the clinic staff in the implementation decision and planning helped the staff to feel empowered and respected and gave them a sense of ownership over the implementation. Finally, sustainability was supported by establishing protocols for annual refresher training for current staff and training for new staff as well as protocols for monitoring progress and sharing monitoring reports with staff.
Despite the overwhelming preponderance of positive information collected during the interviews, we do not want to suggest that there were not some concerns reported. In fact, some of the collected information suggests that the sustainability of the HIV RT programme may be in jeopardy in the future. A minority of the staff interviewed felt that the priority of HIV RT was waning as suggested by the following quote:
‘The culture of the VA is that we have the disease of the month, things that are of special interest and focus. HIV screening had its heyday and now it’s on maintenance so nobody gets too excited about it’.
The staff who reported this decreasing enthusiasm attributed it to leadership changes. They did not feel that HIV RT was as high of a priority for new leadership as indicated by less frequent sharing of the testing data. They also felt that staff time was becoming more of a barrier because of staff shortages and new tasks being continually added to primary care nurse workload.
Conclusion
Our qualitative analysis focusing on the Sustainability Index Factors revealed that HIV RT was in fact well suited to the patients served by this clinic; however, simply identifying that fit is not necessarily sufficient to achieve the successful launch and sustainability observed in this setting. Pre-existing positive practices and operational norms endemic at this clinic provided fertile ground for a prompt uptake and longitudinal sustainability, specifically, their history of sustained quality improvement, suitable staffing, job descriptions, policies, procedures, equipment, positive performance feedback and communication pathways. Other elements attributable to this success involved leadership enthusiastically embracing the new implementation and involved staff at inception. This practice of full staff engagement empowered the nurses to own and customise the HIV RT process to best fit into their clinical repertoire. Additionally, leadership provided nurses periodic performance briefings and ongoing encouragement, which provided a feedback system to enact implementation changes as needed. It is expected that such success(es) could be achieved with HIV RT and other viable implementations at other sites, provided the institutional culture is as positive and efficient as this team. The results also highlight the importance of understanding the context in which implementation will take place. Pre-implementation contextual assessment would allow for determination of critical contextual elements that are already in place and those that are missing and may need to be addressed prior to undertaking an implementation effort.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.