
Abstract
We report a case of chancroid in a white heterosexual man in the United Kingdom. This patient was seen by four separate health services over a period of five weeks with excruciatingly painful penile ulcers. Despite several negative herpes simplex virus polymerase chain reaction tests and a self-diagnosis of chancroid, he was repeatedly offered multiple courses of aciclovir. This case highlights the need for awareness of alternative diagnoses in persistent cases of genital ulcer disease.
Keywords
Introduction
Chancroid, although common at the turn of the 20th century, is now a rare cause of genital ulcer disease (GUD) in the UK. In 2011, the Health Protection Agency recorded 67 cases in England of which only one was in the North East. Chancroid is caused by the Gram-negative coccobacillus Haemophilus ducreyi and is characterised by painful genital ulcers accompanied in 10 to 40% of patients by inguinal lymphadenitis or bubo formation. 1 The diagnosis is best confirmed by polymerase chain reaction (PCR) testing. In recent times, owing probably to a combination of enhanced sexually transmitted infection (STI) surveillance, 2 short infectivity 3 and susceptibility to azithromycin 4 chancroid appears in industrial countries to be limited to isolated outbreaks.5,6
Case report
A 23-year-old white Caucasian man from the North East of England, with no history of recent contact with a commercial sex worker or non-UK resident, presented to our service with a nine-day history of progressively enlarging red ‘spots’ on his penis. On examination, he had three extremely tender erythematous lumps on his glans penis and coronal sulcus. He had no other symptoms, findings or evidence of lymphadenopathy. A provisional diagnosis of Herpes simplex virus (HSV) infection was made pending investigations. Treatment was deferred. In addition to his regular female partner, he had a casual female sexual contact nine days prior to the onset of symptoms. Both contacts were white and from the North East.
He re-attended our service 14 days later. All prior investigations including HSV PCR, syphilis and HIV serology were negative. On examination, the three lumps previously noted were found to have ulcerated. He had no lymphadenopathy. A five-day course of aciclovir for suspected HSV was initiated; however, a repeated HSV PCR taken at that time was negative.
He was reviewed 10 days later. In the intervening period, he had presented to two other genitourinary medicine (GUM) services, a walk-in centre and an A + E department in an increasingly desperate state. He was unable to sleep, study or carry out normal activities such as putting on his socks because of the pain generated by the ulcers. He researched his condition on the internet and made a self-diagnosis of chancroid. On his last two attendances he explained his diagnosis and requested erythromycin but was reassured he had herpes. Such was his desperation, he threatened to kill himself unless he was given some erythromycin. A casualty officer reluctantly issued a three-day course of erythromycin 500 mg four times a day.
Examination revealed three extremely painful, deep, irregular, sloughy-based ulcers with raised edges, oozing yellow serum (Figure 1); one located on his frenulum and two on the coronal sulcus (Figure 2). Other than mild bilateral tender lymphadenopathy, he had no other signs and had just completed the three-day erythromycin course issued in A + E. We suspected lymphogranuloma venereum (LGV) infection and commenced him on doxycycline 100 mg twice a day. Multiplex PCR testing for H. ducreyi via Public Health England’s Colindale Reference Laboratory was reported 10 days later as positive, and he was reviewed in clinic the same day. His ulcers had healed; however, in view of the diagnosis of H. ducreyi, he was treated with a stat dose of azithromycin 1 g.
Contact tracing was initiated. His regular partner was asymptomatic with a negative STI screen. She was treated empirically with azithromycin 1 g; unfortunately, we were unable to trace his casual contact.
Discussion
Chancroid is an uncommon infection in the UK. However, as illustrated by our case, the diagnosis should be considered in any patient presenting with intractable painful genital ulceration (with or without lymphadenopathy) and in whom HSV has been excluded. Currently, the most reliable diagnostic technique is PCR testing 7 (95% sensitivity). Microscopy has low sensitivity and culture is no longer commercially available. (In the past, when a variety of different culture media were used to identify chancroid there was a significant risk of false-positive diagnoses associated with HSV. This is not the case with PCR testing).
Important differential diagnoses to exclude are syphilis, LGV, Behçet's disease and infections due to Streptococcus pyogenes or Staphylococcus aureus. 8
The most convenient treatment option is single-dose oral azithromycin 1 g. Erythromycin is also effective; however, tetracyclines have minimal activity against H. ducreyi and are not recommended.4,9 (Our patient was probably cured by his three-day course of erythromycin).
This is an interesting case not only for the pathology but also because the patient reached the correct diagnosis and treatment before the health professionals. The internet is indeed an astonishing tool for education.
Chancroid ulcers showing typical features; deep with ragged, raised, under-mined edges and a necrotic yellow base. Kissing chancroid ulcers on the sub-prepuce and coronal sulcus. Painful, non-indurated and friable.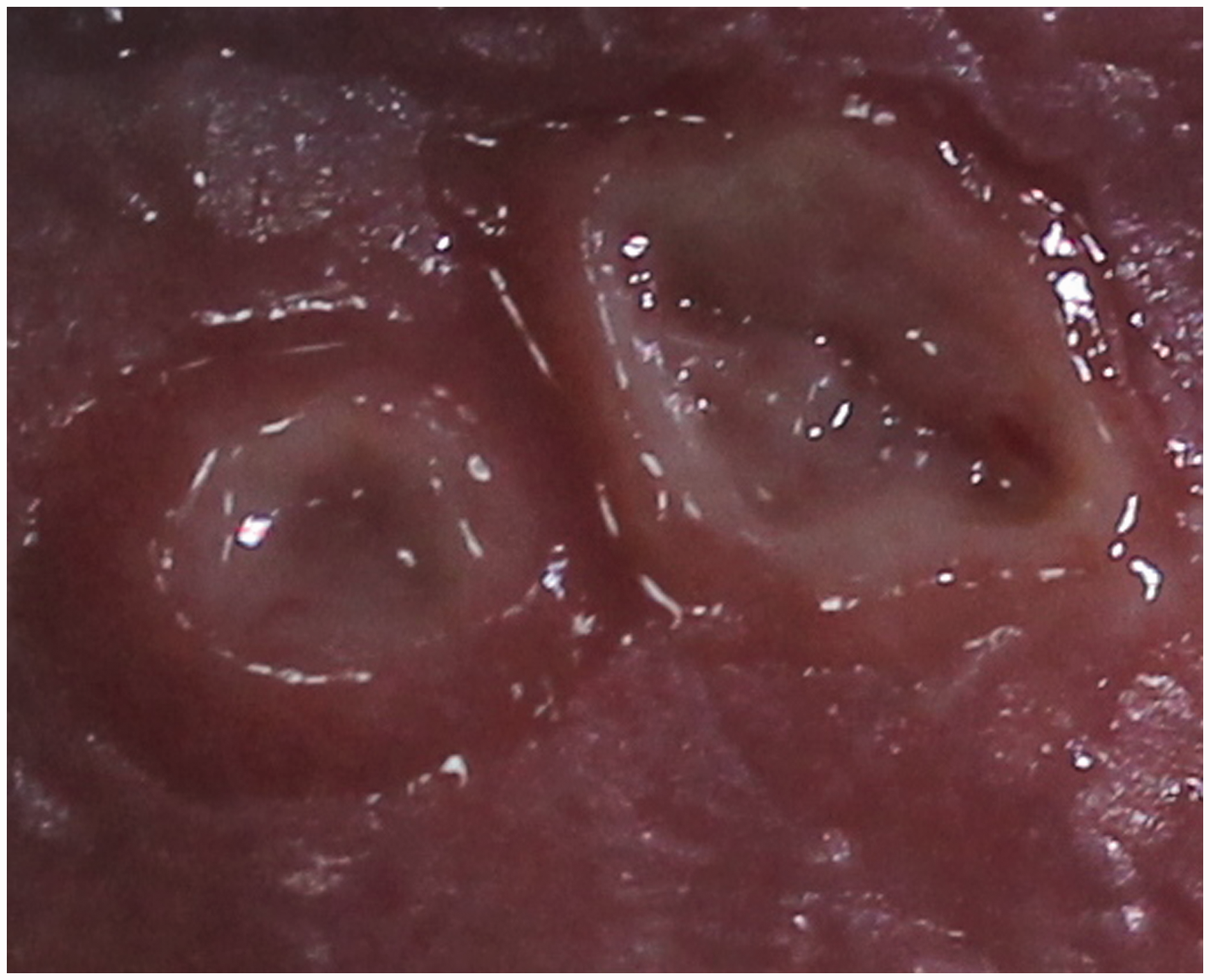

Key Learning points
Chancroid as a cause of GUD is rare in the developed world but still occurs and should not be forgotten In cases of GUD where swabs for HSV and syphilis tests (PCR/serology/dark ground microscopy) are negative, it is important to consider chancroid in the differential. Single-dose azithromycin is effective in treating chancroid and should be considered in the treatment options.
Footnotes
Conflict of interest
The authors declare no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.