
Abstract
Summary
Between July 2005 and January 2006 we evaluated 1248 Paraguayan active duty military volunteers. Participants provided a blood sample for HIV testing and answered an anonymous survey. HIV seroprevalence was 0.4% (5 of 1248) among participants. The median age at first sexual intercourse was 16 years. Only 14.8% of participants reported condom use with every sexual encounter. Military students used condoms the most. Participants older than 45 years, compared with younger participants, had a fourfold (adjusted odds ratio 4.3) increased risk of not using condoms. Men were less likely to use a condom, more likely to practice anal intercourse, and had more sexual partners than women. Officers and non-commissioned officers were identified to have a twofold (as measured by adjusted odds ratio = 2.00 and 2.22, respectively) increased risk of having more than two sexual partners in the last month compared with students. Both officers and non-commissioned officers were twice as likely as students to practice anal intercourse. Despite the high-risk behaviours reported by those surveyed, HIV seroprevalence in active duty personnel was low. Future efforts should emphasize on the correct condom use keeping focus on the high-risk behaviours of groups at risk, and on routinely testing the military personnel for HIV.
Keywords
Introduction
More than three decades after the beginning of the acquired immunodeficiency syndrome (AIDS) epidemic, reducing high-risk sexual behaviour remains a vital component1,2 of human immunodeficiency virus (HIV) prevention, even in 2013, when vaccines are not yet available 3 and pre-exposure antiretroviral prophylaxis is neither completely effective nor accessible for high-risk groups.4,5 These factors, coupled with the high percentage of various HIV-infected populations unaware of their status,6,7 make imparting healthy sexual practices on high-risk groups important. One group at particular risk is the military.
One shared characteristic of many soldiers throughout the world is young age, a high-risk demographic for acquisition of sexually transmitted infections (STIs). 8 In addition to young age, those serving in the military share other traits and risk factors, further adding to their overlooked high-risk status for HIV infection. 9 Military personnel are overwhelmingly men and frequently travel far from home and their partners, increasing the opportunities to access commercial sexual workers (CSWs). In the United States, it has been studied that relocation increases the risk of HIV infection, especially when military personnel are deployed to areas with high HIV rates. 10 The steady income associated with such deployments, mixed with the excitement of new surroundings and people, creates a scenario that may lead to increased risk taking such as consumption of mind-altering substances that may lead to unsafe sexual behaviours. 11 Sadly, when such behaviours lead to the spread of HIV, it results in increased instability to an already destabilized area. HIV infection in deployed US personnel not only affects the individual soldier but may also impact a country's security and the health of the local population.12,13
In Paraguay, since 1990, the National AIDS/STI Control Program (PRONASIDA in Spanish), under the direction of the Ministry and Public Health and Social Welfare, has been the principal entity in charge of Paraguay's response to AIDS. PRONASIDA provides healthcare to HIV/AIDS patients, offering counseling and antiviral treatment when necessary. This programme also administers the screening programme for recruits and military personnel from the Armed Forces of Paraguay. PRONASIDA has conducted an HIV-seroprevalence study on high-risk subjects: female commercial sexual workers (FCSWs) and men who have sex with men (MSM). 14 There, 2.8% FCSWs and 13% MSM were identified to be newly HIV-infected during the study period.
Little is known about HIV prevalence in active duty military personnel in Paraguay, but some data exist in Brazil, where more than 30,000 conscripts were studied. 15 In that study, increased risks of HIV infection with lower socio-economic and education levels were noted. Those of lower socio-economic class were reported to have higher levels of sexual activity, more sexual partners, and an earlier age of sexual debut. 15 Similar results have been identified in other regions, such as Thailand. 16
As part of an ongoing collaboration among PRONASIDA, the Paraguay Army Command Forces, and The Naval Medical Research Unit No. 6– Lima, Peru (NAMRU-6), we conducted a research study evaluating HIV seroprevalence and sexual behaviour in an active duty military population. Aims of the study included delineating which specific high-risk behavioural practices were common and characterizing which segments of the armed forces were particularly at risk.
Methods
The Armed Forces of Paraguay are organized into three commands, all under the Armed Forces Command and the Joint Chiefs of Staff: Army, Navy, and Air Force. The Army is divided into Infantry, Cavalry, Artillery, Engineering, and Communications. Those serving in any of the Armed Forces were divided into these broad categories: officers, enlisted/non-commissioned officers (NCOs), and students/cadets. Officers are the leaders of the military structure and are commissioned by the government. Enlisted/NCOs are workers and technical experts in different military areas like intelligence, weapon system, personnel and others (formerly called sub-oficiales in Paraguay).
Study population and participant enrollment
A cross-sectional HIV seroprevalence and behavioural survey was conducted between July 2005 and January 2006 by PRONASIDA and the Army Forces Command of Paraguay on active duty military personnel. Volunteers were enrolled in military detachments of Asuncion, Central, Ciudad del Este, Encarnacion, Paraguari, and Mariscal Estigarribia (El Chaco Area), where Army, Navy, and Air Force bases were located (see Figure 1). Inclusion criteria were active duty service for at least three months, 18 years of age or older, and freely provided consent. Recruits have less than three months in active duty service and were not included in any category of this study.
Map of Paraguay that includes the cities where this study was performed.
A sample size of 1248 subjects was calculated using the single-proportion sample size formula (Epi Info). The total active duty military population in the country was 12,561, with an estimated HIV seroprevalence of 1%. A precision of 1% with a confidence level of 99% and two tails for design effect was sought. Sampling distribution was not probabilistic. Regions of the whole country were selected following geographical accessibility, presence, and number of active military units of any army force. Regions selected were Eastern area (Ciudad del Este), Southern area (Encarnación), Central area (Asunción, Central, and Paraguari), and El Chaco area (Mariscal Estigarribia) (Figure 1). The Northern area of the country was not included (Concepcion). If two units from the same force existed in the visited geographical area, one of them was randomly selected. Inside these regions, units were selected according to the number of active military, as per information provided by the Paraguayan Armed Forces authorities. All military personnel present upon the time the research team visited the unit were invited to participate in the study. Only volunteers were included without any randomization process. At each unit, subjects were enrolled until the unit quota was obtained. If more volunteers wanted to participate, PRONASIDA counselors took care of them and if necessary performed an HIV test. Those were not included in the research protocol. Personnel who were not present at the headquarters visit were not included in the study. Sampling was conducted across 27 different military installations. Median 31 participants, range (2–320). All three categories of personnel (students, NCOs, Officers) were not present (or did not participate) at all installations. Students/cadets were only present in the Militar Academia for Officers and in the Training Institute for NCOs.
Trained bilingual (Spanish and Guaraní) personnel from PRONASIDA recruited the volunteers in selected military detachments. Complete confidentiality was assured based on a signed document provided by The Commanding Officer of the Military Forces. He also designated a project counterpart as a liaison in every military detachment located in the capital city and in the other regions of the country. PRONASIDA personnel explained to the commanders in each unit that subject participation was voluntary.
As per request of the Armed Forces, no printed materials were used to recruit the subjects. The invitation was done through oral announcements provided by trained personnel of PRONASIDA. At an auditorium, all military personnel received a briefing on the details and objectives of the study using a Naval Medical Research Center (NMRC) Institutional Review Board (IRB)-approved PowerPoint presentation. Counselors provided information about HIV infections and STIs, emphasizing prevention and explaining that many STIs are treatable. Then, each attendee went to a private room without the presence of military staff, where they were invited to participate. Personnel who did not wish to participate were allowed to leave the private room following the description of the study. This made it difficult for anyone to know who was participating in the study and minimized the potential for coercion. The number of refusals was not recorded.
Military personnel who wished to participate were informed about the study and signed the consent form. If the participant was not able to read or write, the counselor asked another participant to come in the room to be a witness and read the informed consent to the participant. In these cases, the consent form and the questionnaire were read aloud and signed with an X or his/her fingerprint. After this process, the witness left the room. A copy of the informed consent document (ICD) was given to each participant.
A confidential one-on-one interview was conducted using the questionnaire, and a blood sample was taken. The survey was organized into two sections: (1) personal background and (2) information on sexual behaviour. An additional form recording military institution, gender, rank, occupation, and identification code was used. In order to preserve confidentiality, it was not attached to other study documents. The blood samples and questionnaires were delivered to PRONASIDA in Asuncion.
Complete access to every person from each detachment was challenging, especially in border regions where specific units were often on patrol and not available to the researchers. In such cases, sampling was completed with personnel from other units. Due to the challenges of not knowing in advance the number of personnel present and the percentage that would want to participate, enrollment occurred until a pre-determined number of participants were recruited.
Sample collection and management
A 4-cc blood sample was collected in an EDTA tube and frozen as soon as possible at −20°C. All samples were identified solely by study ID number. Once samples were received at PRONASIDA, they were tested for HIV antibodies by third-generation enzyme linked immunosorbent assay (ELISA Bio-Rad, Hercules, CA, USA) with confirmatory Western blot (WB) as previously described. 17 The sample was centrifuged to separate two plasma aliquots; one was used to perform the HIV tests (ELISA, WB) and the second was kept at −20°C, as back-up. The samples reported to be positive on the first ELISA underwent a second ELISA. Samples with duplicate positive ELISAs were confirmed by Western blot using FDA-approved testing kits (Calypte Biomedical, Alameda, CA, USA).
Management of results
ELISA-positive participants were encouraged to provide another sample for confirmation and were subsequently referred to the PRONASIDA medical health centre for counseling and test results. All participants received their results away from the military bases, at the PRONASIDA medical health centre. At this location, treatment and notification were given apart from any other military personnel in order to ensure that no other member of the military unit, including commanding officers, were aware of participants' HIV status or treatment.
All consent forms and questionnaires were kept at PRONASIDA, and copies were shipped to NAMRU-6. All data collected were not linked to any personal identifiers, such as names or personal identification numbers. All ICDs and questionnaires had a unique identifier (study code). If a person came back for his/her results, he/she was referred to PRONASIDA.
Ethical considerations
The study protocol was approved by the Ministry of Health and the Armed Forces of Paraguay, the NMRC IRB (Protocol # NMRCD.2002.0006), and the non-governmental organization Rayos de Sol IRB of Paraguay, in compliance with the Helsinki Declaration and all applicable federal regulations governing the protection of human subjects.
Statistical analysis
Data entry was performed at PRONASIDA using EPI INFO version 2000. The analysis was performed using SPSS Statistics 17.0 for Windows (SPSS Inc, Chicago, IL, USA).
The proportions of positive results were calculated for each variable with 95% confidence intervals (CI), and proportions were compared using a Chi square test (χ2). Continuous normal distribution data were expressed in terms of mean values (±1 standard deviation [SD]). Non-normal distribution data were expressed in terms of median and percentiles 25th (Q25) and 75th (Q75). Graphic boxplots were included representing the middle 50% of the cases, with the whiskers of the box indicating the expected top and bottom 25%. The outliers were depicted with “O”s, above or below the whiskers.
Continuous variables with a normal distribution were compared using the Student's t-test; otherwise, the Mann-Whitney U or Kruskal-Wallis (H) test was applied. p Values ≤0.05 were considered statistically significant. Associations of risk factors were expressed as adjusted odds ratios (AOR) with CI 95%. Variables with more than two categories were re-codified in order to analyze sexual behaviours at risk for STI and HIV acquisition among military personnel. These variables were made dichotomous.
Demographic characteristics and risk behaviour in military personnel according to military rank. Paraguay, 2005–2006.
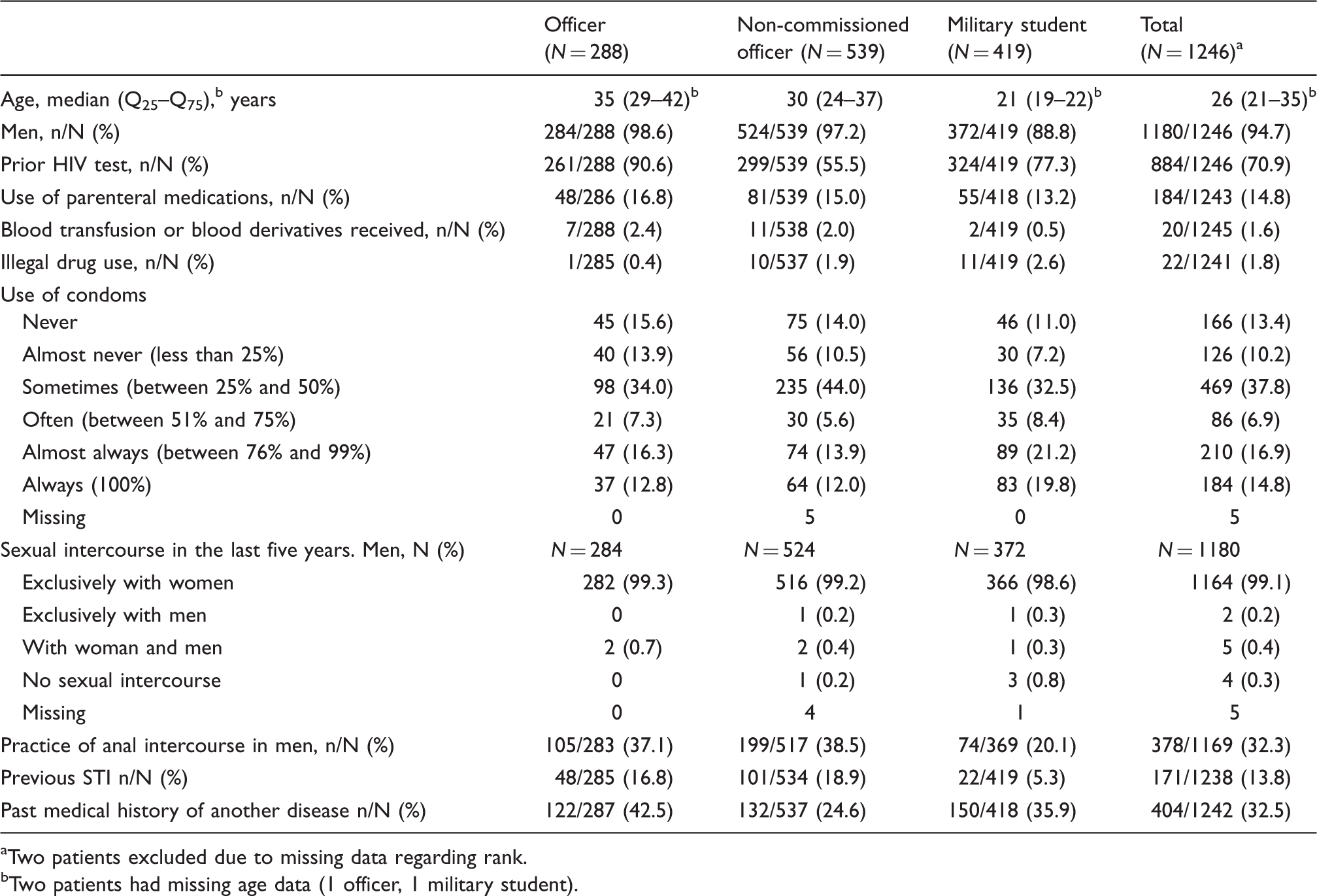
aTwo patients excluded due to missing data regarding rank.
bTwo patients had missing age data (1 officer, 1 military student).
Demographic characteristics and risk behaviour of HIV positive active duty military personnel. Paraguay, 2005–2006.
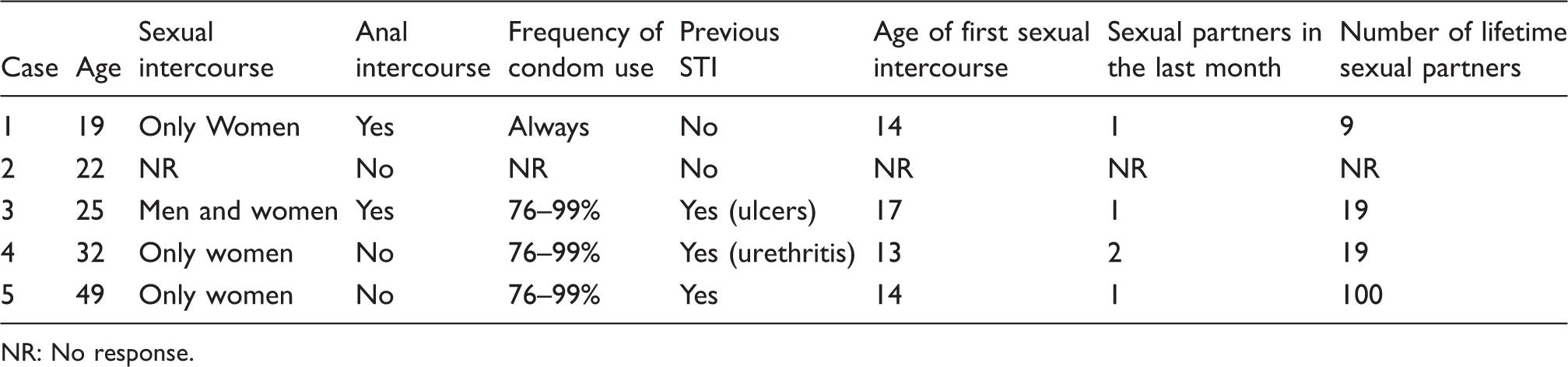
NR: No response.
Results
Study population
A total of 1248 military-active duty personnel were enrolled, and 1182 (94.7%) were men. Nine hundred and seventy five (78.1%) were from the Army, 238 (19.1%) from the Navy, and 35 (2.8%) from the Air Force. Demographic characteristics are presented in Table 1 according to military rank. The median age was 26 years, the mode was 20 years, and the range was between 18 and 58 years. Figure 2 shows these distributions by age and military rank. The proportion of women personnel differed significantly by military rank (χ2 = 44.8, p < 0.001). The largest proportion of women was among students (11.2%); among the NCOs and officers, the proportion was lower (2.8% and 1.4%, respectively).
Distribution of age according to military rank and gender. Paraguay, 2005–2006.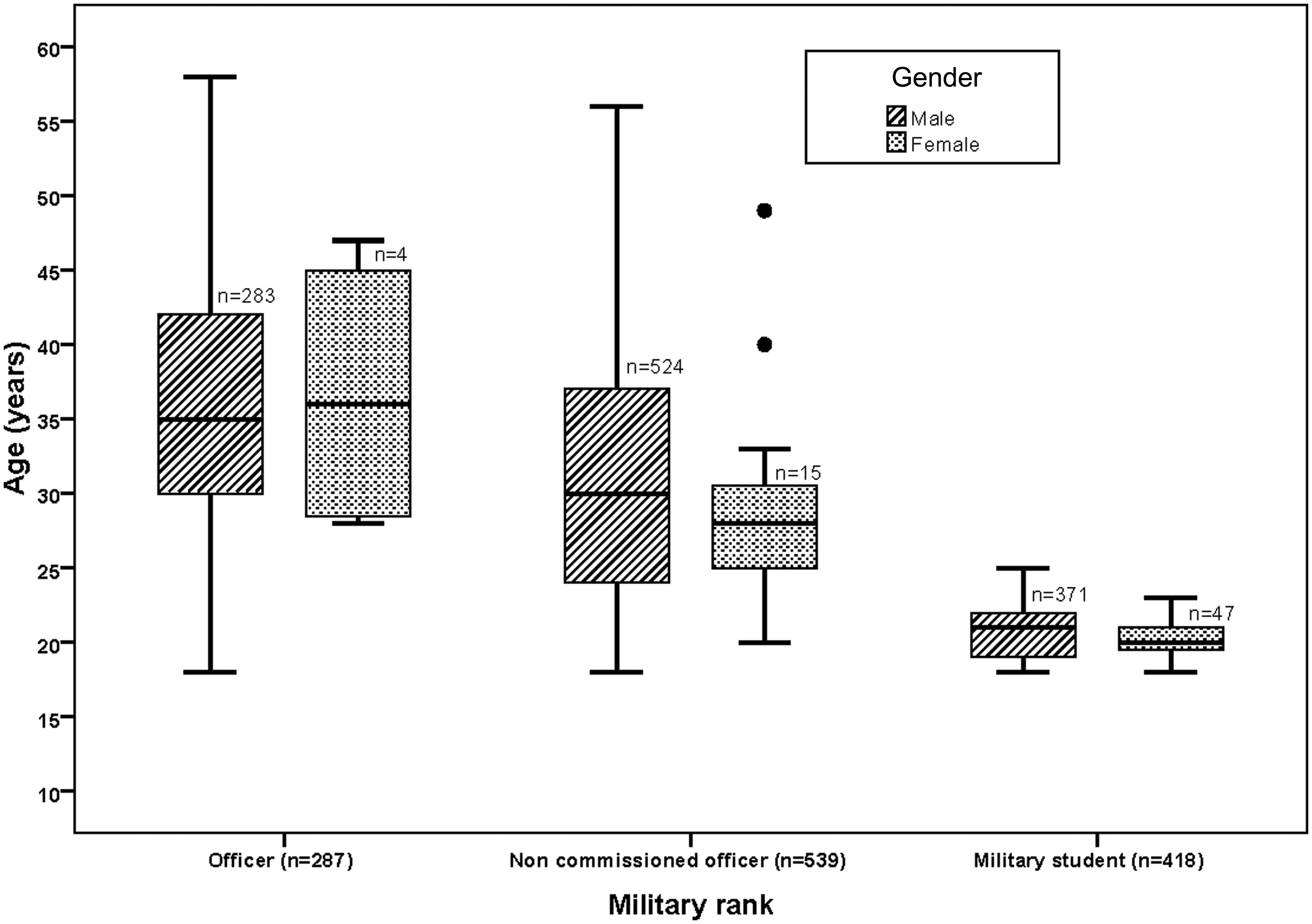
HIV results
Risk behaviour in military personnel by military rank. Paraguay, 2005–2006.
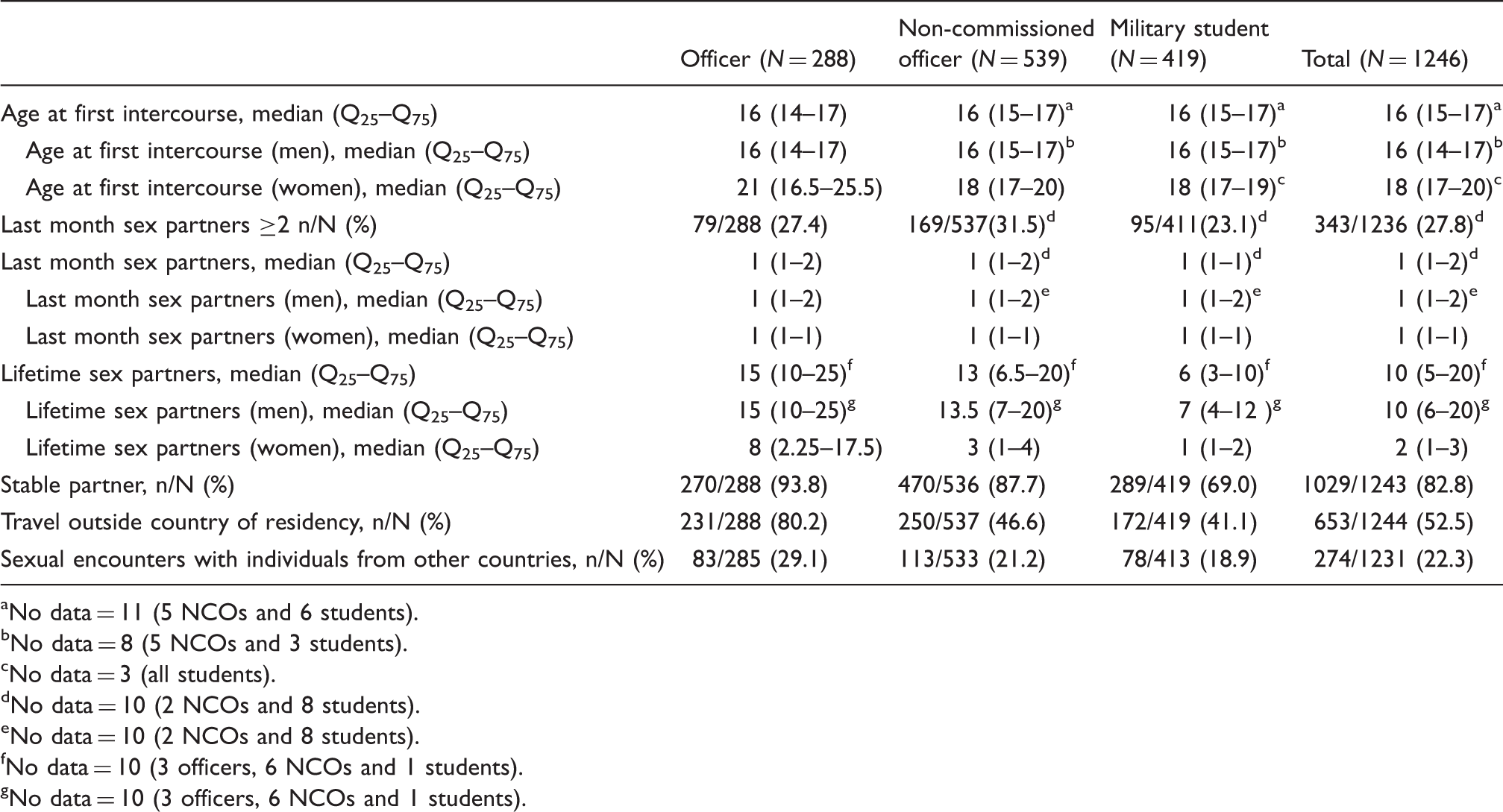
aNo data = 11 (5 NCOs and 6 students).
bNo data = 8 (5 NCOs and 3 students).
cNo data = 3 (all students).
dNo data = 10 (2 NCOs and 8 students).
eNo data = 10 (2 NCOs and 8 students).
fNo data = 10 (3 officers, 6 NCOs and 1 students).
gNo data = 10 (3 officers, 6 NCOs and 1 students).
Risk behaviour
A higher percentage of officers reported having a previous HIV test compared with NCOs, and students (χ2 = 124.9, p < 0.001: Table 1). By gender, female NCOs had this test done more than men, 93.3% (14/15) versus 54.4% (285/524), respectively (χ2 = 8.9, p < 0.003). There was also a significant difference among students, where a higher proportion of men compared with women had this test done, 79.3% (295/372) versus 61.7% (29/47), respectively (χ2 = 7.4, p = 0.007).
No differences were reported between various military ranks regarding receiving parenteral medications (χ2 = 1.8, p = 0.40), blood transfusions, or derivatives in the last 5 years (χ2 = 5.3, p = 0.07). Twenty-two participants (1.8%) reported using illegal drugs over the past 5 years (χ2 = 5.1, p = 0.08). None described intravenous drug use (Table 1).
When asked about the use of condoms, 13.4% (166/1243) reported never using this form of prevention, with no statistical significant difference among various military ranks (χ2 = 3.5, p = 0.17). Lack of condom use occurred more frequently in women than in men, 33.3% (22/66) versus 12.2% (144/1177), respectively (χ2 = 24.0, p < 0.001). The use of condoms in every sexual intercourse was reported in 14.8% (184/1243) of all surveyed, with students doing this more (19.8%) than officers (12.8%) or NCOs (12.0%) (χ2 = 12.5, p < 0.002; Table 1).
With respect to anal intercourse (either receptive or insertive), 32.3% (378/1169) of men and 10.6% (7/66) of women reported this practice (χ2 = 13.7, p < 0.001). Among men, this practice occurred more commonly in officers, and NCOs, compared with students (χ2 = 37.3, p < 0.001). Out of 368 men who answered the question on the anal sex modality they performed, 94.6% (348) were active (insertive), 4.9% (18) were passive (receptive), and 0.5% (2) practiced both modalities, with no significant difference per military rank.
Officers and NCOs had a higher proportion of history of STIs, 16.8% and 18.9%, respectively, compared with 5.3% of students (χ2, p = 0.001; Table 1). No significant difference by gender was reported. The median age at first sexual intercourse was 16 years, with no significant statistical difference between military ranks (H = 0.6, p = 0.72). Median age of initial sexual intercourse among men (16 years) was younger than in women (18 years) (U = 12685.5, p < 0.001). The number of sexual partners in the last month was higher for officers and NCOs compared with students, Q75 = 2 and 1, respectively (H = 19.1, p < 0.001). The median number of lifetime sexual partners for all participants was 10, with higher totals associated with higher rank (Figure 3). The number of lifetime sexual partners was lower in women (U = 8088.5, p < 0.001). Officers traveled abroad the most in comparison to NCO personnel and students (χ2 = 118.3, p < 0.001). The proportion of NCO personnel and students that traveled abroad did not differ significantly.
Number of lifetime sex partners by military rank and gender. Paraguay, 2005–2006.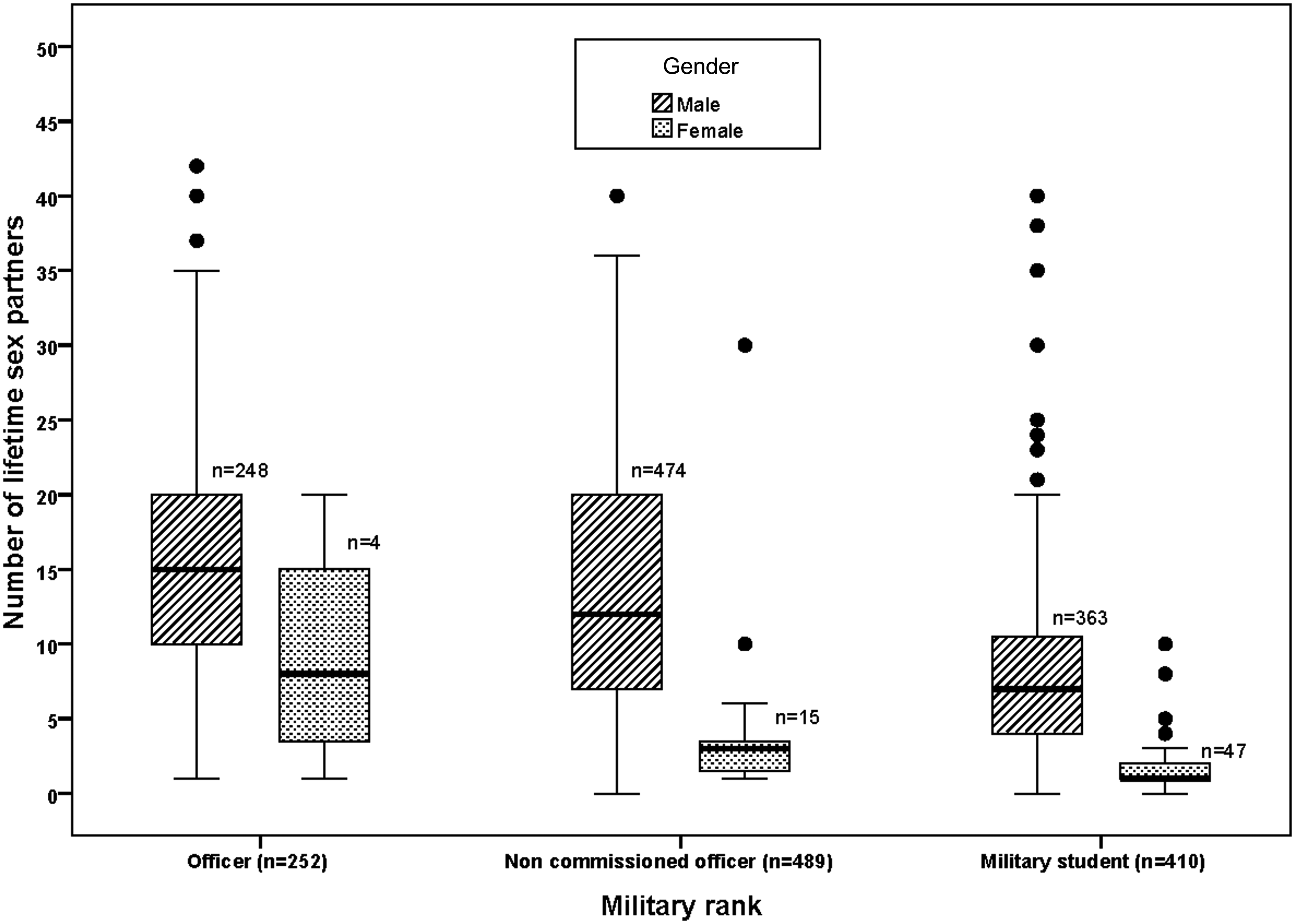
Adjusted odds ratios for high-risk sexual behaviours among military personnel. Paraguay, 2005–2006.
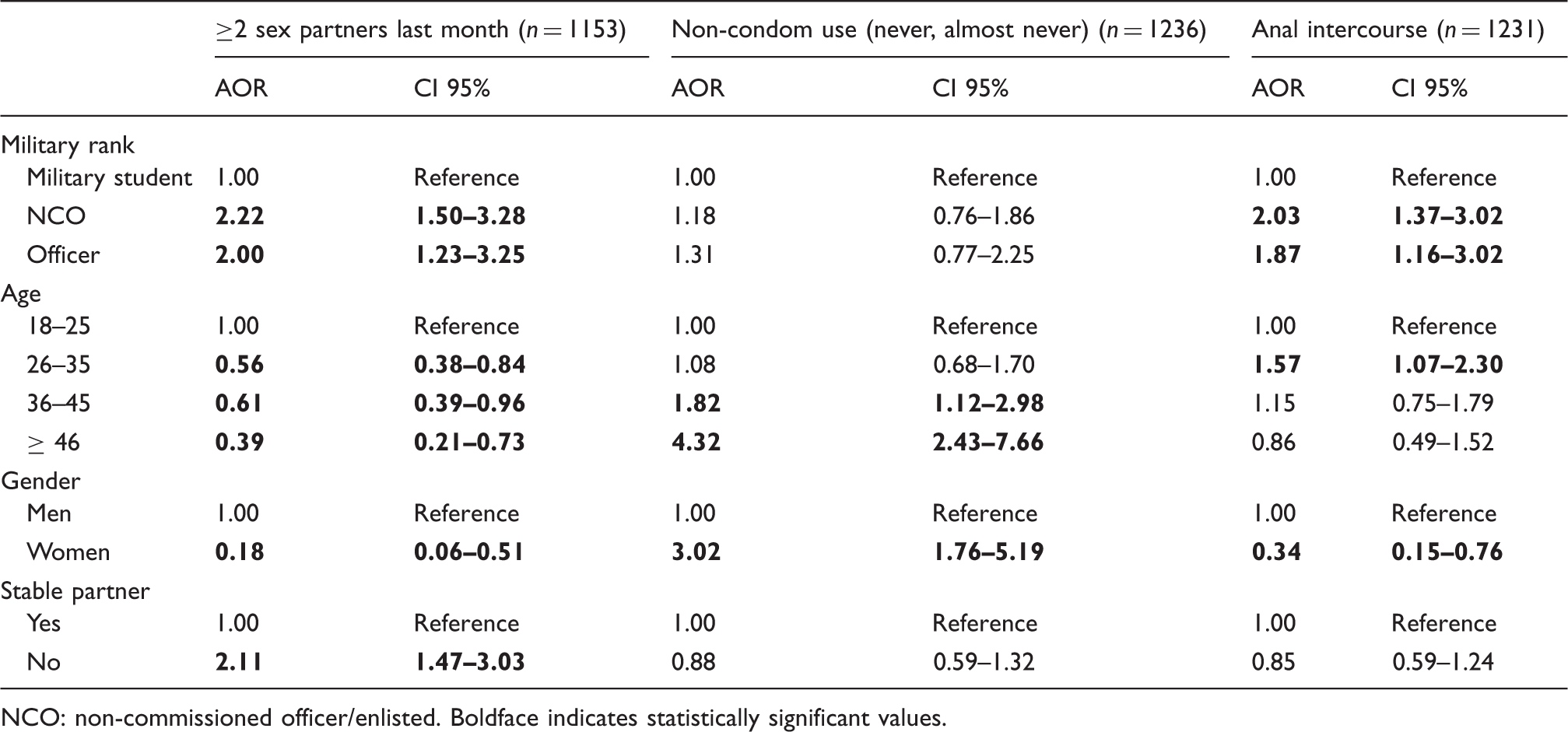
NCO: non-commissioned officer/enlisted. Boldface indicates statistically significant values.
AORs controlling for military rank, age, gender, age at first sexual intercourse, and presence of a stable partner were calculated to investigate likelihood of certain high-risk behaviours (Table 2). For the outcome variable, “having more than one sexual partner in the last month,” the odds for officers and NCOs answering affirmatively were twice that for students. Those between 26 and 35 years at the time of the interview were 44% less likely to have more than one recent sexual partner compared to the 18- to 25-year-old group; furthermore, those older than 45 years were 61% less likely to have multiple recent sexual partners than those between 18 and 25 years. The odds for women having more than one sexual partner in the last month was lower than the odds for men (AOR 0.18). Those participants without a stable partner were twice as likely to have more than one sexual partner in the prior month (Table 2).
The behaviour, “non-use of condoms,” was associated with older age groups. People between 36 and 45 years had almost twice the likelihood of not using a condom than those between 18 and 25 years. Persons older than 45 years were four times less likely to use a condom compared to those between 18 and 25 years. In addition, women were more likely to not use a condom than men (AOR 3.0; Table 2). Officers and NCO personnel were both nearly twice as likely to have practiced anal intercourse as students (Table 2). No differences were found in the logistic regression results for each outcome by three methods (Appendix 1). Clustering has no impact on the results reported in Table 2.
Discussion
Our results indicate that many Paraguayan military personnel have unsafe behavioural practices that may predispose them to acquire STIs, including HIV infection. Nevertheless, the disciplined setting provided by the military provides an environment conducive to prevention campaigns and follow-up surveys.
HIV results
Prior to this study, there has been a paucity of published data on HIV and other STI risk factors in the Paraguayan military. This serosurvey discovered only five HIV infections in 1248 active duty military Paraguayans in 2006. Although this is a low absolute number of infections, the data will be complemented by future studies in the same population by our group. Our results show a low prevalence of HIV infection in the military population, similar to other results reported in developing countries' soldiers/recruits.18,19 The prevalence among this population is as low as other low-risk Paraguayan demographic groups, such as the general women population and pregnant women.
Although we used a single-proportion sample size formula, the representativeness of study sampling to all Paraguayan military was not ideal. Due to military security reasons we failed to know the exact number of military personnel present or absent on the day of our visit to each city/detachment. Random sampling was not possible, by which everyone would have had the same option to participate in the study. The obtained results could have been biased to a certain degree since it would have been ideal to have a list of people present and draw names at random instead. Anyone who knew that he/she was positive might have refused to participate, and those who were absent (in the border area or on duty) failed to have a chance to participate.
We do not know the number of participants that were briefed but refused to be tested. Military members not wishing to participate left the private room following the information about HIV infections and STIs, and thus were not counted by our study personnel.
Risk behaviour
In Paraguay, there is no law forbidding discrimination based on sexual orientation, but the government is working on a bill. Likewise, the Paraguayan Armed Forces have no policy either for or against homosexuality, but it is not hard to infer that active duty personnel could feel uneasy disclosing homosexual behaviour around military colleagues, especially superiors, as has been noted in other countries' militaries. 20
Interestingly, only two men admitted to having sex with other men, but when asked about anal intercourse, 20 men admitted to being passive (receptive) partners during this type of intercourse without significant differences per military rank. This led us to conclude that the number of MSMs was underreported in this population. Others have described how some men live in “secretive bisexuality” or consider themselves heterosexual because, different from some soldiers in our study, they took the insertive role in anal or oral sex. 21 This may have even extended to completing our survey, although we took extra measures to ensure complete confidentiality. In the United States, this behaviour has been extensively characterized in bisexual black men who do not disclose their sexual activities, a phenomenon called being “on the down low.”22,23 Although initially described in black men, other studies have noted similar behaviour in other ethnic minorities in the United States. 21
Sometimes military rank was an important determinant of high-risk behaviours. In one study from Angola, possessing more resources, money, and freedom was reported to permit higher-ranking officers to obtain more sexual partners. 24 The fact that officers were more likely to have received a prior HIV test than the younger-aged NCOs or students was most likely secondary to the officers' longer time in an environment that provided HIV testing. In addition, officers' education level most often exceeds those with lesser rank and is frequently associated with a better socio-economic status and more opportunities for sex.11,24 On the other hand, low rank and educational level can also be a risk factor, as Brazilian or Asian soldiers with a lower educational level had a higher HIV prevalence than those who completed high school.16,18 It is important to mention that higher number of sexual partners was associated with higher rank, but in this specific case rank might be a confounder because higher ranking officers are more likely to be older and therefore likely to have more sexual partners.
Male officers and NCOs practiced anal sex more frequently than other groups, and 95% of individuals interviewed were active (insertive). The higher numbers of STIs and lifetime sexual partners in officers was counterbalanced by officers' higher rates of having a current stable partner. In addition, officers traveled abroad more frequently than NCOs and students. As stated before, 25 foreign travel provides an opportunity to have sexual contact, with increased risk associated with return visits to the same location. 26 Male gender, single status, age <20 years, and traveling without a partner were also listed as factors associated with increased exposure.25,27
Substance abuse is also a notorious predictor of risky sexual behaviour.19,24 In our study, officers were less likely to use illicit drugs (nasal, oral, or inhaled) than students. Others have also reported that the use of illicit drugs begins at a young age. 19 Decreased use of illicit substances often coincides with the acquisition of additional professional and personal responsibilities. Even though the survey was coded, preventing us from identifying affirmatively answering respondents, the possibility remains that some did not answer this question truthfully and that the actual prevalence of drug use was higher.
Potential clustering of high-risk behaviours could be a limitation in our study. To rule out this possibility, we ran cluster-based SE estimation and no statistically significant differences were found with a robust SE estimation (empirical SE estimation).
It has been previously reported that a consistent educational programme about sexual behaviour results in lower rates of unsafe sexual practices. 26
Educational efforts should support correct condom use, which may be the best method for preventing most STIs, including HIV/AIDS. 1 Correct and consistent condom use has been reported to be effective in preventing transmission of HIV and other STIs. 28 Although women reported less condom use than men in our study, this result should be considered together with our finding that more women reported being in monogamous relationships and, therefore, are not exposed to the same amount of risk as someone with multiple partners. Though the efficiency of the condom use to prevent STIs is already proven, it is highly important to promote the condom use with occasional partners especially if there will be anal intercourse.
Although some researchers prefer to dichotomize the variable “condom use” in favour of allowing normal data distribution and therefore a less complicated analytic method 29 a variable divided in six strata was used for this manuscript, to be described as thoroughly as possible. 30 Usually dichotomizations by other authors consider “consistent” use as use in 100% of sexual contacts; any other value is considered “inconsistent.”
Military populations may be ideal for educational strategies that minimize risky behaviours. Messages that could be conveyed include the importance of barrier precautions with anal intercourse or during intercourse with somebody of unknown HIV status. Furthermore, the proper use and storage of condoms can be emphasized. Some people are unaware that improper storage and the use of non–water-based lotions can weaken the condom; however, failures due to condom breakage have been reported to be minimal. 31 Spermicides are not effective in preventing many STIs. In fact, they may increase risk for HIV and other STI transmission. 32
The fact that our data were collected 6–7 years ago is a weakness of our study. HIV seroprevalence in the general Paraguayan population has not changed from 0.3% (2005–2012, according to PRONASIDA-MoH Paraguay – unpublished data). No other data in the ensuing years have been published about high-risk sexual behaviour or HIV rates in the Paraguayan military. At least one major change has occurred within the Paraguayan military and police force since our study: increased sexual behaviour risk factor education and condom availability have been made possible by the Global Fund and the Armed Forces Committee for Prevention and Control of Sexually Transmitted Diseases.
In future studies, we will aim to assess various preventive strategies, and measure soldiers' subsequent risk-taking behaviour and prevalence of HIV, as well as other STIs. Although our study revealed a low prevalence of HIV in the Paraguayan military in 2006, the many unsafe behaviours detected in the study may result in higher number and rates of HIV infection in the future. Educational efforts should be directed at active duty personnel in Paraguay in order to increase awareness of unsafe sexual behaviours and these efforts should target low- and high-ranking soldiers alike, as increased rank did not correlate with a decrease in risky behaviour.
Finally, efforts should emphasize on the correct condom use as a protective measure for all Paraguayan military members. It will also be important to consider whether establishment of a routine, periodic HIV screening programme among Paraguayan military personnel is acceptable and leads to increased detection of HIV infections and subsequent treatment.
Footnotes
Disclaimer
The views expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the Department of the Navy, Department of Defense, nor the U.S. Government. The study protocol was approved by the Ministry of Health, the Armed Forces of Paraguay, the Naval Medical Research Unit-6 Institutional Review Board (Protocol NMRCD.2002.0019) and NGO Rayos de Sol IRB of Paraguay in compliance with all applicable Federal regulations governing the protection of human subjects. Disclosure: None of the authors has a financial or personal conflict of interest related to this study. The corresponding author had full access to all data in the study and final responsibility for the decision to submit this publication. Copyright Statement: Eric S. Halsey and Tadeusz J. Kochel are US military service members, and V. Alberto Laguna-Torres, Julia S. Ampuero and Juan Perez are employees of the US Government. This work was prepared as part of their official duties. Title 17 U.S.C. § 105 provides that ‘Copyright protection under this title is not available for any work of the United States Government’. Title 17 U.S.C. § 101 defines a US Government work as a work prepared by a military service members or employees of the US Government as part of those person's official duties.
Acknowledgement
We thank Morgan Marks and Brett Forshey for their statistical support in the robust SE estimation. Maria Esther Gamero, Jane Rios, and Ruth Centeno for invaluable laboratory and technical support in the execution of the study. We express our gratefulness to Milagros Cifuentes for translation and editorial assistance of the manuscript.
Conflict of interest
The authors declare no conflict of interest.
Funding
This study was funded by the United States Military HIV Research Program (USMHRP), WORK UNIT NUMBER: 62787A.873.HB0002.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.