
Abstract
The knowledge of HIV incidence is essential to better understand patterns of HIV transmission. We estimated HIV incidence over 2010–2012 in the eastern European country of Georgia. Mathematical modeling using Spectrum software and assay-based recent infection testing algorithm were applied. The study included 1155 HIV patients newly diagnosed in 2010–2012 (84% of total diagnoses). Of them, 231 were determined to be recently infected on the recent infection testing algorithm. The proportion of recent cases did not differ between 2010, 2011 and 2012 (20.4% vs. 19.4% vs. 20.2%, p = 0.94). Both study methods derived comparable estimates ranging from 0.2 to 0.3%, which is up to twice as high as rates of new diagnosis reported in the same period. Despite the relatively stable HIV incidence over 2010–2012, the epidemic continues to grow because of the increasing gap between HIV-infected and diagnosed persons. Increased efforts are needed to reduce the number of people with undiagnosed HIV.
Keywords
Introduction
Knowledge about HIV incidence is essential for describing patterns and trends of the epidemic. Accurate information on the incidence has valuable applications in surveillance, programme planning and impact evaluation. The gold standard for estimating incidence is longitudinal follow-up of a cohort of HIV-negative individuals, who are tested for HIV at regular intervals. Surveillance of such type is difficult to establish and maintain even in resource-rich settings, it is costly and prone to selection, retention and intervention biases. Alternative approaches for estimating HIV incidence include mathematical modeling and the use of laboratory assays to detect biomarkers of recent HIV infection. 1
It has been shown that modeling approaches can provide reasonably accurate indirect estimations of HIV incidence. A major disadvantage of this approach is the use of prevalence data, which is challenged by the growing influence of antiretroviral therapy (ART). Increase in the mean survival influences prevalence trends further complicating the relationship between HIV incidence and prevalence. The laboratory-based approach uses cross-sectionally collected specimens to estimate HIV incidence based on detection of recent HIV infection. This approach is termed a recent infection testing algorithm (RITA) and describes a laboratory assay, or a combination of one or more assays and clinical information, which is used to classify a case of HIV infection as being either recently acquired or not recently acquired. 2
Work on HIV/AIDS in Georgia was started in 1984 with the establishment of first HIV laboratory in the country. Currently, there is well-established surveillance system built on the principles of second generation HIV surveillance. 3 The main components of the surveillance are voluntary and confidential HIV testing and counseling, HIV/AIDS and mortality case reporting and bio-behavioural surveys (BBS). Currently, HIV testing activities include targeted screening of most-at-risk populations (injection drug users [IDU], men who have sex with men [MSM], female sex workers [FSW], prisoners), HIV indicator disease-guided testing, universal screening of pregnant women and mandatory screening of donated blood.
The first case of HIV infection in Georgia was identified in 1989. As of December 31, 2012, a total 3642 cases of HIV infection were reported. Similar to other former Soviet Union (FSU) countries the HIV epidemic in Georgia has been driven by IDUs, accounting for 54% of all reported cases. However, recent trends indicate an increase in the proportion of sexually-acquired infections. In 2011, for the first time since the start of the epidemic in the country, the proportion of newly reported heterosexually-acquired infections exceeded the proportion of cases attributable to IDU. The annual number of reported HIV cases has risen each year. There was almost fivefold increase in the rates of new diagnosis from 2.3 per 100,000 in 2002 to 10.9 per 100,000 reported in 2012. Regional distribution of reported cases is not uniform; the most cases per 100,000 inhabitants were registered in regions of Samegrelo and Achara, followed by the capital city of Tbilisi and Imereti regions. Latest BBS data indicate that HIV prevalences among IDUs and FSWs remain relatively low at −3% and 1%, respectively.4,5 There was significant increase in HIV prevalence among MSM from 3.7% reported in 2007 to 13% in 2012.6,7 Georgia has made substantial progress in providing ART. Since 2004, through the support from the Global Fund, Georgia ensured universal access to ART to all patients in need and has the highest ART coverage in Eastern Europe. 8
Until recently, assessment of the state of the HIV epidemic in Georgia has been based on prevalent HIV cases, with information on HIV diagnoses and data from BBS being primary sources for epidemic analysis. Undoubtedly, the prevalence is a very important figure for measuring disease burden, but it indicates historic spread rather than existing trajectories. With the universal availability of ART in Georgia, people with HIV live longer resulting in changes in prevalence, which may not be related to changes in incidence. Moreover, it has been shown that populations with high incidence of the infection do not necessarily show high prevalence of the disease. 9 Therefore, the knowledge of HIV incidence is essential to better understand patterns of HIV transmission in the country and to provide rational basis for targeting response interventions. The objective of this study was to estimate HIV incidence in Georgia during 2010–2012 by RITA-based approach and mathematical modeling. We also evaluated factors associated with recent HIV infection.
Methods
Design
We conducted a retrospective study to estimate HIV incidence in Georgia within the national case-based HIV surveillance. The study was conducted at the Infectious Diseases, AIDS and Clinical Immunology Research Center (IDACIRC), which is the country’s reference institution for HIV diagnosis, treatment and care. The study utilized remnant HIV diagnostic specimens stored at IDACIRC and the data routinely collected at the Center for surveillance purposes or as part of standard clinical care.
Assay-derived RITA combined with clinical and laboratory data were applied to estimate HIV incidence. We used the Aware™ BED™ EIA (BED) as an assay of recent infection. Data on age, gender, mode of transmission and region of residence were available from the national database operated by IDACIRC since 1989. We additionally searched HIV case investigation records for the evidence of previous positive HIV tests delivered outside the country. Clinical and laboratory data were abstracted from medical records using a standardized data abstraction form. The study included newly diagnosed HIV infections among persons aged >15 years registered in 2010–2012.
HIV infection was defined as recent if individual had recent infection on the BED assay and did not have clinical, laboratory or historical evidence of longstanding infection (Figure 1).
Recent infection testing algorithm (RITA) for determining recent HIV infection.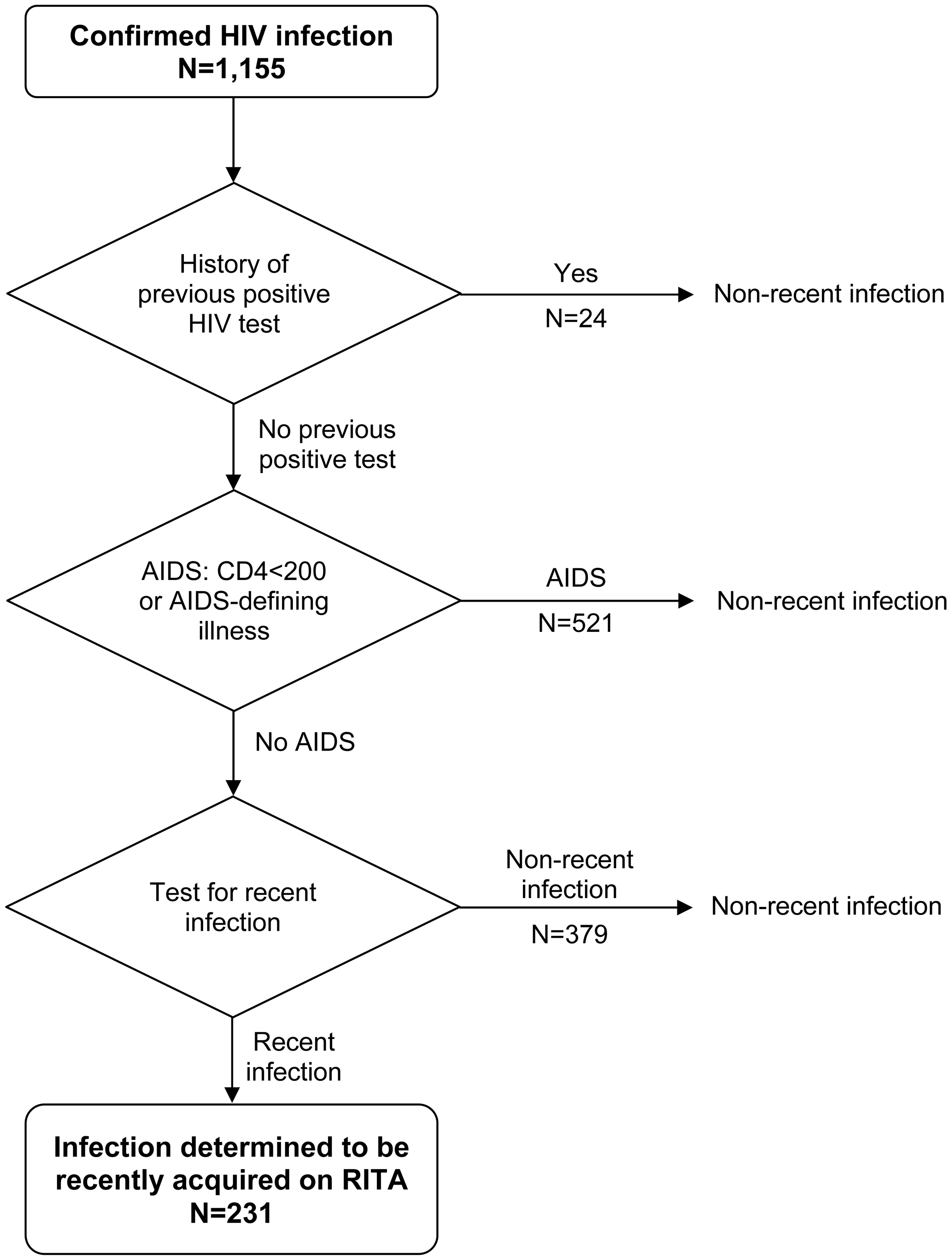
Evidence of longstanding infection included history of previous positive HIV test and diagnosis of AIDS, defined as CD4 count <200 cells/mm3 or presence of AIDS defining illness, 10 within 6 months of HIV diagnosis.
Laboratory procedures
The BED test was performed and interpreted according to manufacturer’s instructions. The principle of the BED test is based on the increasing proportion of anti-HIV specific IgG in total IgG following seroconversion. HIV-positive persons are classified as ‘recent’ seroconverters if their blood samples have a normalized optical density (OD) below a pre-set cut-off of 0.80.
Frozen serum specimens stored at –70°C at IDACIRC were thawed and inspected for suitability for BED testing. Of 1377 adult persons diagnosed in 2010–2012, frozen specimens from 1319 HIV-positive persons (95.8%) were available at the IDACIRC and 1155 (83.9%) were suitable for BED testing. Overall, 164 specimens were either grossly lipaemic, or haemolyzed or cloudy and were excluded in accordance with manufacturer’s instructions. Suitable specimens were initially run in single on the BED test. Specimens with OD <1.2 were tested again in triplicate to confirm their OD values. In confirmatory testing, if the OD of the specimen was ≤0.80, the specimen was considered a recent seroconversion.
HIV incidence estimation
HIV incidence was estimated using McWalter/Welte formula described in detail elsewhere. 11 Briefly, required inputs include (a) number of persons testing positive for HIV, (b) number of persons classified as recent on RITA, (c) number of persons testing negative for HIV, (d) the mean recency time of the assay for recent infection, (e) the false recent rate (FRR) of the assay for recent infection.
Inputs were derived from the current study, national HIV surveillance and from literature. The number of HIV-positive and -negative persons has been available from the national surveillance system. Overall, of 442, 418 and 517 HIV-positive individuals aged >15 years diagnosed in 2010, 2011 and 2012, samples from 358 (81%) 366 (88%) and 431 (83%) persons were suitable for RITA testing, respectively, and were included in analysis. According to National Center for Diseases Control and Public Health (NCDC) 90,078 in 2010, 99,331 in 2011 and 92,115 persons in 2012 were tested for HIV. We used updated mean recency period of 197 days estimated for BED from multiple HIV subtypes. 12
We estimated FRR within the current study from 462 specimens with known long-standing infection. Of them, 78 were classified as recent on BED −16.8%. In addition, we also used the external FRR of 5.7% reported by McDougal and colleagues. 13
Mathematically-modeled HIV incidence
We compared RITA-driven and modeling-based incidence estimates. The mathematically-modeled HIV incidence estimates were derived using Spectrum projection software version 4.47. 14 The software was developed to examine the consequences of current trends and future programme interventions in reproductive health. For HIV/AIDS field Spectrum is used to estimate key HIV indicators, including HIV incidence. The methodology and assumption used by the software is regularly updated based on the recommendations of UNAIDS Reference Groups on Estimates, Models and Projections.
Predictors of recent infection
Predictors of recent infections were assessed first in univariate analysis and then in multivariate logistic regression. Initial multivariate model included variables significant at p < 0.20 in univariate analysis. Variables significant at p < 0.10 were retained in the model along with those confounders, which was determined as at least 10% change in parameter estimates as compared to full model. Statistical analyses were performed using SAS v9.2.
Results
Study population characteristics.

Estimated HIV incidence.

95% CI: 95% confidence interval.
Among 231 patients classified as recent seroconverters 65 (28%) were IDUs, 121 (52%) were heterosexually infected individuals, 39 (17%) were MSM and 6 (3%) were infected either through blood transfusion or mode of transmission could not be determined.
Factors associated with recent HIV infections.

OR: Odds ratio; 95% CI: 95% confidence interval.
The strongest predictor of recent HIV in multivariate analysis was younger age. Persons younger than 30 years had significantly higher odds of having recent infection compared to any age category (odds ratio [OR] 4.17, 95% CI: 2.22–7.85, vs. age group of 50+; OR 2.82, 95% CI: 1.84–4.30, vs. age groups of 40–50 and OR 3.22, 95% CI: 2.18–4.75, vs. age group of 30–40). Odds of having recent infection was almost 4-times higher among MSM compared to IDUs and more than twice as high compared to heterosexually-infected persons. Being resident of Samegrelo region was inversely associated with the recent HIV (OR 0.50, 95% CI: 0.28–0.90).
Discussion
Our study shows that HIV incidence over the 2010–2012 period remained relatively stable. Estimates of both assay-derived RITA and Spectrum modeling corresponded fairly well with each other when we used locally derived FRR. The application of external FRR produced estimates up to four times over the observed prevalence in the country. 15 This is an implausible level of incidence and underscores importance of incorporating locally-relevant FRR in assay-based estimation exercises.
The most concerning finding of our study is that identification of HIV-positive cases lags behind the rate new infections occur. HIV incidence estimates produced in our study are up to two times higher than rates of new diagnosis reported in Georgia over study period. This situation contributes to increasing the number of HIV-positive persons, who are unaware of their infection. Indeed, recent analysis of the spectrum of engagement in HIV care showed that the major gap in the cascade occurs at the stage of HIV case detection. Analysis showed that at least 48% of the estimated number of persons living with HIV in Georgia remains undiagnosed, 16 who most likely contribute to the majority of new infections.17,18
High rates of late HIV diagnosis (45% of our study population already had AIDS at the time of HIV diagnosis) also provide evidence that a significant proportion of HIV-positive individuals remain undiagnosed for many years. The major reason behind this difference between the numbers of HIV-infected and diagnosed persons is the low testing coverage of key populations at risk4,19 and missed opportunities to diagnose in healthcare settings. 20 Reducing the number of undiagnosed cases of HIV infection will be critical to achieve the impact on the epidemic in terms of saving lives and preventing new transmission. Increased efforts are needed to expand HIV testing and counseling services as it serves as a gateway for linking vulnerable populations to prevention and care services.
Our findings reinforce the need for stopping the emerging epidemic among MSM. Similar to Georgia, expanding HIV epidemics has been described in other, traditionally viewed as IDU or heterosexual, epidemic settings of east Asia and Sub-Saharan Africa. 21 Nearly half of the persons infected through male-to-male sex in our study had recent HIV infection, and the proportion of MSM with recent infection increased from 36% in 2010 to 56% in 2012. BBS among MSM showed an alarming increase in HIV prevalence from 3.7% in 2007 to 13% in 2012.6,7 Unless urgently addressed this situation may result in an explosive outbreak of the epidemic. Along with scaling-up essential prevention packages for MSM, use of antiretrovirals for prevention needs to be considered in order to halt the spread of the virus in this population.
The HIV epidemic in Georgia is rapidly evolving. Similar to many Eastern European countries, in recent years Georgia has been observing transition from IDU-driven to heterosexual epidemic. 22 Although IDUs and heterosexually-infected persons were less likely to have recent HIV, in absolute numbers they accounted for the majority of recent infections, and remain at the core of the epidemic in the country. Available evidence indicates that in Georgia there exists an IDU epidemic-initiated heterosexual epidemic, which continues to be closely linked to IDU community.23,24 It is unclear whether there are linkages between MSM and IDU/Heterosexual epidemics. It should be mentioned that the HIV prevalence in pregnant women remains low (below 0.05%) indicating that the virus has not been spread in the general population. 15 Thus, the HIV epidemic in Georgia remains concentrated around key populations at risk. This provides the country with the opportunity to halt the spread of the virus through implementing targeted combination HIV prevention as a strategic mix of structural, behaviour and biomedical approaches that address both immediate risk and underlying causes of vulnerability. 25
Our study showed that younger persons were significantly more likely to have recent HIV, which was expected. However, data also provide evidence that transmission events occur in older populations as well. Regional differences should be also discussed. The proportion of recent infections was similar across all regions of the country except of Samegrelo. This region has the second largest number of reported cases and the fact that residents of Samegrelo were least likely to have recent HIV most likely indicates even greater caveats in testing coverage.
Findings of our study should be interpreted with caution as our study had strengths and limitations. The well-established HIV case-based surveillance, which collects data not only from the health system but from civil society, provided strength to the study. The system captures data on every reported case and biological specimens are also readily available. Use of clinical and laboratory data allowed us to minimize bias associated with false-recent cases.
On the other hand, there are caveats associated with surveillance-based estimation. The major limitation is that identification of new infections within the surveillance system depends on HIV testing patterns and thus may miss populations not accessing HIV testing and counseling services. Indeed, according to the data from the National Center for Disease Control and Public Health, more than 70% of persons tested annually represent low-risk populations such as pregnant women and blood donors. This issue is of particular concern in the major risk group of IDUs, who report extremely low HIV testing uptake. 4
FRR obtained in our study was very high, resulting in greater uncertainty around incidence estimates. The high FRR value was due to a high proportion of patients with AIDS or low CD4 cell counts in the sample. Despite the statistical power considerations, FRR was measured in a sample of individuals representative of the study population and therefore produced plausible estimates.
Despite these limitations, the study provides important information on the dynamics of the epidemic. Implementation of RITA as part of routine surveillance is feasible and a new generation of assays and approaches holds the promise to substantially improve the accuracy.26–28 Information generated from such surveillance, meaningfully triangulated with reliable and systematically collected second generation surveillance data, will help to better understand trajectories of the HIV epidemic in the country and thus will help to guide the effective and efficient response towards an AIDS-free generation.
In summary, despite the relatively stable HIV incidence over 2010–2012, the epidemic continues to grow because of the increasing gap between HIV infected and diagnosed persons. HIV is rapidly emerging in MSM, while IDU and connected heterosexual epidemic accounted for the majority of new infection. Scaling-up prevention interventions among key populations at risk and reducing the number of people with undiagnosed HIV will be critical for controlling the HIV epidemic in Georgia.
Footnotes
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This work was supported by UNAIDS Regional Support Team, Europe and Central Asia [project number 010/02/2012] and WHO Regional Office for Europe [project number 2012-256801].