
Abstract
Bichat Hospital's free and anonymous Voluntary Counseling and Testing centre in Paris is widely visited, with a high rate of HIV-positive diagnosis. This study proposed, in this centre, to describe the HIV newly-diagnosed patients over an 8-year period and to determinate risk factors for failure to return for a positive result. Higher risk for failure to return was found among the heterosexual subjects regardless of their socio-economic background.
Keywords
Introduction
Approximately 6000 HIV tests are performed each year at Bichat Hospital's Voluntary Counseling and Testing centre (VCT). The average rate of HIV-positive tests is 1.5% versus 0.66% tests in the overall Paris area. 1 This centre stands out for the high rate of positive tests and the high proportion of immigrants among the consulting population. The Sub-Saharan Africans and South Americans represented respectively 14% and 3% of the tested population, respectively (Bichat VCTs’ activity report, unpublished data). In the era of “Treatment as Prevention,” 2 it is important to design and implement different HIV testing strategies to improve linkage to care. 3 Identifying and targeting persons with risk of failing to return (FTR) may improve their return rate to the VCT. The objective of this study was to assess the proportion of FTR for an HIV-positive test result among those who tested positive and to identify risk factors associated with FTR.
Methods
We retrospectively analysed all HIV-positive patients diagnosed from 01 January 2004 to 31 December 2011 in Bichat’s VCT. Data were collected by reviewing patients’ files using a standardised questionnaire. The following variables were collected: year of consultation, gender, type of sexual contact (men who have sex with men [MSM]/heterosexual), exposure risk factors (sexual/other [IDU, unknown]), income (regular/non-regular), health insurance coverage (yes/no), residence status (fixed housing/homeless) and place of birth (France/Sub-Saharan Africa/South America/other). FTR was defined by an HIV-positive test in a patient who did not attend for follow up for ≥1 year. Patients who disclosed at the post-test visit of already knowing their positive status were classified as “hidden status.” They were not included in the analyses, as they probably represent a specific population. To compare characteristics between FTR and non-FTR among newly diagnosed HIV-positive patients, non-parametric tests were used for univariate analyses (Wilcoxon and Fisher exact tests). Variables achieving a p-value <0.20 in the univariate analysis were entered into a multivariate logistic regression model. A backward selection method was used to obtain a model in which all risk factors had a p-value <0.05. Statistical analyses were performed with SAS v9.3 (SAS Institute, Cary, NC).
Results
Univariate and multivariate analysis of failure to return for a HIV-positive test.
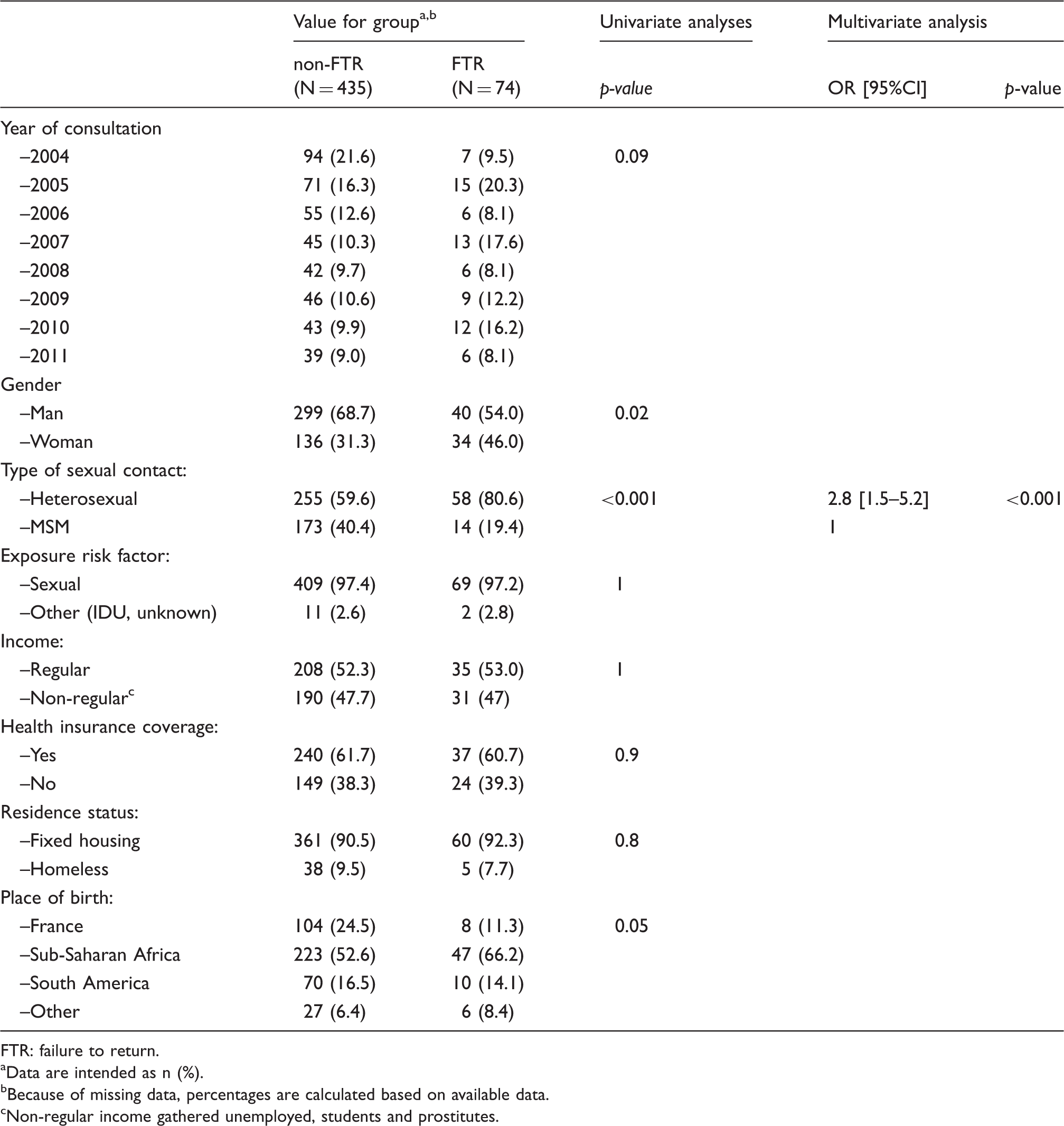
FTR: failure to return.
Data are intended as n (%).
Because of missing data, percentages are calculated based on available data.
Non-regular income gathered unemployed, students and prostitutes.
Discussion
HIV testing and counseling has been established worldwide as an important HIV prevention strategy.3–6 In France, publicly-funded free and anonymous VCT centres have high proportions of HIV-positive test results and are successful in targeting younger and high-risk populations.1,7,8 Our study is in accordance with these data. However, few French studies have reported FTR, a key variable along with testing and linkage to care in the current discussions regarding “test and treat” strategies.5,9 We estimated that 14.5% of HIV-positive patients FTR to the post-test counseling visit. This is in agreement with a study conducted in public-funded sites throughout California, where FTR occurred in 16.4%. 10 Two other studies performed in the US between 1995 and 2000 reported higher rates of FTR (48% and 58%).11,12 Moreover, in a study performed between 1997 and 2004 among clients of a mobile van testing in Los Angeles, a worsening trend was found in the proportion of FTR over time. 13 We found that heterosexuals were less likely to come back for their results; gender (women) was also associated with the outcome but only in the univariate analysis. In a study documenting the self-reported FTR for HIV in 7 states in the US in 2000, 20% of heterosexuals vs. 10% of MSMs reported FTR at least once. 14 In our study, heterosexuals were mostly immigrants from Sub-Saharan Africa. This population may be more concerned by HIV test results, than for example MSM, because of stigmas associated with an HIV diagnosis. 15 It has been shown that people with higher perceived risk of HIV infection are more likely to FTR for their result.12,14,16 We also found that socio-economic background and lack of medical insurance are not associated with FTR. This differs from studies performed mostly in the USA, where low educational level and unemployment increase FTR risk.11,14,16 Compared to the USA, 17 French public health policy provides full coverage of HIV-related care expenses and allows the delivery of a residency permit and financial help when required.
This study has limitations. First, data were only available for individuals who tested HIV-positive. It is not clear whether risk factors for FTR in HIV-positive patients are the same as in HIV-negative ones. Second, the study results obtained in a specific VCT in Northern Paris may not be extrapolable to other VCTs.
In conclusion, this study confirms that rates of FTR for a HIV-positive test results in a VCT are not negligible. To improve return rates, HIV pre-test counseling might be emphasised11,12,18 as well as the use of rapid HIV tests with results available during the same visit,12,14–16 putting aside other sexually transmitted infections testing. 19 Based on our results these tests should in particular target heterosexuals, who are at higher risk not to return for test results (vs. MSM).
Footnotes
Authors' contributions
All authors have made a substantial contribution to the concept and design, acquisition of data or analysis and interpretation of data, drafted the article or revised it critically for important intellectual content and approved the version to be published, the final manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.