
Abstract
Several effective interventions are available for preventing HIV in women. Targeting interventions requires understanding their risk of acquiring HIV. We used surveillance data to estimate risks of HIV acquisition for 13–59-year-old women following a diagnosis of syphilis, gonorrhoea or chlamydia in Florida during 2000–2009. We excluded women reported with HIV before their STI, and measured HIV reported subsequent to STI (through 2011). Rates were compared to women with no reported STI. A total of 328,456 women had: syphilis (3325), gonorrhoea (67,784) or chlamydia (257,347). During 2,221,944 person-years of follow-up, 2118 of them were diagnosed with HIV. For women with no STI reported, during 64,763,832 person-years, 19,531 were reported with HIV. The crude rate of subsequent HIV diagnosis (per 100,000 person-years) was higher for women diagnosed with syphilis (597.9), gonorrhoea (171.3) or chlamydia (66.3) than women with no STI (30.2). Annual rates of HIV decreased over-all by 61.8% between 2001 and 2011. Women with syphilis or gonorrhoea were at highest risk for HIV and therefore might benefit from intensive counselling. However, they represented only a small fraction of the women who acquired HIV. Most cases of HIV infection among women occurred among the large group of women who were not at highest risk.
Keywords
Introduction
Several interventions are now available that have evidence of effectiveness for preventing HIV infection, 1 including counselling, 2 HIV testing, 3 condom use, 4 treatment of infected persons, 5 post-exposure prophylaxis 6 and pre-exposure prophylaxis.7,8 Appropriate targeting of these interventions requires understanding of a woman’s risk of acquiring HIV infection. 9
In the United States, the rate of new HIV diagnosis for all women was 8.0 per 100,000 in 2010. 10 Prospective studies of women in some African countries have documented HIV incidence rates as high as 2000–4000 per 100,000 person-years (relative risk = 500 compared to all US women).1,7,8 Women considered ‘at-risk’ in the United States will likely have a risk that lies between these two extremes, but there are not many studies that provide good estimates. Studies that estimate risks for women have usually been cross-sectional or case–control studies; they estimate the risk of having HIV infection.11–18 There are not many studies in the United States that have followed HIV-negative women to see how many acquire HIV, and studies that are done often show rates that are lower than expected.13,19 In one study of 2099 high-risk women, recent infections detected at baseline suggested an annual incidence of 2520 per 100,000 person-years, but when the uninfected women were followed for a year only four acquired HIV, an incidence of 240 per 100,000 person-years.20,21 Persons who acquire other sexually transmitted infections (STIs) have a high relative risk for acquiring HIV, suggesting they should be a priority for interventions,11,15,17,19 but their absolute level of risk is less clear.
Infection with HIV is an important health problem in Florida, where HIV was the second leading cause of death for 25–44 year-old black women in 2010 (23.2 per 100,000). 22 Since 1998, the Florida Department of Health has routinely matched STI and HIV surveillance databases (using an algorithm based on name, age, race and date of birth) and added HIV diagnoses (for persons who have had syphilis, gonorrhoea or chlamydia) to the STI dataset. We used that database to determine the risk of being diagnosed with HIV infection following diagnosis of an STI, as an estimate of the risk of acquiring HIV.
Methods
We analysed all records of 13–59-year-old women in Florida who had reportable STIs (syphilis, gonorrhoea or chlamydia) that were reported between 1 January 2000 and 31 December 2009. We excluded late latent syphilis diagnoses if non-treponemal antibody was undetectable at dilutions of ≥ 1:32 because they were likely to be old infections. We then took the first diagnosis of syphilis, gonorrhoea or chlamydia that was recorded after 1 January 2000 for each woman. Women with more than one infection when the first diagnosis was made were categorised according to the first infection on this hierarchy: (1) syphilis; (2) gonorrhoea; and (3) chlamydia. We then excluded women who were reported as having HIV at or before the time of their first STI diagnosis (and within 60 days afterwards because they were likely already infected at baseline), and searched the database to see if the remaining women had subsequently been newly reported as having HIV infection. Follow-up for HIV began 60 days after the STI diagnosis and included all HIV infections diagnosed before 31 December 2011 that were reported by 19 March 2012. Person-years-at-risk for HIV began 60 days after the date of diagnosis for the STI and ended on the date the HIV infection was diagnosed, or on 31 December 2011 if no HIV was reported.
For comparison, we calculated the rate of HIV infection diagnosed among women with no reported preceding STI. This group includes women with HIV diagnoses before (or within 60 days after) their first STI diagnosis. To calculate the numerator, we took the number of HIV diagnoses for 13–59-year-old women in the Florida HIV/AIDS Surveillance database for 2000–2011, and subtracted the number of HIV diagnoses reported for women following an STI (measured above). The person-years-at-risk for this group includes risk time contributed by women before (and 60 days after) they were reported as having an STI. It was estimated by: (1) taking the number of 13–59-year-old women living in Florida in 2005, (5,582,148 according to the census); (2) multiplying by 12 years (to account for 2000–2011); and (3) subtracting the person-years-at-risk calculated for the women who had an STI (above).
Estimates were compared for various subgroups by STI, race/ethnicity, age, location and year of first STI. Multiple risk factors were combined to identify smaller subgroups at high risk. Age is not entirely comparable between groups because age was recorded at the time of STI diagnosis for women with an STI, and at the time of HIV diagnosis for other women. Location was classified as the residence at the time of the STI diagnosis even if the HIV infection was later reported from another location in Florida. ‘High-risk’ areas were defined as ZIP codes where at least 100 women aged 13–59 were reported with newly diagnosed HIV infection between 2000 and 2011, and there was an average annual rate of at least 65 HIV diagnoses per 100,000 women. Population estimates by combined age/race/ZIP code were only available for 2000 and 2010, so person-years-at-risk were calculated by assuming that the age/race proportions of women living in high-risk areas were the same in 2005 as they were in 2010.
Changes in HIV risk over time were assessed by plotting cumulative HIV diagnoses by time since the STI diagnosis for women grouped according to the year of their STI diagnosis (2000–2009).
To estimate risks by year of HIV diagnosis, we combined all women from the STI database and compared them to women with no STI reported. Risks for women with no STI reported were estimated by taking the yearly number of HIV diagnoses and census estimates for women living in Florida, and subtracting the corresponding women who have had STI.
We did not calculate confidence intervals for our estimates or p values for our comparisons because we included all surveillance data from Florida, not a sample. Our numbers are very large, and most of our errors would be expected to be due to variations in testing and reporting of STI or HIV and not due to chance. Centers for Disease Control and Prevention (CDC) staff did not have access to personal identifiers. Secondary analyses of routinely collected surveillance data do not involve human research and therefore do not require approval by the CDC Institutional Review Boards (IRB).
Results
Rate of HIV diagnosis for 13–59 year-old women in Florida 2000–2011, comparing women with and without a history of a preceding sexually transmitted infection in 2000–2009.
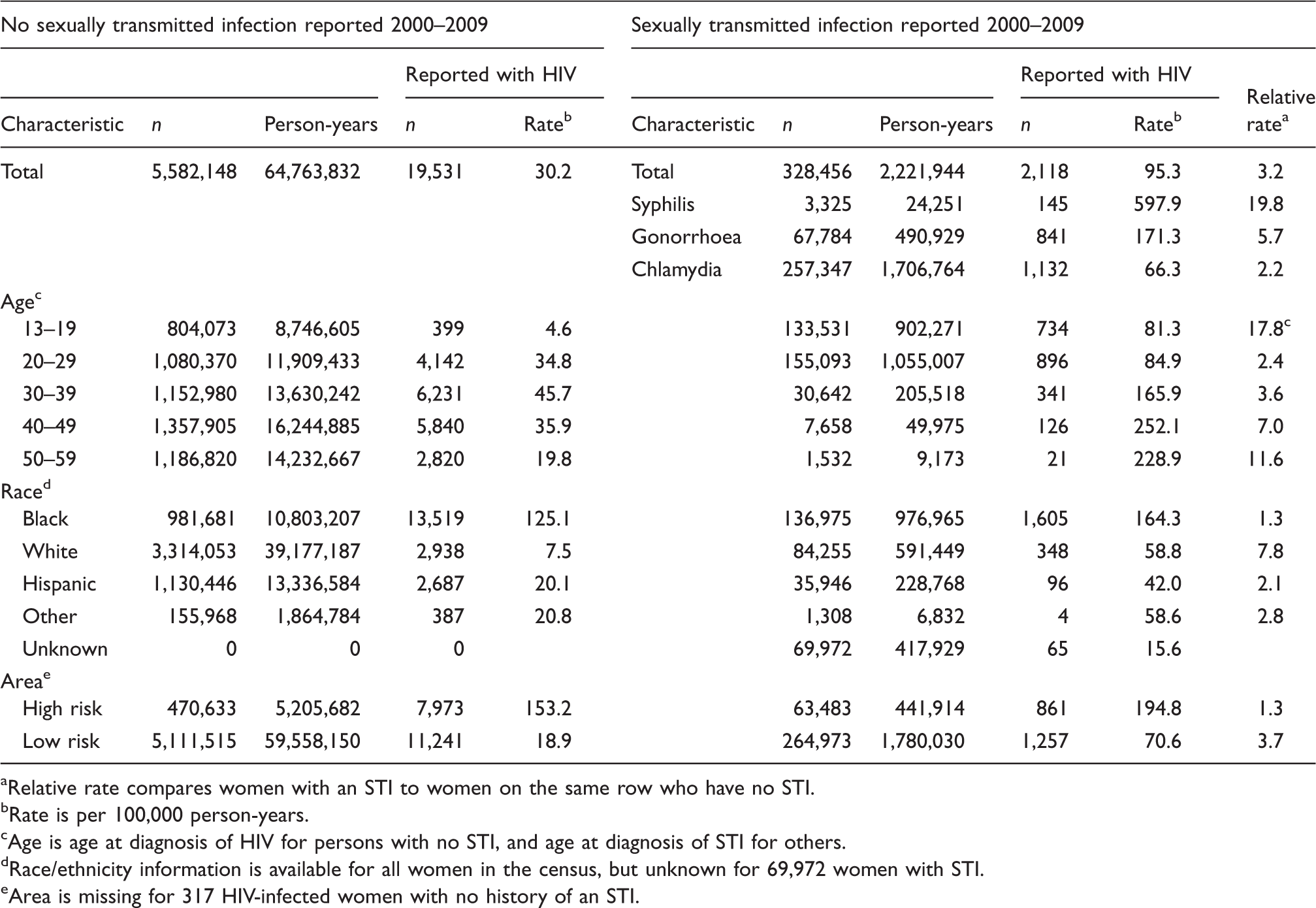
Relative rate compares women with an STI to women on the same row who have no STI.
Rate is per 100,000 person-years.
Age is age at diagnosis of HIV for persons with no STI, and age at diagnosis of STI for others.
Race/ethnicity information is available for all women in the census, but unknown for 69,972 women with STI.
Area is missing for 317 HIV-infected women with no history of an STI.
The 328,456 women with an STI had 2,221,944 person-years of follow-up in the database; 2118 were subsequently diagnosed as having HIV 61 days–11.6 years after the STI was diagnosed (mean follow-up 6.8 years, mean time to HIV 3.6 years). The 5,582,148 women (ages 13–59) in Florida with no STI reported in the interval had 64,763,832 person-years of follow-up; 19,531 were diagnosed as having HIV between 2000 and 2011. The rate of a subsequent diagnosis of HIV infection (per 100,000 person-years) was higher for women diagnosed with syphilis (597.9), gonorrhoea (171.3) or chlamydia (66.3) than women with no STI reported (30.2) (Table 1). The age group at highest risk of a reported STI was 13–19 year-olds (133,531 had STIs with a population size of 804,073 in 2005) whereas the group with the highest number of HIV diagnoses (6231) was 30–39-year-olds with no STI reported (45.7 per 100,000 person-years). Among all women diagnosed with one of these STIs, the rate of subsequent HIV diagnosis (per 100,000 person-years) was higher for blacks (164.3) than whites (58.8) or Hispanics (42.0). In contrast, the relative rate for HIV, comparing women with versus without an STI, was higher for white women (7.8) than for black women (1.3) or Hispanic women (2.1).
Rate of HIV diagnosis between 2000 and 2011 for select subgroups of black women in Florida.
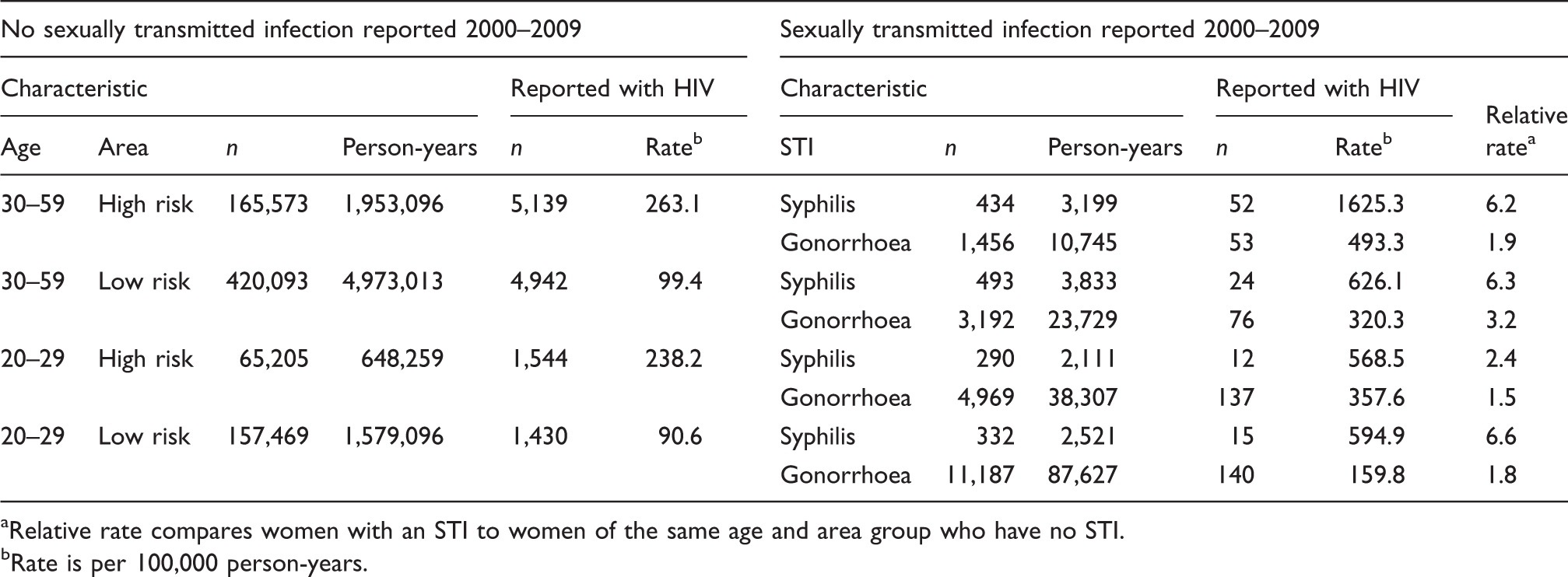
Relative rate compares women with an STI to women of the same age and area group who have no STI.
Rate is per 100,000 person-years.
The likelihood of being newly diagnosed with HIV was highest in the years immediately following the STI diagnosis, but even 11 years after their diagnosis, women who had an STI were diagnosed with HIV at a higher rate than women who had not had an STI (Figure 1). The risk of HIV for women diagnosed with an STI in 2000 was substantially higher than the risk for women first diagnosed in subsequent years. Six years after their STI, the cumulative number of HIV diagnoses was 1020 per 100,000 women who had an STI in 2000 compared to only 463 per 100,000 women diagnosed in 2005. Women in the 2005 cohort could not have an STI in the previous five years, or they would have been assigned to the cohort-year of their first STI. When we removed that restriction and allowed women to enter a cohort every year they had an STI, we still saw a decrease in risk over time, though the decrease in risk for years after 2000 was attenuated by an average of 16 per 100,000 per year of follow-up (data not shown). There were also changes in the initial STI diagnosed for women over the years in our STI cohorts. Comparing initial STI diagnoses in our dataset, in the years 2000 and 2009: syphilis decreased (629 to 327); gonorrhoea decreased (9154 to 5508); and chlamydia increased (22,506 to 32,675).
Cumulative number of HIV infections reported following the diagnosis of an STI, per 100,000 women, by year of STI diagnosis.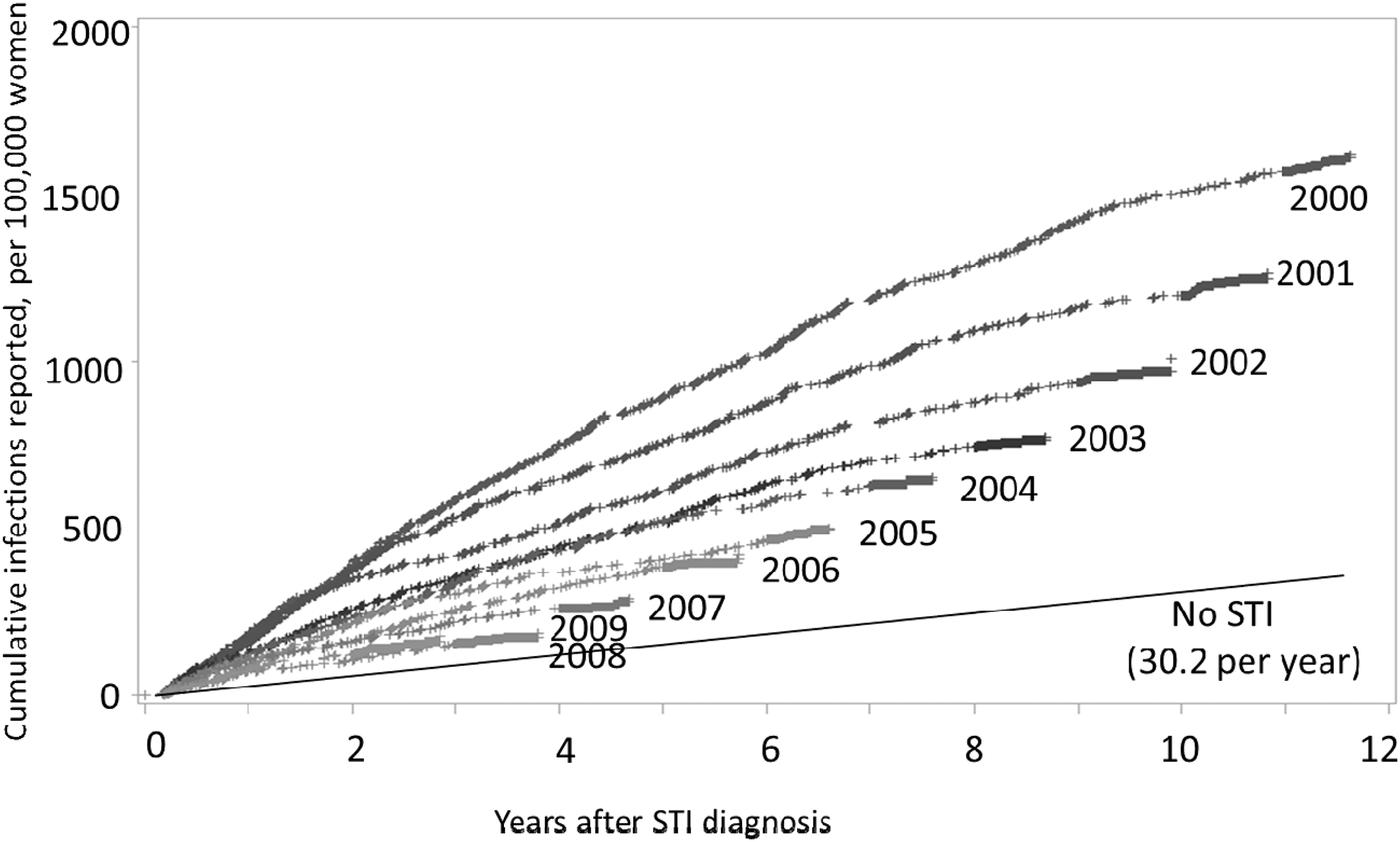
The annual risk of HIV for 13–59-year-old women in Florida who were not in the STI cohorts fell 61.8% (from 46.6 to 17.8 per 100,000 women) between the years 2001 and 2011 (Figure 2). The decrease in risk for women in the STI cohorts was larger (74.9%).
Annual HIV diagnosis rates for 13–59 year-old women in the STI cohorts and women not in the STI cohorts, Florida, 2001–2011 (log scale).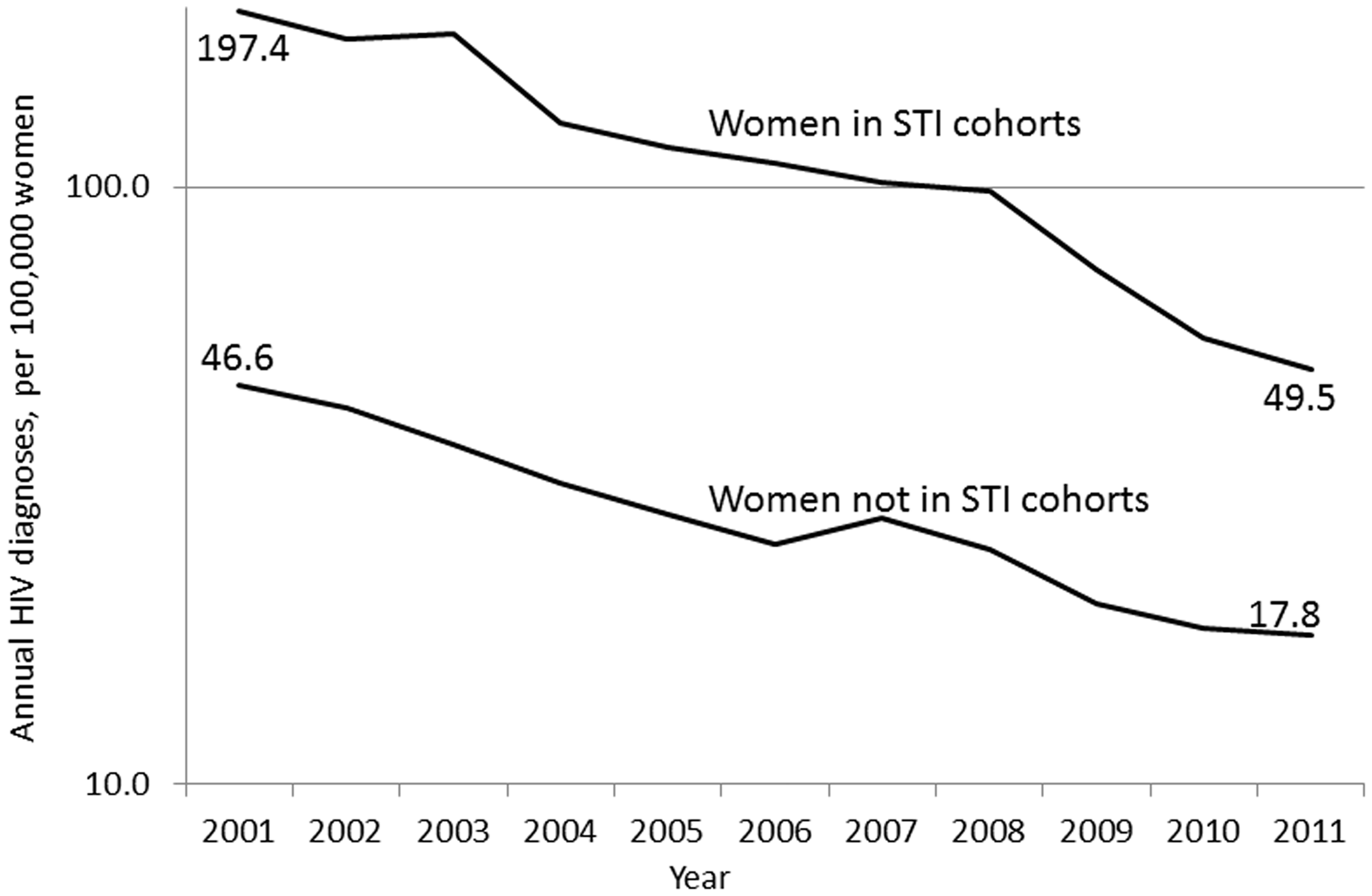
Discussion
The Florida surveillance database allowed us to retrospectively identify over 328,000 women who had an STI reported and calculate their risk of a subsequent diagnosis and report of HIV. After having an STI, the rate of being diagnosed with HIV infection was 95 per 100,000 person-years, 3.2 times the rate for other women in the same age range in Florida and 10 times the rate for women of all ages in the United States. Rates were high for older women, black women and women who were diagnosed as having syphilis or gonorrhoea. Black women aged 30–59 years who lived in high-risk areas and had syphilis were subsequently diagnosed as having HIV infection at a rate of 1625.3 per 100,000 person-years.
There have been several approaches to estimating the rate of HIV infection for women. The incidence of HIV (per 100,000 person-years) has been estimated for 2006–2009 as 8.6–10.7 for all women (age ≥ 13 years) in the US and 39.7–50.8 for black women using HIV antibody titres to estimate which infections were recently acquired (the serologic testing algorithm for recent HIV seroconversion, STARHS). 23 These rates are almost identical to rates of reported new HIV infections in the CDC national surveillance system in those same years (9.7–10.9 for all women and 47.4–52.9 for black women). 10 The STARHS assay and newer approaches 24 have been used to estimate the number of infections detected in cross-sectional studies that were recently acquired. However, these estimates may be too high if persons seek HIV testing due to recent high-risk behaviour. 25 A few studies have followed cohorts of women in the United States to measure their rate of acquiring HIV, and each identified only a few new infections. One found four seroconversions among 449 women in Brooklyn, NY for an incidence rate of 621 per 100,000 person-years. 13 Another found four seroconversions among 2099 high-risk women recruited at several venues around the United States for a rate of 240 per 100,000 person-years.20,21 Several of the subgroups of women with STI that we studied had rates of new diagnosis in this range.
The rates of HIV diagnosis seen in our cohorts have decreased since 2000. One reason for this decrease is that persons who entered the first cohort (2000) could have multiple STI in previous years, whereas persons who entered in subsequent years could not have a previous STI (since 2000), or they would have been represented in an earlier cohort. This illustrates how the potential impact of a prevention programme will decrease if persons at the highest risk are recruited early, and persons at lower risk are recruited later. Florida also had an increase in diagnoses of chlamydia over time, so later cohorts included more young women who are at lower risk of HIV than older women. However, most of the decrease in risk for the STI cohorts appears to be related to the 61.8% decrease in risk of HIV for other 13–59-year-old women in Florida since 2000. This decrease is greater than that reported by most other states with stable HIV reporting and warrants further investigation to identify possible causes. 23
The high level of risk seen in women with STI certainly merits counselling so that the women are aware of their risk and can take steps to reduce it. High-intensity counselling has been recommended for persons at risk by the US Preventive Services Task Force (at the ‘B’ level) 26 and would therefore be covered by certain insurance plans under the Affordable Care Act.27,28 Women who are diagnosed with an STI should be advised to use condoms consistently and correctly. The high risks we found suggest some of the women might be in a relationship with an HIV-infected partner. Therefore, women with STIs should assure that when their partners are treated for the STI, they are also tested for HIV and, if they are HIV infected, they stay on therapy. The high risk for women in certain ZIP code areas is consistent with other studies,15,17,29,30 and suggests that community-level interventions could and should be evaluated.9,29 However, community intervention trials would require identification of interventions expected to have a substantial impact that could be measured at the community level.
Electronic databases have the potential to track diseases in ways not possible with paper forms. Paper forms must be searched by hand, so surveillance in the past was typically reported as numbers of cases in a population. Electronic records are easily searched and, if the data are valid and complete, can add a new dimension to surveillance – patterns of infections within individuals over time. Others have merged disparate databases to identify intersection of populations at risk, but that approach is limited by the ability to match records. 31 Florida, like most large jurisdictions, maintains separate HIV and STI surveillance systems. However, Florida routinely matches databases so that HIV diagnoses are added to the records of persons who have had an STI. That matched STI–HIV database used in this analysis appears to be quite accurate, perhaps because it has been used as a single database by the sexually transmitted diseases programme, and the primary users depend on the accuracy of the data. In the future, other programmes may have the capacity to do similar analyses that expand the use of surveillance data for different infections. Timely access to surveillance analyses at the local level will increase opportunities to target prevention interventions.
Our findings have limitations. We did not actively follow women who were all tested and found to be HIV-uninfected. We measured the risk of being reported as having HIV in Florida, not true HIV incidence. We do not know the date that HIV infection was acquired, or how many infections were undiagnosed. Our estimates would overestimate incidence if HIV-infected women were not tested for HIV at the time of their STI diagnosis. Our estimates would underestimate incidence if women later acquired HIV but were not detected by our database because they were not tested, or because they moved away from Florida and HIV infection was diagnosed elsewhere. We cannot be sure that the women who were diagnosed with HIV after their STI actually acquired HIV after their STI, but the sustained high rate of diagnosis for several years suggests that the women were at sustained high risk for acquiring HIV. We have slightly over-estimated risk for HIV by race/ethnicity for women with STI because race/ethnicity information was missing for 21% of women with STI (the denominator), but was less likely to be missing for those women who later acquired HIV (the numerator). Finally, the goal of our study was to identify women at risk for acquiring HIV, not to measure the impact of STIs on HIV transmission. Therefore, women who had HIV diagnosed at the same time as their STI were not included. Similarly, women who developed an STI elsewhere would not be considered STI-associated if they were reported with HIV in Florida.
Women who are diagnosed with syphilis or gonorrhoea can benefit from being counselled about their risk for HIV and the many approaches to reducing it. The women at highest risk should be considered for additional interventions; however, they represent only a small fraction of the women who will acquire HIV. Most HIV infections among women are occurring among the large group of women who are not at highest risk. Targeting them individually will be difficult.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.