
Abstract
Summary
HIV-syphilis co-infection is often cited as a major reason behind recent resurgence in syphilis prevalence among men who have sex with men in China. Most published literatures explore factors associated with either HIV or syphilis, but not their co-infection. We analysed data from a cross-sectional survey on men who have sex with men in seven Chinese cities. Snowball sampling was used to recruit participants for the survey. Socio-demographic and behavioural predictors for HIV-syphilis mono/co-infection were examined using ordinal logistic regression. Factor scores were used to summarise (1) HIV-related knowledge and (2) access to HIV preventive services. Prevalence of HIV, syphilis, and their co-infection, among 2936 self-identified men who have sex with men, were 7.7%, 14.3%, and 2.6%, respectively. In the adjusted analysis, the significant positive correlates of poorer diagnoses (co-infection vs mono- and no infection or co- and mono-infection vs no infection) were: 30 to 39 years and ≥40 years age, education up to senior high school, unprotected anal intercourse, recent sexually transmitted infection symptoms, incorrect knowledge about routes of transmission, and access to preventive or counselling/testing services for HIV. For effective control of this dual epidemic, integrated HIV and syphilis surveillance and targeted intervention strategies for Chinese men who have sex with men are needed urgently.
Introduction
As has been widely reported, men who have sex with men (MSM) in China have been witnessing a rising epidemic of HIV and syphilis infection.1–3 While the overall prevalence of HIV in the Chinese population stands at a modest 0.05–0.06%, 4 the reported prevalence among MSM ranges from an estimated 3.5% (north-west and south-central China) to 13.2% (south-west China) and has been showing an increasing trend.2,3,5 Additionally, syphilis infection has also been rising over the past two decades, after being close to eradication in 1960s.1,6 Co-infection of syphilis with HIV among MSM is expected to have played an important role in this resurgence. 1 The positive association observed between syphilis and HIV among MSM can be explained by biological plausibility and similar risk behaviours associated with both infections.7,8 Most studies report the determinants of either HIV or syphilis in a selected sample population from specific urban cities in China at a specific time, but very few studies have reported on co-infection. 1
In the literature, a wide array of demographic, behavioural and societal factors, have been identified that predict acquisition of syphilis or HIV among MSM in China. These factors include but are not limited to old age, poor education, multiple sex partners, engaging in commercial sex, unprotected anal intercourse (UAI), being infected with other sexually transmitted infections (STIs).9,10 Although most of the published literatures accept the role of knowledge about infection, many of them either fail to adjust for them or use some surrogate measures, while estimating associations between disease and the predictors.2,9,10 Behavioural interventions have been an integral part of the measures adopted by China in the past decade to halt the HIV epidemic.11,12 These interventions have been supported by efforts to improve knowledge about HIV and other STIs and scaling up of HIV-related services. 13 Thus, knowledge about HIV and uptake of HIV preventive services should be taken into account while estimating predictors of not only HIV but also syphilis, as these infections share many predictors. 1
Quite a few studies have reported the risk factors of HIV and syphilis infection among MSM in various cities of China.14–18 The findings from these studies often vary widely, which may suggest differences in geographic, socio-economic, and risk behavioural factor distribution between different cities. Among these studies, however, few report co-infections of HIV and syphilis, and even fewer explore the factors associated with co-infections. We analysed survey data from seven Chinese cities to determine the factors associated with co-infection of HIV and syphilis among MSM.
Methods
Study sample
This analysis used cross-sectional survey data from seven Chinese cities, namely Nanjing, Chongqing, Jinan, Haerbin, Guangzhou, Suzhou, and Yangzhou. The data were collected in 2008 as part of a nation-wide survey 3 on MSM, conducted by Chinese Center for Disease Control and Prevention (CDC). The initial plan was to employ “Respondent-driven sampling (RDS)” 19 in five cities (Nanjing, Chongqing, Jinan, Haerbin, and Guangzhou), and “Snowball sampling” 20 in the other two cities for participant recruitment. However, owing to operational difficulties, “Snowball sampling” was used in all seven cities. Briefly, a set of initial participants (seeds) were enlisted, in consultation with non-governmental organisations, who were then asked to recruit other MSM in their network(s) for behavioural evaluation and serological testing, using uniquely numbered coupons to allow tracking of the recruitment process. This process continued in an expanding format, with respondents obtained in one wave being asked to recruit others in the next wave, until desired sample size was reached.
To be eligible for the study, the participants needed to be men, at least 18 years old, having had oral and/or anal sex with men during the past 12 months, and willing to provide consent for HIV and syphilis testing. The data collection procedure was anonymous and names (or other identifying information) of the participants were not recorded. Blood specimens collected (following counselling and consent) from participants were tested immediately for HIV and active syphilis using rapid testing kits and waiting participants were informed about test results. In case a participant had inconclusive test result(s), he was asked to return to obtain his result(s) from confirmatory tests. (See online supplementary information for details about diagnostic tests used). As a token of appreciation for their participation, respondents were provided a package containing lubricant and condoms (worth ∼US$ 5). Further, a sum of approximately US$ 1.6 (per new recruit) was paid to participants who successfully recruited other MSM from their social networks. Study procedures were carried on at local STI clinics run by provincial CDCs.
Measures
Demographic and socio-economic variables
Demographic and socio-economic measures included in the analysis were age, education level, monthly income, ethnicity, marital status, and city of residence. Education was measured by highest level of education obtained, categorised into less than junior high school, junior high school, senior high school, and junior college or higher. Since the Chinese population is predominantly Han, we used two categories for ethnicity, Han and others. City of survey was used as a surrogate for participant's city of residence.
Risk behavioural variables
The following risk behavioural characteristics were included in the analysis: venue of meeting partners, sexual orientation, age at first insertive intercourse, gender of first partner, condom use during last anal sex, number of different male partners in past six months, reported UAI in past six months, symptoms of STI in past year, paying for and/or selling anal sex to men in past six months. Sexual orientation was determined by what a respondent perceived himself to be, and not what his actual behaviour suggested. UAI was defined as never or only occasionally using a condom during anal intercourse in the past six months with all male partners. Number of different male partners was categorised into having five or fewer male partners in past six months and more than five different partners.
Factors representing knowledge and access to HIV-related services
In our analysis, we used two separate sets of factors, created using factor analysis, (1) to determine knowledge and attitude of participants regarding HIV and (2) to evaluate access to various services provided under HIV prevention programmes. There were eight possible responses, each coded as a discrete variable, determining a participant's knowledge about HIV. Access to HIV-related services were represented by six other variables (for the complete list of knowledge and access to care variables, see online supplementary information).
To reduce the problem of dimensionality caused by large number of variables representing knowledge and access to HIV-related services and to find specific constructs, we created factor scores from those variables. Factor analysis with principal component extraction and varimax rotation method was employed (factor loading ≥ 0.50) to extract knowledge and access to prevention factors. We used orthogonal (varimax) rotation because it could make interpretation simpler and also could maintain independence of the factors. 21 The results extracted from factor analysis represented two underlying factors (based on loading of specific items) for knowledge about HIV, namely “Correct/helpful knowledge about routes of transmission” and “Incorrect knowledge about routes of transmission.” In the domain of access to HIV services, the two extracted factors were interpreted as follows, “Receiving HIV/STI preventive services” and “Access to HIV/STI testing and counseling.” We based our selection of the number of factors on interpretability of factors, instead of selecting them mechanically on the basis of “Eigenvalues” or “Scree plots.” 22
Outcome measures
The outcome in our analysis comprised two components: testing positive for (1) syphilis and (2) HIV.
For assessment of determinants of syphilis and HIV co-infection, we created a combined outcome variable having three levels (for easier interpretation these categories were classified as good, poor, and poorest diagnoses):
i) Co-infection (positive for both HIV & syphilis) – poorest diagnoses ii) Mono-infection (either HIV or syphilis) – poor diagnoses iii) No infection (neither HIV nor syphilis) – good (baseline) diagnoses
Statistical analysis
Descriptive analysis of our data included determination of prevalences and distribution of socio-demographic and risk behavioural characteristics. There were 2958 observations in total. We deleted the observations which had missing values for any of the following variables: age, marital status, ethnicity, education level, income, venue for meeting partners, age at sexual debut, and size of MSM network. Following these deletions, we were left with 2936 observations. For some variables missing observations were generated by ‘skip-pattern’ in the questionnaire because of negative response to some prior questions (e.g. if the participant did not engage in certain activity, then he was not asked the following questions about that activity). To account for such automatically generated missing values, we created distinct missing value categories for sexual orientation, number of male partners in past six months, STI symptoms in past year, engaging in commercial sex in past six months, and UAI in past six months.
Bivariate associations of demographic and risk-behavioural characteristics were tested, using simple logistic regression, with syphilis and HIV-positive status. Frequencies (and proportions) in each category of different predictor variables were cross-tabulated with syphilis and HIV. Similarly, distribution of predictors and bivariate associations were also assessed with the combined outcome variable having the following categories: co-infection (HIV and syphilis), mono-infection (HIV or syphilis), and no infection.
We implemented multiple ordinal logistic regression to determine predictors of HIV-syphilis co-infection and find the adjusted associations. We reviewed published literature to select the following independent variables for our analysis: age, educational level, reported sexual orientation, venue for meeting partners, age at sexual debut, UAI in past six months, history of STI symptoms in past year, paying for sex with other men in past six months, number of male partners in past six months, as well as factors (from factor analysis) representing knowledge about HIV/STI and access to HIV-related services. The observed associations were further adjusted for ethnicity, marital status, monthly income, city of survey. The ordinal model was built on the assumption that the categories of combined outcome variable i.e. co-infection, mono-infection, and no infection followed a natural ordering (from good to poorest diagnoses) and fulfilled the proportional odds criteria. The score test (multivariate model) for proportional odds hypothesis yielded a p value of 0.55, suggesting that ordinal model was reasonable.
All analyses were carried out using SAS statistical software version 9.3.
Results
Socio-demographic and risk behaviour characteristics of participating MSM, China National MSM Survey (n = 2936), 2008.

Values and percentages may not sum to total or 100% due to missing and rounded numbers.
Among the included subjects, 441 reported not engaging in anal sex in past 6 months.
Western blot positive.
Simultaneously positive on both RPR and TPPA.
RIBA positive.
HCV, hepatitis C virus.
Distribution and bivariate associations with predictors (from ordinal logistic regression) of syphilis and HIV co-/ mono-/ no infection, China National MSM Survey (n = 2936), 2008.

Values and percentages may not sum to total or 100% due to missing and rounded numbers.
Factors created from factor analysis. Significant associations (p<0.05) in bold.
Predictors of syphilis and HIV co-infection (compared to mono and no infection) from ordinal logistic regression, among men who have sex with men, China National MSM Survey (n = 2936), 2008.
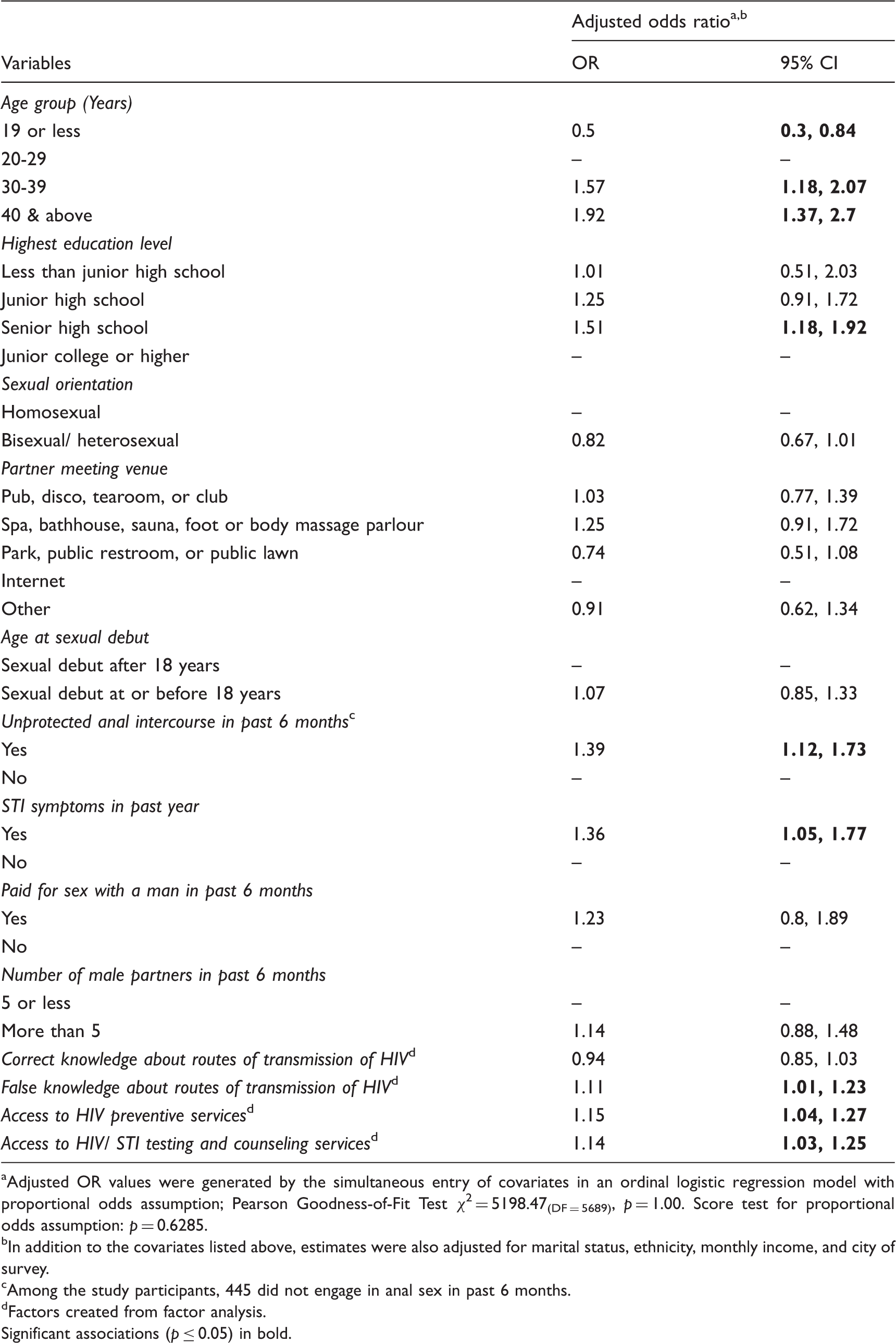
Adjusted OR values were generated by the simultaneous entry of covariates in an ordinal logistic regression model with proportional odds assumption; Pearson Goodness-of-Fit Test χ2 = 5198.47(DF = 5689), p = 1.00. Score test for proportional odds assumption: p = 0.6285.
In addition to the covariates listed above, estimates were also adjusted for marital status, ethnicity, monthly income, and city of survey.
Among the study participants, 445 did not engage in anal sex in past 6 months.
Factors created from factor analysis.
Significant associations (p ≤ 0.05) in bold.
Discussion
This study of MSM provides information on prevalences of HIV, syphilis, and their co-infection in seven Chinese cities, along with demographic and behavioural factors associated with co-infection of these two STIs.
The overall prevalence of HIV, syphilis, and co-infection among MSM in the seven studied cities were 7.7%, 14.3%, and 2.6%, respectively. Prevalences of HIV and syphilis were higher than the nationwide (61 cities) prevalence obtained from China National MSM survey (4.9% and 11.8%). 3 Co-infection prevalence was commensurate with the findings of a meta-analysis based on 13 eligible studies (2.7%), 1 however, it was higher than the cumulative prevalence in the MSM survey (1.5%). 3
As per the biological plausibility, UAI and recent STI symptoms were found to be potential risk factors for co-infection, corroborating previous reports from China. 23 We did not detect a significant association of co-infection with having higher number of male partners. Reverse causation can be a potential reason for this, as an MSM may reduce frequency of his sexual contact if he is having any STI symptoms, suffering from poorer health (owing to presence of simultaneous infections), and/or after being diagnosed with either infection.
Adjusting for other predictors, correct knowledge about routes of transmission of HIV was not a significant protective factor for co-infection. This finding can be due to the fact that the overall knowledge of the study participants were quite high (about 80% participants correctly answered six or more of the eight questions related to the knowledge about routes of transmission of HIV). Since the overall knowledge was high, discrimination of knowledge between HIV or syphilis sero-positive and sero-negative participants was probably low, leading to lack of power to detect a significant association. 24 Incorrect knowledge, as expected, was associated with increased odds of co-infection. However, contrary to expectation, access to HIV-preventive services and access to HIV/ STI testing and counseling services were positively associated with co-infection. Again, reverse causation can be a possible explanation for these findings, as participants having symptomatic STIs in a single cross-sectional time frame are likely to avail/access preventive and treatment services.
Being observational in nature, this study suffered from quite a few limitations. First, because of our cross-sectional design, lack of temporality prevents us from drawing any causal inferences. The time orders of predictors were often unclear – e.g. whether access to preventive services affected infection prevalence or the other way round. Secondly, the fact that most of our data were self-reported raises concern about social desirability bias that, in turn, may lead to severe exposure misclassification. Moreover, selection bias (which can arise from low response/participation rates) can also be a potential threat to validity. Response rates, measured by proportion of returned coupons out of total coupons distributed during recruitment of MSM, were quite low across all the study sites (for example, it was only 33.3% in Nanjing). 25
To minimise chances of variation in quality of collected data across the study sites, a uniform protocol was followed at every site, and all study personnel were trained together by the same programme. Further, HIV and syphilis results were declared to the participants only after completion of their interviews, reducing the probability of obtaining “expected” answers from participants who were aware about their disease status. Therefore, we expect any misclassification of exposure in this study, if present, to be non-differential. Still, we do not rule out possibility of differential misclassification, because some participants might have had symptomatic infection or were aware of their infection status before they participated in the study.
Despite the above limitations, our study had quite a few strengths. Use of snowball sampling gave us access to sufficient number and a relatively comprehensive pool of participants from this hard-to-reach population. We further enhanced our sample size by aggregating data from different cities, which allowed for simultaneous adjustment of multiple potential confounders. We used factor analysis to create scores for disease-related knowledge and access to preventive services, enabling us to summarise their effect on syphilis and HIV prevalence in an efficient way.
Our study findings reiterate the fact that Chinese MSM are at high risk of syphilis and HIV infection (and their co-infection) and there is an urgent need for intervention targeted towards this population. Literature review reveals that being infected with syphilis increases risk of acquiring HIV. Moreover, an active T. pallidum infection worsens the biological parameters associated with HIV – leading to lowering of treatment response and predisposing the infected towards AIDS.26,27 Concentrated epidemics of HIV and syphilis among this highly vulnerable group calls for a convergent surveillance strategy – as per recommendations of Karumudi et al. – anyone presenting with syphilis should be tested for HIV and vice versa. 28 Additionally, behavioural components, such as reduction in UAI, should constitute an integral part of the intervention measures. Spreading awareness about these STIs can be a crucial prevention tool as well. Finally, most studies on MSM have utilised data arising from cross-sectional surveys, thereby severely restricting the ability to make causal inference about different predictors of STIs. To overcome such limitation, a large-scale longitudinal study could be planned to further explore variables associated with HIV, syphilis, and other STIs among MSM.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant No. 81373125), Jiangsu Provincial Technologies Research Program (BE2009685), Jiangsu Province's Outstanding Medical Academic Leader Program (RC2011086, 2011087).