
Abstract
Summary
In Kenya, there was a reported decline in HIV incidence and prevalence among those aged 15 to 64 years and children. Despite the decline, closer assessment of psychosocial issues like depression, contextual factors (family and community), and social support is necessary given the likely impact on overall health and HIV prevention. This paper examines an association between symptoms of depression and social support on overall health among HIV-positive participants recruited from an HIV clinic in Kenya. Descriptive statistics and logistic regression analyses were utilized. Findings reveal that compared to those with minimal depression (referent category) participants with mild, moderate, moderately severe/severe depression had higher odds of having poor health. For social support, compared with participants with no social support (referent category), participants with high social support had lower odds of having poor overall health in both unadjusted and multivariable-adjusted models. In conclusion, this study suggests that HIV clinics and interventions need to focus more on the psychological and/or mental health status of HIV-infected individuals while providing avenues such as social support groups that can be a buffer against the negative impact of HIV infection and depression on overall health outcomes.
Introduction
Although HIV/AIDS is reported to disproportionately impact sub-Saharan Africa, the Joint United Nations Programme on HIV/AIDS (UNAIDS) recently reported a decline in HIV rates among adults and children since the year 2001. 1 Particularly, as of 2011 there was a 25% decline in HIV incidence rates, a 32% decline in HIV/AIDS-related mortality, and a 28% decline in tuberculosis-related mortality rates among people living with HIV/AIDS (PLWHA). 1 Such decline signifies tremendous effort in the fight against the spread of HIV infection in sub-Saharan Africa.
In Kenya, there was a reported 40% decline in new HIV infections in 2011, 2 1.6% decline in HIV prevalence (from 7.2% to 5.6%) among those aged 15 to 64 years, and a 0.9% decline in children 18 months to 14 years old in 2012. 3 While such declines were noted in most regions in Kenya, significant declines were reported in Nairobi, Coastal and the Rift Valley areas. 3 Again, such findings signify great strides in the fight against HIV/AIDS in this region. However, given that HIV prevalence rates have stabilized at high levels in Kenya, there is a need to further enhance prevention strategies in order to maintain the continued reduction in HIV transmission. Particularly, a closer assessment of underlying psychosocial issues like depression, HIV stigma, contextual factors (family and community), and social support, which may have a potential influence on HIV prevention, is necessary.
Relevant to depression, there is a reported correlation with HIV infection. A more concerning issue about such a relationship is that depression and HIV infection are projected to be a prominent driver of disability in the near future. 4 In a study examining depressive symptoms and psychosocial aspects of PLWHA receiving HIV/AIDS care in Kenya, Namibia, and Tanzania, findings indicated a little over 25% of the study participants reported mild to severe depressive symptoms and therefore needed psychological care. 5 Additionally, participants with high scores on depression measures are reported to have low quality of life, which may increase disease progression, impact overall health, 6 and increase psychiatric-related morbidity,7,8 engage in maladaptive sexual behaviours, 4 engage in alcohol use, and not adhere to prescribed anti-retroviral medication. 9
Depression in PLWHA is deemed an impediment to HIV prevention strategies such as medication adherence, condom use, and disclosure of serostatus. Particularly, concerns about disclosure of HIV status could lead to depression, stress, and early morbidity. 10 Hence, a lack of social support after testing HIV positive is likely to increase the likelihood of depressive symptoms in PLWHA in urban cities, while in rural areas cultural practices such as polygamy increase depression because women are not in favour of sharing a partner.10,11
To help alleviate depression symptoms, social support from friends, family, and community organizations and knowledge of other people who also have HIV is considered a buffer.4,12 Social support is reported to enhance aforementioned HIV infection prevention strategies and reduce related stigma.5,13 In a study examining factors leading to unsafe sexual behaviours and changes in sexual behaviours among PLWHA receiving antiretroviral medication for a period of 12 months, findings revealed that 32–35% of participants suffered from moderate to mild depression. These participants were deemed to be at an increased risk of engaging in unsafe sex. 14 To that end, research supports that social support is critical in helping to minimize psychological distress, isolation, and enhance success of aforementioned HIV-prevention strategies.5,12–16
Such findings are critical to HIV prevention programmes in Kenya given that HIV prevalence rates have stabilized at high levels. There is documented need to monitor and address depression feelings in PLWHA to prevent HIV transmission among participants who are concerned with disclosing their status to their sexual partners, which determines the likelihood of practicing safe sexual relations. More investigation of a likely relationship is important and should be incorporated in the treatment plan of PLWHA. 17 Given the documented link between HIV infection, depression, social support, overall health outcomes of PLWHA and the limited research in Kenya examining that particular link, the purpose of this paper is to examine the impact of symptoms of depression and social support on the overall health of PLWHA in a resource-limited setting of a large urban city in Kenya. No other studies in Kenya have examined the aforementioned link in that target population and setting.
Methodology
Recruitment and data collection
This was a cross-sectional study approved by the African Medical Research Foundation (AMREF) Ethics and Scientific Review Committee Kenya (P22/11) and Indiana University-Bloomington's Institutional Review Board (1011004332). The study involved 370 HIV-positive participants recruited from and receiving HIV care at an HIV Voluntary Counseling and Testing clinic in a low-income urban setting in Kenya over a period of three and a half weeks in the year 2011.
Potential participants were recruited with the assistance of two designated medical officers (because principal investigator [PI] did not have access to medical records) in the privacy of the medical officer's office and asked if they were interested in voluntarily providing information about their HIV experiences including stigma. All measures were taken to be discreet to protect the privacy of each potential participant. Willing participants were then directed to a private room and screened for eligibility. Eligible participants had to have a diagnosis of HIV, receiving HIV-related care at the VCT clinic, and between 18 and 60 years old. Eligible and willing participants signed an informed consent form before completing an anonymous researcher-administered paper-based survey developed in English and Swahili (Kenya national languages spoken by the majority of the population).
Two HIV-positive assistants, a man and a woman, were recruited from a social support group to assist with administering the questionnaires. They received training on cultural sensitivity, reading questions to participants with low levels of educations and reporting any issues to the PI. Prior to assisting with the current study, both assistants had previously engaged in counseling activities among different PLWHA support groups. Informed consent forms were administered for signature by the PI to ensure that each participant understood the purpose of the study and voluntary nature of their participation.
More information on recruitment and validating the paper-based survey translation can be found in previously published papers.6,18
Measures
Dependent variable: Overall health
The general rating measure was adopted from the SF-12 19 instrument to measure overall health. The response levels (excellent = 5, very good = 4, good = 3, fair = 2, poor = 1) were collapsed into two binary categories: optimal = 5 through 3 and poor = 2 through 1.
Independent variables
Sources of supportive resources
Participants were asked to rate how supportive different groups of people (family, friends, co-workers, people at church) were of them on a scale of 1–5 (1 = “never”, 5 = “always”, and 6 = “question not applicable). Social support sum scores ranged from 0 to 44 and are based on participants' rating of the level of support they received from different individuals over the past three months regardless of their HIV status. Because “never” responses imply not receiving any support, the response levels were recoded into (0 = never, 1 = rarely, 2 = less often, 3 = often, 4 = always”). Individuals with “not applicable” responses were assigned value of 0 to indicate that they have not received any support. Cronbach's alpha of 0.71 supported the internal consistency reliability of the sources of supportive resources scale in this sample. The list of supportive resources include: spouse, children, immediate family members, friend, employer, elders, close relatives, people at church, grandparents, a neighbour, and others. After creating the sum of scores for each question, the new variable was transformed to a 0 to 100% scale by dividing the observed score by the maximum possible score and multiplying the result by 100%. These values were then recoded arbitrarily into three categories of supportive resources (none = 0%, medium = 1% through 25% and high = greater than 25%).
Depression
Depression symptoms were measured using the nine-item Patient Health Questionnaire (PHQ-9).20,21 Depression sum scores ranged from 0 to 27 across severity categories: minimal = 0 to 4, mild = 5 to 9, moderate = 10 to 14, moderately severe = 15 to 19, and severe = 20 to 27. These categories were then collapsed and recoded into four categories (minimal depression = 0 through 4, mild depression = 5 through 9, moderate depression = 10 through 14, and a combination of moderately severe and severe depression = 15 through 27). The last two categories were combined because of small sample sizes in each. Cronbach's alpha of 0.82 supported the internal consistency reliability of the PHQ-9 in this sample. This validated questionnaire has also been utilized among similar PLWHA populations globally.20–26
Other covariates
Characteristics of study sample (N = 312).
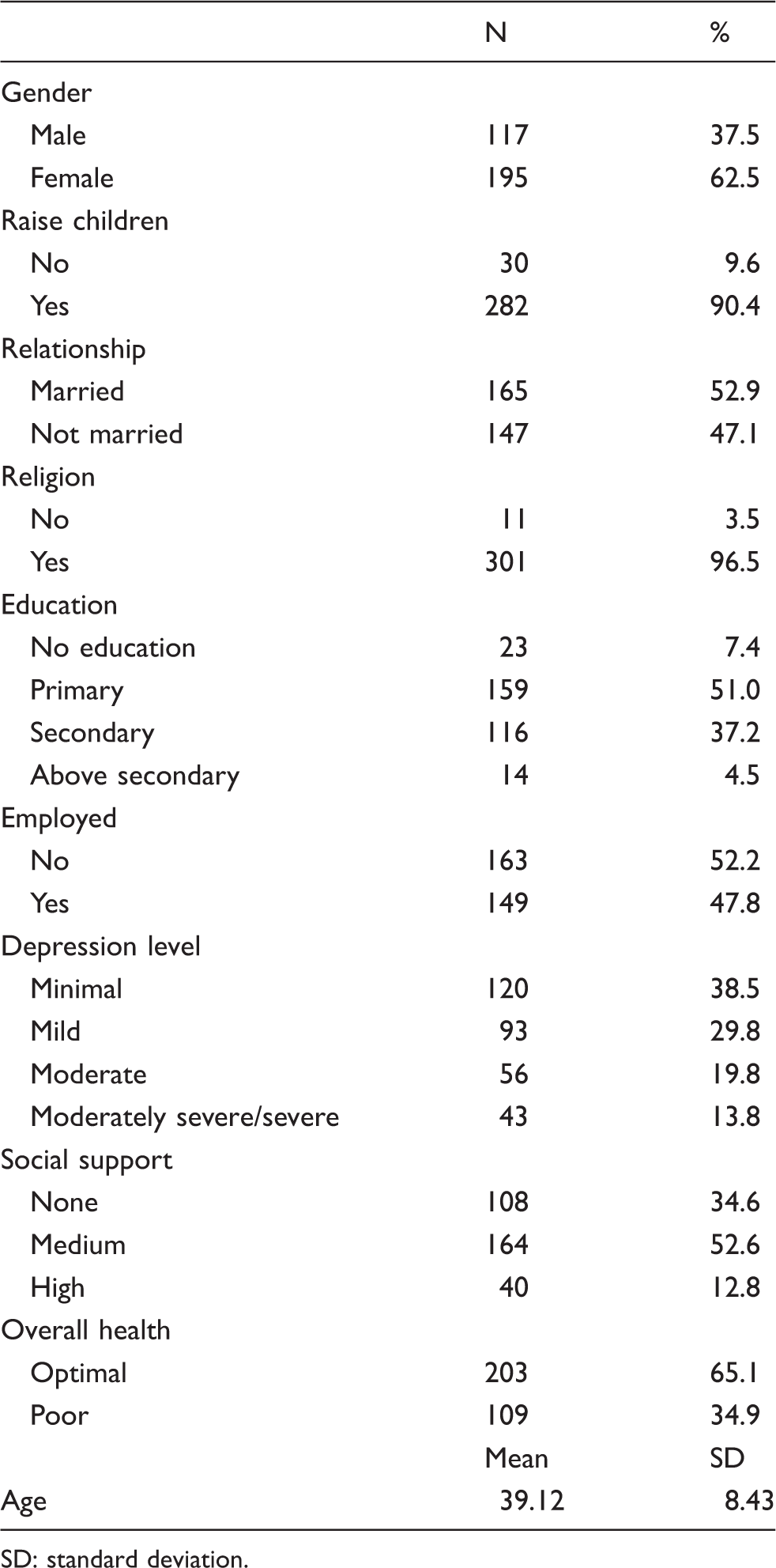
SD: standard deviation.
Statistical analysis
Descriptive statistics using mean and standard deviation for continuous variables and frequencies and percentages for categorical variables were computed. Depression and social support level by overall health status were determined utilizing Chi square test. The association of depression and social support and overall health were evaluated using two logistic regression models. We completed (1) crude or unadjusted logistic regression model; (2) multivariable model in which we adjusted for age, gender (female, male), raises children (no, yes), relationship (married, not married), associated with religion (no, yes), education (none, primary, secondary, above secondary), employed (no, yes). We performed tests for trend with social support as an ordinal variable in the unadjusted and multivariable models. To examine potential collinearity, regression diagnostics for collinearity were performed. There was no significant collinearity of variables included in the multivariable model. All analyses were conducted using SAS (version 9.3.; SAS Institute, Cary, NC) software.
Results
We excluded subjects with missing data on responses related to social support, depression, overall health and other covariates used in our multivariable models. The final sample for the analysis comprised 312 participants (62.5 % women), of which 109 (35%) had reported poor overall health.
Table 1 presents the descriptive characteristics of the study participants. There were more participants who: raised children, were married, were associated with religion, only had primary level education, were not employed, had medium depression, and had medium social support. Overall, the study sample population was middle-aged (mean age 39.12 years).
Depression and social support by overall health status (N = 312) .
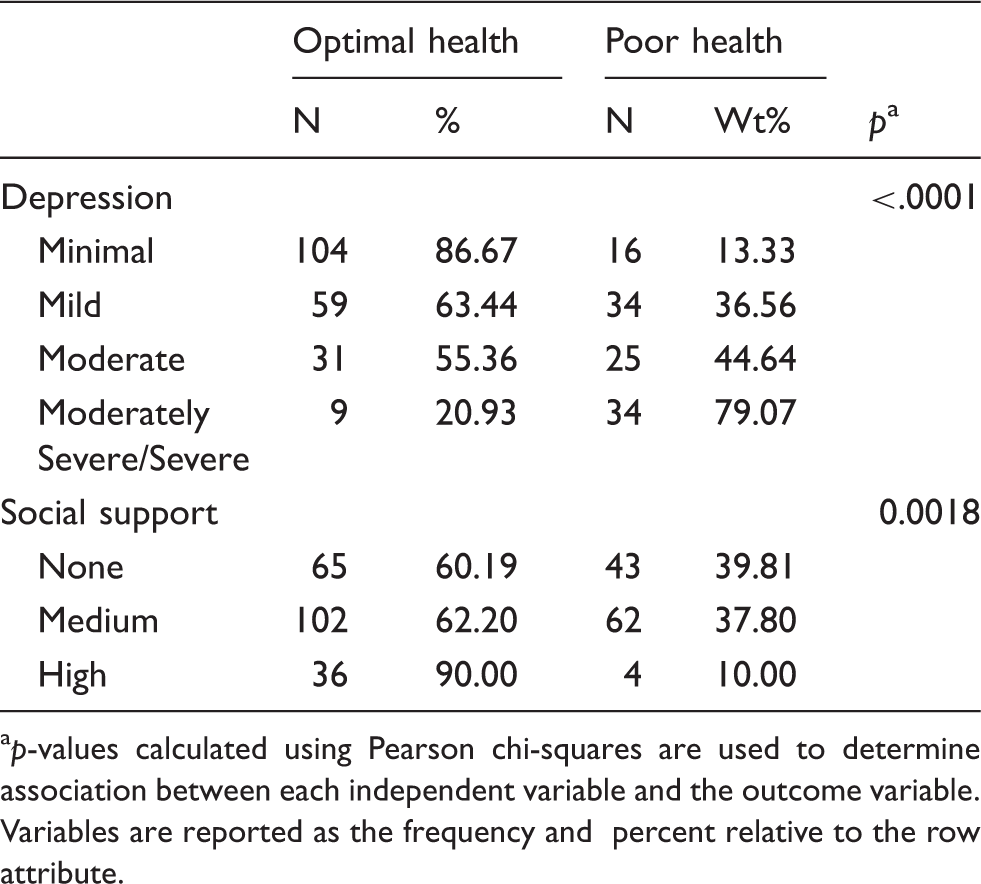
ap-values calculated using Pearson chi-squares are used to determine association between each independent variable and the outcome variable. Variables are reported as the frequency and percent relative to the row attribute.
Association between depression, social support and the presence of poor overall health among PLWHA (N = 312).
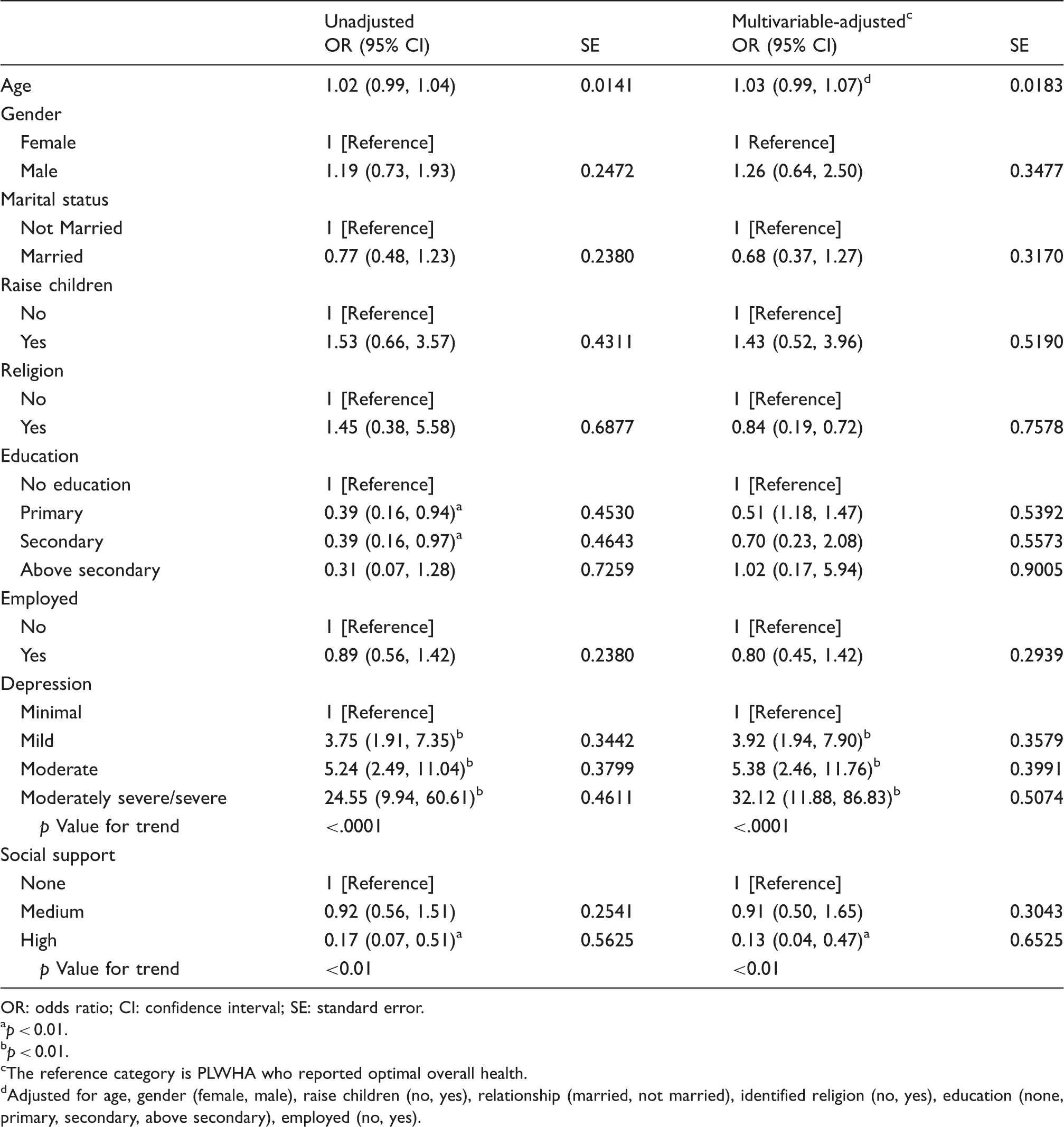
OR: odds ratio; CI: confidence interval; SE: standard error.
ap < 0.01. bp < 0.01.
cThe reference category is PLWHA who reported optimal overall health.
dAdjusted for age, gender (female, male), raise children (no, yes), relationship (married, not married), identified religion (no, yes), education (none, primary, secondary, above secondary), employed (no, yes).
Association between depression, social support and the presence of poor overall health stratified by gender (N = 312).
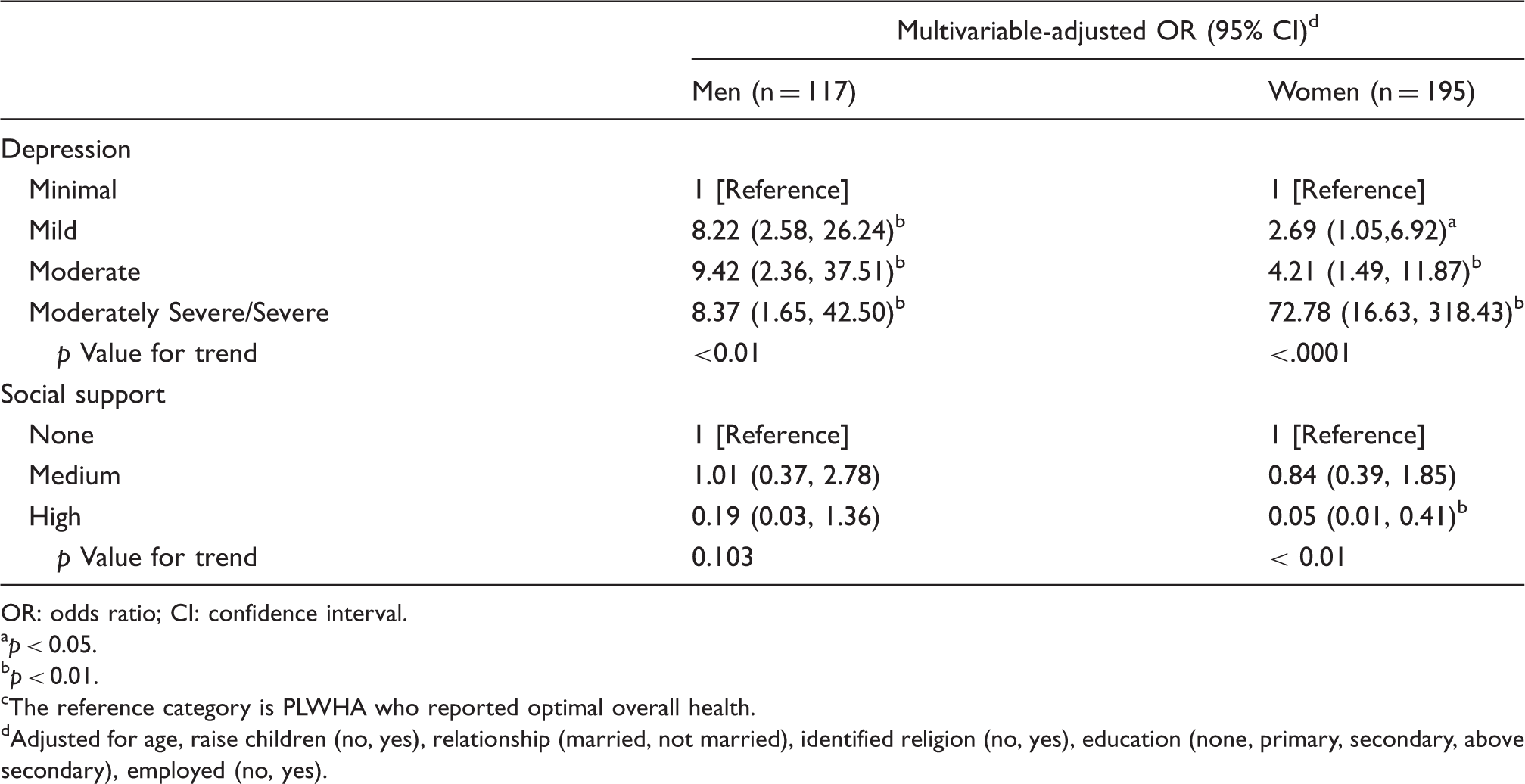
OR: odds ratio; CI: confidence interval.
ap < 0.05.
bp < 0.01.
cThe reference category is PLWHA who reported optimal overall health.
dAdjusted for age, raise children (no, yes), relationship (married, not married), identified religion (no, yes), education (none, primary, secondary, above secondary), employed (no, yes).
Discussion
In the targeted sample of PLWHA, severe depression and lack of sufficient social support were found to be associated with poor overall health. The observed association was independent of age, gender, whether or not participants raise children, relationship status, participants' association with religion, level of education, and employment status. Similar to documented research, our findings suggest that among PLWHA, depression and lack of social support may be associated with a negative impact on overall health.
Over the past few years, attention has been given to the prevalence and increased risk of depression among PLWHA in Kenya.6,27–30 The main theme running across these studies is the need to include depression as part of their treatment plan to enhance HIV prevention strategies (medication adherence, disclosure of serostatus to sexual partners, and condom use).5,12–16 Additionally, past literature on estimates of the prevalence of major depressive disorders among PLWHA indicates a wider range from 1.9% to 35% in clinical samples and from 30% to 65% in community samples while lifetime prevalence of depression estimated at 20% to 45%.31–33 In our study sample, we found severe depression in 14% of the clinical participants. However, our findings were self-reported and depressive symptoms were not confirmed by any clinician. Future research engaging in clinical screening of depression may supplement self-reported diagnosis.
Nevertheless, PHQ-9, which was used to measure depression symptoms in targeted sample, revealed a high internal consistency and has previously been used in Kenya and globally among PLWHA.20–26 Therefore, PHQ-9 is deemed a reliable tool for measuring depression symptoms given its utilization globally and reliability scores. Overall, it is challenging to definitively ascertain whether depression increases HIV-infected persons' risk for disease progression, or whether HIV disease progression is associated with increased risk of depression. 32
Regarding overall health, our findings add confirmation to previously reported association between depression and overall health among PLWHA.6,34–,38 While the reported link is informative, we should note that in the current study, majority of the participants were of low socio-economic status (SES) (primary education, low-income community, and high unemployment), which could have placed them at risk for depression and consequent poor overall health39–41 prior to a diagnosis of HIV infection. Hence, it is likely that participants may have had previous depression symptoms prior to HIV diagnosis, which could have been exacerbated after the diagnosis. SES (education, income, employment) influence and a previous diagnosis of depression prior to HIV diagnosis was not examined in this paper, but it is worth mentioning given the reported influence of SES on overall health.39–41 This relationship can further be examined utilizing longitudinal studies to determine whether SES is an independent risk factor accountable for depression among PLWHA.
With respect to social support, previous studies have shown a positive association between social support and improved health outcomes in PLWHA.42–44 While the exact mechanisms by which social support improves health outcomes are yet to be discerned, speculations regarding the nature of this association rely on the potential contribution of social support to improving medication compliance, access to health care, psychosocial status, and reducing levels of stress.12,14,15,45 It is important for future studies to determine whether different types of social support have a greater impact on overall health among PLWHA in the long-term.
Limitations
The sample is cross-sectional and highly selective and findings can only be generalized to PLWHA receiving HIV care services in a clinic within an urban setting. Longitudinal studies examining similar constructs may likely show causal relationships. Regarding depression, we need to exercise caution during interpretation of the findings given that depression symptoms were self-reported and not clinically measured. Also, while length of HIV or AIDS diagnosis would have provided more information on the link between depression and HIV infection, those analyses were not included because of substantial missing data. Regarding social support, the categories presented to the sample may not be exhaustive to capture all types of social support available to PLWHA. Chosen categories in this study were informed by previous literature indicating the most prevalent reported types of social support among PLWHA.
In conclusion, the current paper provided additional evidence of the association between severe depression, inadequate social support, and poor overall health among PLWHA. This association is independent of potential confounders such as age, gender, whether or not participants raise children, relationship status, participants' association with an identified religion, level of education, and employment status. To that end, this study suggests that HIV clinics and interventions need to focus more on the psychological and/or mental health status of HIV-infected individuals while providing avenues such as social support groups that can be a buffer against the negative impact of HIV infection, depression on overall health outcomes.
Footnotes
Acknowledgements
We extend thanks to study participants, co-authors, statistical consultants, medical officers at AMREF-Kenya, and field assistants. Contents of the paper are solely the responsibility of the authors and do not necessarily represent any official view. Special thanks are extended to Winnie Nzioka, Dorcas Kinuthia, Walter Kibet, Yvonne Machira, Wairimu Njoroge, Dr Festus Ilako, the late Alex Thuo, Brian Derrel Powers, Blevins, Stephanie Dickinson.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partly sponsored by funding provided from the Department of Applied Health Science and School of Public Health-Indiana University in Bloomington Indiana USA.