
Abstract
Studies have suggested CD8 lymphocytes may be a possible marker for inflammation, which is believed to be a contributing factor to neurocognitive impairment. Individuals enrolled in the MSM Neurocog Study were analysed. Those with depression, anxiety or mood disorders were excluded. Individuals with neurocognitive impairment were identified using the Brief NeuroCognitive Screen and compared to those with normal scores. CD4 and CD8 T cell values and CD4:CD8 ratios were compared between groups. In all, 144 men, aged 18–50 years, were included in the analysis. Twenty were diagnosed with neurocognitive impairment. We were unable to identify any significant difference between current, nadir or peak CD4 and CD8 counts. CD4:CD8 ratios and CD4:CD8 ratio inversion (<1) were also found to be similar between both groups. However, neurocognitive impairment subjects were 8% more likely to have inversion of CD4:CD8 ratio and higher median peak CD8 cell counts reported compared to non-impaired subjects. Analysis of data from the MSM Neurocog Study, demonstrated trends in peripheral CD8 counts and CD4:CD8 ratios. However, we are unable to demonstrate any significant benefit. Plasma biomarkers of neurocognitive impairment in HIV-infected subjects would be of great benefit over current methods of invasive CSF analysis and technical neuroimaging used in the diagnosis of neurocognitive impairment. Future, prospective, longitudinal work with large numbers of neurocognitive impairment subjects is required to further investigate the role of peripheral CD8 T cells as markers of neurocognitive impairment.
Introduction
The introduction of highly active antiretroviral therapy (HAART) in the mid 1990 s led to a dramatic decline in the incidence of severe HIV-associated dementias. 1 Despite this, the incidence of mild-to-moderate neurocognitive impairment (NCI) is reported to be unchanged, even in patients with optimally controlled plasma viral loads (pVL).2,3
Guidelines on detection, monitoring and management of NCI currently include questionnaires (both paper and online), other tests of cognition, and invasive procedures such as lumbar puncture (LP) examination to allow CSF HIV RNA to be quantified. 4 Studies are ongoing looking at the role of CSF biomarkers and neuroimaging in diagnosing NCI, but relatively little research has looked at the use of biomarkers in the plasma.
There are data suggesting an association between factors such as plasma viral load (pVL) and CD4 lymphocytes in the pathogenesis of HIV-related NCI5,6 as well as more novel peripheral markers, such as CD14 and lipopolysaccharides, as indicators of activity of neurological disease.7,8 Although there is still limited evidence in the literature determining the role of CD8 T cells in HIV-related NCI, studies have suggested CD8 lymphocytes may be a possible marker for inflammation, which is believed to be a contributing factor to NCI.9,10
The recent observation of CD4:CD8 ratio association with markers of age-associated disease in virally suppressed individuals with immunological recovery 11 strengthens the requirement for data on the role of CD8 T cells in NCI. Serrano-Villar and colleagues 11 observed inversion of the CD4:CD8 ratio in virally suppressed individuals with CD4 T cell restoration, which led them to suggest that peripheral oligoclonal expansion of CD8 T cells may be responsible for these observations. This expansion is considered to be a surrogate marker of immunosenescence.
A peripheral, non-invasive and cost-effective method of assessment of NCI would be a useful adjunct to allow universal early screening and subsequent monitoring and management of NCI.
Method
We retrospectively analysed data of individuals enrolled into the MSM Neurocog Study between September 2011 and June 2012. Patients enrolled are men who have sex with men (MSM) aged 18–50 years (there is a separate clinic for patients aged over 50). Individuals who scored highly for depression and anxiety using the physical health questionnaire 9 (PHQ9) and general anxiety and depression score 7 (GAD) prior to neurocognitive testing were excluded from our analysis. Individuals with formally diagnosed mood disorders were also excluded.
Subjects were screened using the Brief NeuroCognitive Screen (BNCS). This included Trail Making A and B tests and digital symbol testing (DST). BNCS scores were interpreted by constructing composite neuropsychometric Z (NPZ) scores. Published normal ranges for the BNCS are historical and it is not yet clear which normal values are most appropriate for use in an HIV-infected population. We constructed a normal range based on participants in the study, and identified those with potential NCI by comparing individual values with this range. There are some potential flaws to this approach, mainly that it is likely to under-identify NCI rather than over-identify it (unlike the high sensitivity required for a screening test). However, the benefit of this approach is that it makes it more likely that those identified are truly impaired. This approach remains open to criticism. Individual comparison to published normal values is currently underway.
Electronic patient records were used to collect HIV-associated laboratory parameters from the time these tests were performed. Data were analysed using SPSS 22 software (IBM Statistics). Mann-Whitney U and Chi square with Yates correction testing was used in the analysis of patients with potential NCI compared to those with normal scores on the BNCS neurocognitive testing. The median current, peak and nadir CD4 and CD8 T cell values were compared between groups along with the CD4:CD8 ratios, pVL and CD3 count to ascertain whether there was any difference in parameters in those presenting with NCI.
Results
Patient demographics from the MSM Neurocog Study group (Sept. 2011 to June 2012) for significance of CD8 T cells in neurocognitive impairment (NCI).
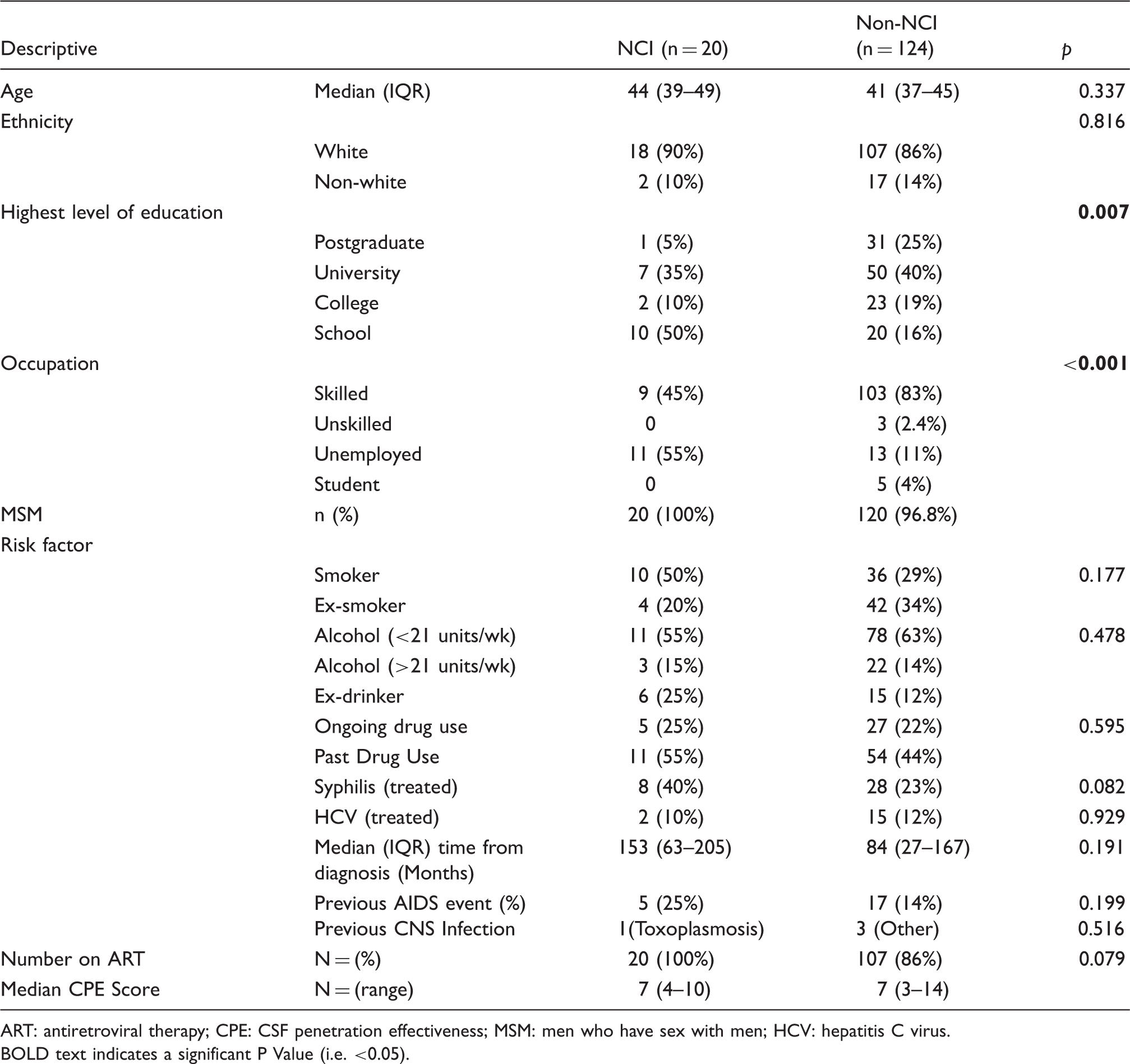
ART: antiretroviral therapy; CPE: CSF penetration effectiveness; MSM: men who have sex with men; HCV: hepatitis C virus.
BOLD text indicates a significant P Value (i.e. <0.05).
HIV parameter analysis from the MSM Neurocog Study group (Sept. 2011 to June 2012) for significance of CD8 T cells in NCI.
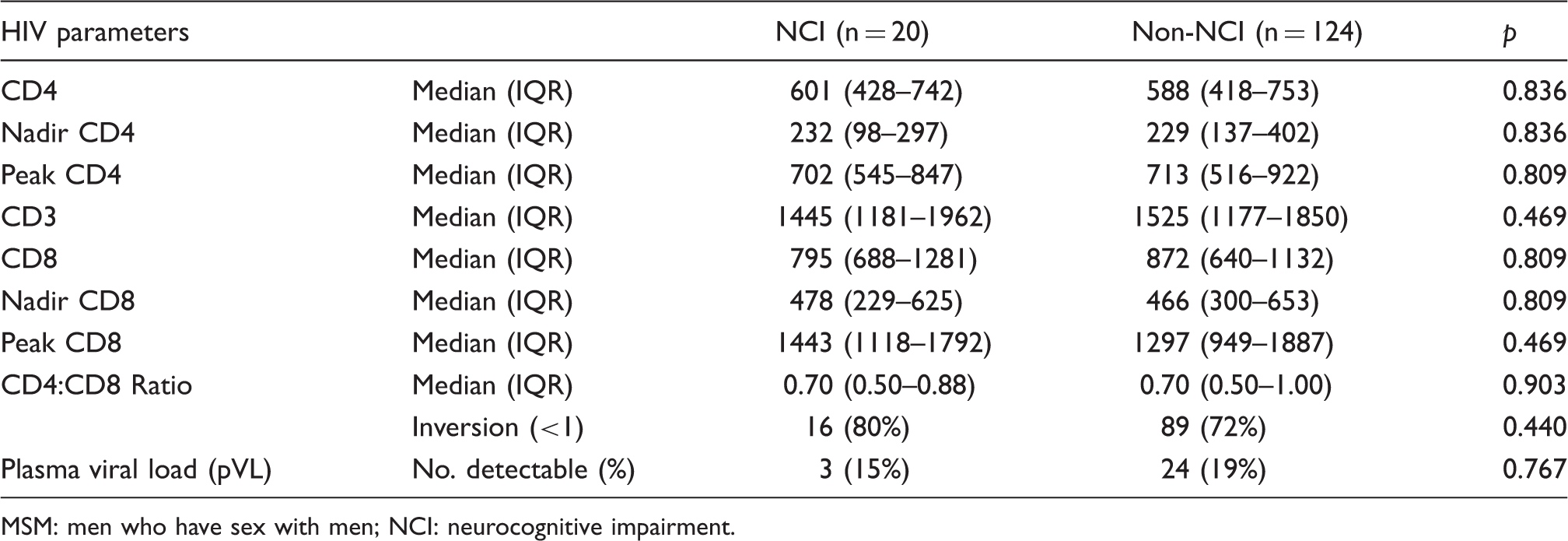
MSM: men who have sex with men; NCI: neurocognitive impairment.
Out of the 144 patients screened in the clinic, 20 were identified as potentially having NCI; 124 had BNCS scores within the normal range on NCI screening. We were unable to identify any significant difference between the subjects’ median age (44 vs. 41 p = 0.054) and sexuality (MSM 44 vs. 120 p = 1.00). No significant difference was identified between available risk factor information (Table 1). All subjects in the NCI group were currently on antiretroviral therapy (ART) with 107 (86% p = 0.079) of the non-impaired group on ART. The median CSF penetration effectiveness (CPE) scores for both groups was 7 (p = 0.082). CPE scores were calculated using the 2010 scoring system. 12
In the NCI group 5% (n = 1) compared to 25% (n = 35) of the non-impaired group had achieved post-graduate education, with these subjects also achieving significantly higher levels of education overall (p = 0.007). Of non-impaired subjects, 83% (n = 103) were currently in skilled work compared to 45% (n = 8) in the NCI group; 55% (n = 11) of the NCI cohort were currently unemployed compared for 11% (n = 13) in the non-impaired group (p < 0.001).
We were unable to identify any significant difference between current, nadir or peak CD4 and CD8 counts. CD4:CD8 ratios, CD4:CD8 ratio inversion (<1), the number of detectable and undetectable pVLs and peak pVL were also found to be similar between both groups (Table 2).
Discussion
In our analysis of 144 subjects from the MSM Neurocog Study we have been unable to identify any significant difference in peripheral CD8 T cell markers between our NCI and non-NCI group. This included analysis of current, nadir and peak CD8 T cell counts as well as CD4:CD8 ratios. We did identify that non-NCI patients were significantly more likely to have a higher level of education and be employed in more skilled labour jobs (p = 0.007 and p < 0.001, respectively) than NCI patients.
Recent evidence has suggested that CD8 T cell levels may be reduced in patients with different types of NCI.9,13–15 It has been postulated that this may come about as part of peripheral redistribution of immature CD8 cells during their recruitment to sites of inflammation in the CNS, 16 which is thought to be a major contributing factor to NCI.9,10 Vivithanaporn et al. 9 demonstrated in a cohort of 404 patients, with one or more neurological disorder, that patients were likely to have lower plasma nadir CD8 T cell levels than controls. Others have also reported low absolute CD8 T cell levels association with NCI.13–15 Sanchez-Ramon et al. 15 observed that lower circulating CD8 T cells predicted progressive encephalitis in HIV-positive children. A hypothesis is that low peripheral CD8 T cells may be associated with trafficking of CD8 T cells from the periphery into the brain with subsequent NCI due to brain inflammation. This hypothesis is supported by data describing the relatively rare phenomenon of CD8 T cell encephalitis in HIV-positive individuals, especially those on HAART. 16 Langford and Letendre reviewed the current literature describing large increases in recruitment and infiltration of CD8 T lymphocytes into the CNS during this phenomenon. 16 They liken the pathogenesis to that seen in immune reconstitution inflammatory syndromes with non–HIV pathogens, such as the JC virus and Cryptococcus neoformans. Interestingly, they also suggest that peripheral redistribution of lymphocyte cell populations may be involved in the recruitment of immature CD8 + CD38+ cells into the CNS during this process. Currently, detection and diagnosis of such phenomenon requires either invasive assessment of CSF and brain matter or the use of post-contrast T1–spin echo with magnetic transfer MRI. 16
Serrano-Villar and colleagues 11 recently demonstrated that inversion of CD4:CD8 ratio (<1) in treated HIV subjects was a marker of age-associated disease including atherosclerosis, renal function and muscle wasting. This led them to conclude that it may also be a useful predictor of non-AIDS-defining conditions. 11 These observations, in the face of good CD4 T cell response to HAART, has led the authors to suggest that oligoclonal expansion in CD8 T cell populations was responsible for their findings. This is a surrogate maker for immunosenescence which is a predictor of all-cause mortality.17,18
In our cohort, we were unable to identify any significant difference in peripheral CD8 T cells (Table 2) or CD4:CD8 ratio inversion (p = 0.440) between NCI and non-NCI subjects. This is a retrospective, observational analysis not powered to identify statistical differences in CD4/CD8 counts and we can comment only on trends. On analysis of our data, we observe a 12% reduction in current CD8 count at presentation in the NCI group (795 and 872) and peak CD8 count was 10% higher in the NCI subjects (1443 and 1297). CD4:CD8 ratio inversion (<1) is 8% more common in the NCI group. A larger, prospective, suitably powered study is necessary to confirm significance.
Our findings may have been limited by a number of factors including the relatively small number of individuals with NCI (n = 20) out of our cohort of 144 subjects. This is a notably lower prevalence of NCI observed in our cohort compared to that reported from large cross-sectional observational studies, such as the CNS HIV Antiretroviral Therapy Effects Research (CHARTER) study. 3 This is likely to be due to the fact that subjects included in our study were young. Secondly, screening of patients for NCI involved brief tests, easily delivered in a routine clinic, but were not diagnostic, with extensive neuropsychological batteries being time-consuming and expensive. 19 There have been previous concerns regarding these tests ability to correctly identify patients with NCI, especially milder forms. However, current evidence suggests that use of multiple, neuropsychological tests with short implementation times demonstrate adequate sensitivity and specificity in detecting NCI when compared to more intensive batteries. 19 Finally, examination of the MSM Neurocog Study has also demonstrated that patients with anxiety and depression perform worse in NCI screening testing (unpublished data). These patients were excluded from our cohort before analysis which may have also had an impact on the prevalence of NCI in our cohort.
In conclusion, from retrospective analysis of data over a 10-month period from the MSM Neurocog Study, despite showing trends in CD4:CD8 ratio inversion and CD8 T Cell counts, we are unable to demonstrate any significant benefit in monitoring CD8 T cells or CD4:CD8 T cell ratio inversion as an indicator of NCI. Plasma biomarkers of NCI in HIV-infected subjects would be of great benefit over current methods of invasive CSF analysis and technical neuroimaging used in the diagnosis of NCI. Future, prospective, longitudinal work with large numbers of NCI subjects is required to further investigate the role or peripheral CD8 T cells role as markers of NCI.
Footnotes
Acknowledgements
The authors thank all patients who took part in the MSM Neurocog study and the staff in the St. Stephen’s Centre who helped to recruit participants.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.