
Abstract
Local genital tract inflammation stimulates leukocyte activity and causes HIV shedding, potentially increasing HIV sexual infectiousness. Although there are available clinical markers for genital tract inflammation, such as urinary leukocyte esterase, none have yet been examined in relation to HIV sexual risk behaviours. We sought to examine the association between urinary leukocyte esterase and sexual practices. Sexually active men living with HIV and receiving antiretroviral therapy (ART, N = 290) provided urine specimens and completed behavioural health assessments. HIV RNA tests and CD4 cell counts were abstracted from medical records. Urine specimens were analysed for leukocyte esterase using a standard point-of-care dipstick test. Thirty-one (10.6%) participants tested positive for leukocyte esterase. Logistic regression models did not indicate differences between men with elevated and un-elevated leukocyte activity on demographic, health, recent sexually transmitted infection symptoms and diagnoses or substance use. However, men with elevated leukocyte activity indicated significantly greater sexual behaviour in the previous three months, including more recent unprotected sexual intercourse. A simple over-the-counter urine test may serve as an indicator of sexual HIV infectiousness to inform further evaluation and treatment of genital tract inflammation, as well as condom use decisions during times of increased genital tract inflammation.
Keywords
Introduction
Antiretroviral therapies (ARTs) effectively suppress HIV replication and have the potential to reduce sexual infectiousness, forming the basis for using HIV treatments as prevention. Most ART regimens penetrate the urogenital compartment of the immune system and suppress HIV in genital secretions. 1 HIV RNA is typically undetectable in the semen of men who achieve blood plasma HIV suppression and do not have co-occurring genital tract inflammation. 2 The biological plausibility of using HIV treatments for prevention is well established, 3 with the most compelling evidence coming from a clinical trial showing early treatment with ART can prevent HIV transmission in heterosexual couples. 4 Still, it is widely known that HIV shedding occurs even when peripheral blood plasma viral activity is suppressed and even in the absence of symptomatic genital infections. 5
HIV suppression in blood plasma is often erroneously assumed to always correspond with HIV-1 RNA in genital secretions and therefore mistakenly interpreted as an indicator of sexual infectiousness.6,7 High concordance between blood plasma and semen HIV RNA has only occurred under controlled conditions that assure perfect adherence to a virally suppressive ART regimen and intensive screening, diagnosis and treatment of co-occurring sexually transmitted infections (STIs).2,8 Studies testing the association between HIV RNA in blood plasma and semen in typical clinical samples find a modest average correlation of 0.44. 5 One study demonstrated no relationship between blood plasma and semen HIV RNA; 53% of men with undetectable HIV RNA in blood plasma had detectable virus in semen and 31% of men with undetectable virus in semen had detectable blood plasma virus. 9
Local inflammation of the genital tract activates HIV replication, shedding virus and therefore increasing HIV infectiousness.10,11 Genital tract inflammation can recreate magnitudes of infectiousness that are otherwise only seen in acute HIV infection. 12 Although HIV RNA in genital secretions tends to be lower than HIV RNA in blood plasma, this relationship can be inverted in the presence of genital tract inflammation. 13
Genital tract HIV RNA is directly associated with the number of leukocytes present. There is indeed a dose-relationship between leukocyte activity in the genital tract and HIV shedding. 14 In one prospective study, for example, the odds of detecting genital tract HIV RNA increased 1.36 for every 1000 cell increase in genital tract leukocytes. 15 Past research has shown that urethritis is associated with an eightfold increase in HIV in the seminal plasma compartment. 16 As much as 40% discordance is observed between seminal and blood viral populations and the complexity of viral populations differs between the two compartments, suggesting at least partial independence of the blood and genital compartments.16–18 An easily performed and inexpensive test for genital tract leukocyte activity, may therefore serve as a marker for HIV infectiousness that could inform the practice of HIV treatment as prevention.
The current study is the first to report the association between urinary leukocyte esterase (LE) and sexual behaviours in men living with HIV infection. Leukocyte activity is monitored by an easily performed urine test to detect LE – an indicator of local lower urogenital tract inflammation. LE in urine is detected using a simple over-the-counter dip-test and therefore offers a point-of-care or home test for genital tract inflammation. Research shows that elevated LE is sensitive to detecting genital tract inflammation, with low specificity for detecting STIs. 19 Exposure to sexually transmitted pathogens, including re-exposure to HIV, as well as urogenital stimulation and other sources of inflammatory response that can result from HIV seroconcordant sexual relationships can increase HIV infectiousness and therefore increase risks to uninfected sex partners. In the current study, we hypothesised that elevated LE in men living with HIV infection and receiving ART would demonstrate greater recent sexual activity than their counterparts with un-elevated LE. In addition, we predicted that the association between LE and sexual behaviour could be indicative of multiple sources of genital tract inflammation and would therefore occur in the context of low-rates of STI symptoms and diagnoses.
Methods
Participants
Men living with HIV/AIDS who were currently receiving ART (N = 290) were reached through community recruitment strategies. Individuals interested in participating approached our research programme to schedule an intake assessment appointment. The study entry criteria were (a) biologically man and 18 years of age or older, (b) HIV positive and prescribed ART and (c) sexually active as defined by having at least one sex partner in the previous month.
Measures
Participants provided four sources of data. First, participants completed audio-computer assisted self-interviews to assess demographic, health and behavioural characteristics at the start of the study. Second, we assessed medication adherence using phone-based unannounced pill counts. Third, we collected HIV RNA (viral load) and CD4 cell counts using a participant-assisted medical chart abstraction procedure. Finally, participants provided urine specimens for substance use screening and LE testing.
Computerised interviews
Demographic and health characteristics
Participants were asked their gender, age, years of education, income, ethnicity and employment status. Participants also reported the year they first tested HIV positive and whether they had experienced 14 HIV-related symptoms of 2-weeks duration. To assess alcohol use we administered the Alcohol Use Disorders Identification Test (AUDIT), a 10-item scale designed to measure alcohol consumption and identify risks for alcohol abuse and dependence. 20 Scores on the AUDIT range from 0 to 40 and the AUDIT with scores greater than eight indicating high-risk for alcohol use disorders and problem drinking.
Sexual health
Participants reported whether they had experienced three common STI symptoms and whether they had been diagnosed with any of the eight non-HIV STIs or sources of genital disease during the past three months (see section Results for symptoms and diagnoses).
Sexual behaviour
Participants responded to questions assessing their number of male and female sex partners and frequency of sexual behaviours (anal and vaginal intercourse) with seroconcordant (i.e. same HIV status) and serodiscordant (i.e. different HIV status) partners in the previous three months. Studies show that a 3-month retrospective timeframe yields reliable estimates of sexual behaviour. 21 These data were collected specific to the participant’s practices as the insertive or receptive partner during anal sex. In addition, we assessed anal sex with male and female partners and combine these behaviours for insertive anal intercourse. We present sexual behaviour data as composites (i.e. total intercourse, condom-protected intercourse and unprotected intercourse) and for individual acts (i.e. unprotected anal intercourse as the insertive partner with HIV-serodiscordant partners).
ART adherence
Participants consented to three unannounced telephone-based pill counts over the course of six weeks constituting a prospective measure of adherence. Unannounced pill counts are reliable and valid in assessing medication adherence when conducted in homes 22 and on the telephone.23,24 In this study, we conducted unannounced cell phone-based pill counts. Participants were provided with a free cell phone for use in the study assessments. Following office-based training in the pill-counting procedure, participants were called at unscheduled times by a phone assessor. Pill counts were unscheduled and occurred over 21–35-day intervals. Participants counted each of the antiretroviral medications they were taking. Pharmacy information from pill bottles was also collected to verify the number of pills dispensed between calls and whether there was a lapse in obtaining medications from the pharmacy. Adherence was calculated as the ratio of pills counted relative to pills prescribed, taking into account the number of pills dispensed, and averaged across pill counts to yield one-month adherence.
Chart abstracted viral load and CD4 cell count
We used a participant-assisted method for collecting chart-abstracted HIV RNA viral load and CD4 cell counts from medical records. Participants were given a form that requested their doctor’s office to provide results and dates of their most recent viral load and CD4 cell counts. These data were therefore obtained directly by the participants from their primary HIV care providers. The form included a place for the provider’s office stamp or signature to assure data authenticity.
Urinalysis and drug testing
Urine specimens were first tested for LE and nitrites. We performed a chemstrip test for the presence of LE, an enzyme that is indicative of urinary tract inflammation. Granulocytic leukocytes contain esterases that catalyse the hydrolysis of an indoxylcarbonic acid ester to indoxyl, which reacts with a diazonium salt to produce a purple colour on the test strip. Specimens were tested with over-the-counter ‘urine dip’ Roche Chemstrips 2 LN (cost US$0.16 each) and read on-site at the research office. Although chemstrips can be visually read for colour change at no cost, we processed the chemstrips using the Roche Urisys 1100 Urine Analyzer (cost $1200). Using the same chemstrips, we also tested for nitrites, indicative of an upper urinary tract infection or renal disease to differentiate potential upper and lower urogenital tract sources of inflammation.
Following LE and nitrite testing we used a multi-panel dip-test to detect illicit drug metabolites in participants’ urine specimens. Drug detection used a lateral flow chromatographic immunoassay for qualitative detection of 12 drugs and drug metabolites (Redwood Toxicology Labs – Reditest-12). The test is US Food and Drug Administration approved and is sensitive and specific for initial drug screening.
Procedures
Men living with HIV were recruited through targeted community sampling. We used both venue recruitment and snowball sampling techniques. Recruitment relied on responses to brochures placed in waiting rooms of HIV service providers and infectious disease clinics throughout Atlanta, GA. We also implemented an explicit systematic approach to word-of-mouth chain recruitment. Specifically, participants were given brochures that described the study opportunity and were encouraged to use the brochures to refer their HIV-positive friends to the study.
Participants provided informed consent and completed the computerised interviews. Participants were then instructed in procedures to conduct unannounced pill counts and how to obtain their most recent CD4 cell count and HIV RNA viral load test results from their medical provider. We also asked participants to provide a first catch urine specimen during this office visit. Participants who tested LE positive were informed of their test results and given a written explanation to take to their medical provider. Drug test results were provided to participants upon request. Participants received US$120 for completing all study measures and procedures. The university Institutional Review Board approved all procedures and protocol changes.
Data analyses
Logistic regressions were performed to test associations between men who did not (N = 259) and men who did (N = 31) test LE positive. Significance tests were performed on composite sexual behaviours (e.g. anal intercourse) to eliminate overlap and avoid statistical redundancy. Analyses of sexual behaviours controlled for participant age and years since testing HIV positive. Significance tests were not performed for sparse tables (cell sizes <5). For all analyses we report odds ratios with 95% confidence intervals. Statistical significance was defined by p < 0.05.
Results
Among the 290 sexually active men living with HIV and receiving ART, 31 (10.6%) tested LE positive, of which 18 (58%) demonstrated trace levels and 13 (42%) showed significantly elevated LE.
Demographic and health characteristics
Demographic and health characteristics of HIV-infected men testing negative and positive for urinary leukocyte esterase (LE).
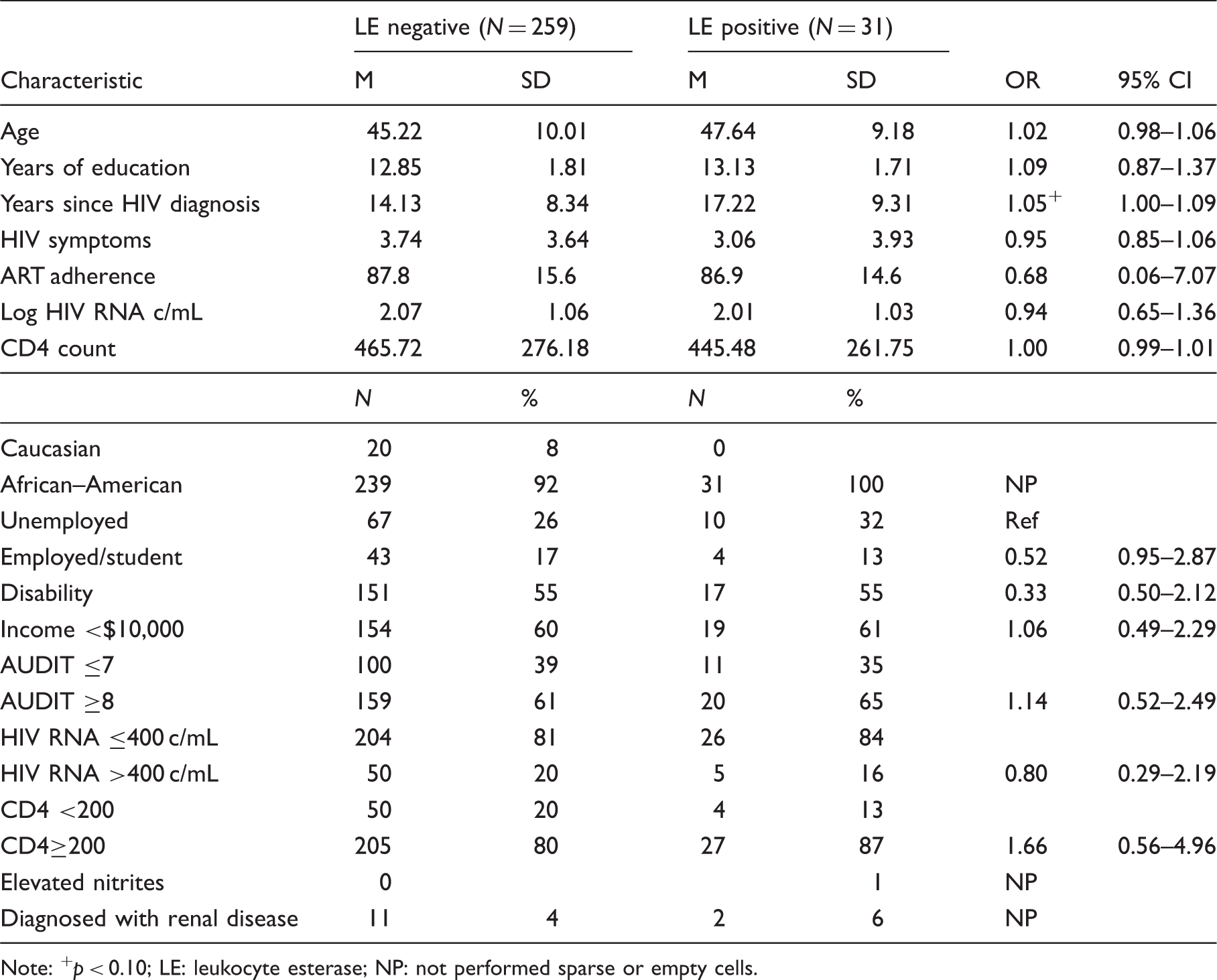
Note: +p < 0.10; LE: leukocyte esterase; NP: not performed sparse or empty cells.
Substance use
Substance use among HIV-infected men testing negative and positive for urinary leukocyte esterase (LE).

Note: LE: leukocyte esterase; NP: not performed due to sparse or empty cells.
Sexual health history
Sexual health characteristics of HIV-infected men testing negative and positive for urinary leukocyte esterase (LE).
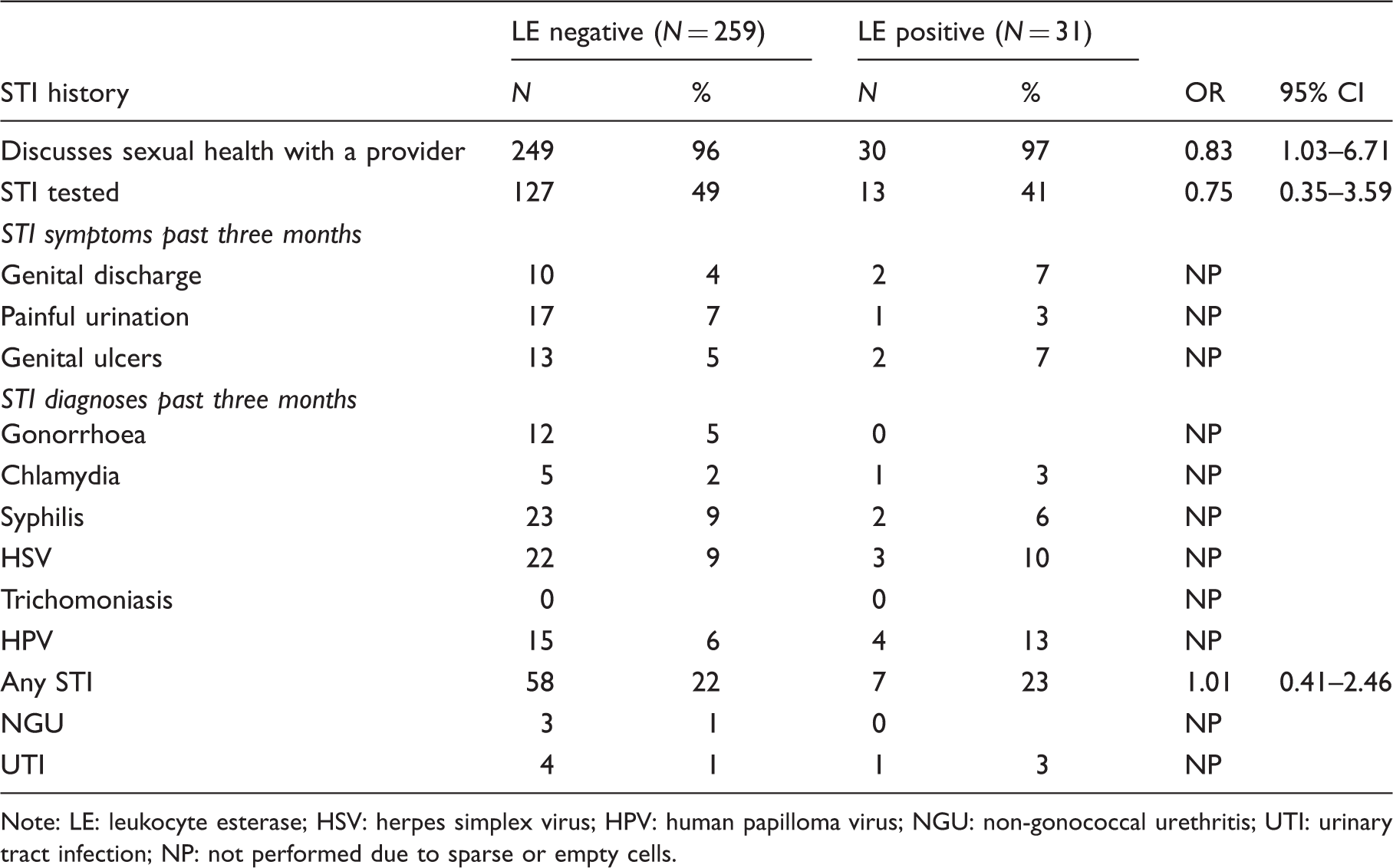
Note: LE: leukocyte esterase; HSV: herpes simplex virus; HPV: human papilloma virus; NGU: non-gonococcal urethritis; UTI: urinary tract infection; NP: not performed due to sparse or empty cells.
Sexual behaviour
Sexual behaviours among HIV-infected men testing negative and positive for urinary leukocyte esterase (LE).

Note: +p < 0.10; *p < 0.05; **p < .01; LE: leukocyte esterase.
Results showed that LE-positive participants had significantly more total sexual acts and a trend towards greater total unprotected sexual intercourse compared to their LE-negative counterparts. Examination of sexual behaviours by partner HIV status indicated that LE-positive participants had higher rates of total sex and unprotected intercourse with HIV seroconcordant partners than the LE-negative group. Both LE groups reported unprotected anal and vaginal intercourse with HIV uninfected partners, with no significant differences.
Discussion
More than one in five men living with HIV in this study reported having been diagnosed with an STI in the previous three months. Over 40% had two or more sex partners in that time period, and one in four reported unprotected anal or vaginal intercourse with HIV non-infected partners. In addition, ART adherence was suboptimal for many men, with an average of 85% of ART taken over the prospective month. These results therefore demonstrate considerable potential for HIV transmission to uninfected partners, with these risks significantly amplified by genital tract inflammation.
This is the first study that we are aware to examine sexual practices in association with any marker for genital tract inflammation in sexually-active HIV-positive men. We found that 10% of participants tested positive for elevated urinary LE, indicating local genital tract inflammatory processes that likely correspond with increased HIV infectiousness. Elevated LE was not explained by recent STI symptoms or diagnoses. Consistent with past research, elevated LE was therefore not indicative of STI. 19 The prevalence of elevated LE in this sample is therefore likely to reflect inflammatory disease processes other than those caused by a current STI. Furthermore, we did not observe associations between LE and demographic, health or substance use characteristics. Thus, confirming our study hypothesis, only rates of recent sexual practices, particularly unprotected anal and vaginal intercourse, were significantly associated with elevated LE. Our findings suggest higher rates of unprotected sex with HIV seroconcordant partners may contribute to increased infectiousness. Importantly, the resulting increased HIV infectiousness will translate to higher risks for HIV transmission during unprotected intercourse with HIV serodiscordant partners. Thus, while serosorting may be a useful risk reduction strategy for HIV-positive men who restrict their sexual relationships to HIV-positive partners, it may inadvertently increase HIV infectiousness and therefore increase risks to uninfected sexual partners.
HIV RNA concentrations in semen are elevated when inflammatory processes stimulate HIV shedding. LE testing may offer a screening test for genital tract inflammation of potential value in clinical settings. Detecting genital tract inflammation with LE testing is particularly important in sexually-active people living with HIV because evidence for inflammatory disease processes can indicate increased risks for HIV infectiousness. Although LE tests are commonly used to screen for potential STIs,25,26 other sources of inflammation would similarly increase HIV infectiousness. Genital tract inflammation resulting from incomplete STI treatment, urethritis, chronic prostatitis, viral pathogens including HSV, HPV and re-exposure to HIV, as well as other non-specific causes including substance use are all putative candidates for explaining the elevated LE observed in the current study.27–32
These findings should be interpreted in light of the study limitations. First, we relied on a convenience sample that cannot be considered representative of men living with HIV infection. The sample also came from a wide range of providers that likely varied in sexual health services. Because the interpretation of elevated urinary leukocytes is different between genders, we did not include women in this study. Future research is therefore needed to replicate these results in women living with HIV. The study also relied on self-report instruments to assess sexual behaviours. Although we collected sexual behaviours using modern computerised interviews, these data may still be subject to reporting biases. Socially sensitive behaviours such as sexual behaviours and STIs assessed by self-report may be underreported, suggesting that rates of unprotected sex in this study should be considered lower-bound estimates. Another limitation of the current study is our assumption that elevated LE is associated with increased HIV infectiousness. However, studies of genital tract inflammation in relation to HIV RNA in semen support this assumption.10,15 Our cross-sectional study design precludes directional interpretations of the findings, such that the observed associations between sexual behaviours and elevated LE activity may be the result of a third variable, such as substance use. Prospective research is therefore needed to rule out potential confounding variables.
We conclude that elevated LE is associated with unprotected sexual behaviours in men living with HIV infection and may serve as a surrogate marker for increased HIV transmission risks for sexually active men receiving ART. If confirmed by subsequent research, this inexpensive (US$0.16) and easily-performed over-the-counter urine test could be integrated into the standard of care for using HIV treatments as prevention to inform clinical decisions for further evaluation and treatment of genital tract inflammation and behavioural decisions regarding the use of condoms during times of increased genital tract inflammation. Should studies confirm these associations, the results may be used to design interventions. For example, HIV-positive individuals may be counselled to refrain from unprotected sex when they have tested positive for elevated LE. In addition, counselling may counter-compensate for sexual activity that could accompany results of negative LE testing. These interventions will be especially warranted for persons who use home LE testing to inform them of their sexual infectiousness. Sexual health messages should therefore be developed to accompany the interpretation of both positive and negative LE testing among people living with HIV.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by National Institute of Drug Abuse Grant R01-DA017399.