
Abstract
Prevalence estimates of various bacterial sexually transmitted infections in South Africa have declined considerably since the mid-1990s. Syphilis among pregnant women, for example, declined from 10.8% in 1998 to 2.8% in 2001. We used Pearson’s correlation coefficients to estimate the association between the prevalence of syphilis/male urethral discharge/male genital ulcers and the peak HIV prevalence at a district and provincial level in the early and late phases of the HIV epidemic in South Africa. Prevalence estimates of syphilis, male urethral discharge and male genital ulcers during the period preceding the peak HIV prevalence were all positively correlated with the peak HIV prevalence at a provincial level (Pearson’s correlation coefficient [r] = 0.83, p = 0.006; r = 0.66, p = 0.052; r = 0.79, 0.011, respectively). These relationships all switched to a negative association later in the HIV epidemic at a provincial level (r = −0.53, p = 0.14; r = −0.73, p = 0.130; r = −0.54, p = 0.027, respectively). AIDS mortality may have played an important role in the decline of bacterial sexually transmitted infections such as syphilis in this region. Consequently, the relatively recent scale-up of antiretroviral therapy may result in a resurgence of syphilis and other sexually transmitted infections as observed in high-income countries.
Introduction
The dramatic decline in Southern Africa over the past 20 years of bacterial sexually transmitted infections (STIs) generally, and syphilis specifically, has been incompletely explained.1–5 Three factors could be responsible for this decline. First, improvements in screening and treatment of bacterial STIs may have been important. 6 Second, behaviour changes such as partner reduction or increased condom use may have been important contributors. Papers examining the decline of syphilis in Botswana and Kenya have both argued that these two factors were responsible.1,7 We investigate a third factor, AIDS mortality, which could have reduced STI incidence by disproportionately affecting persons at high risk for acquisition and transmission of STIs. A study that used regression analysis of state-level AIDS mortality rates and syphilis incidence rates for men found that AIDS mortality explained one-third to one-half of the decline in syphilis incidence among men in the United States following the peak of the AIDS epidemic. 8 Mathematical modelling of data from South Africa suggests that about 40% of the decline in syphilis prevalence between 1990 and 2005 is attributable to improved management of STIs using syndrome-based algorithms, while increased condom use and AIDS mortality accounted for the rest of the decline. 9 Which one of these factors had the greatest effect? The recent resurgence of syphilis and other STIs in high-income countries underscores the importance of getting this answer correct and mobilizing resources accordingly. 10 If improved treatment was sufficient, then maintaining national treatment programmes should suffice to keep prevalence low. However, the fact that syphilis incidence rates in men who have sex with men in the United States increased during periods of intensified syphilis outreach and treatment efforts, such as the recent syphilis eradication campaign by the US Centers for Disease Control and Prevention, suggests that more than improved diagnosis and treatment is required to avert a resurgence. 11 The increase in syphilis cases within high-income countries has been linked to a number of factors including a reduction in AIDS deaths and behavioural disinhibition in the years since HIV infection has become manageable as a chronic disease. 10 If the decline of syphilis in South Africa has been predominantly due to behaviour change and AIDS deaths, then the relatively recent and widespread introduction of antiretroviral therapy may act to reverse both AIDS deaths and behaviour change via a process similar to behavioural disinhibition. Consequently, this may lead to increases in the incidence of syphilis and other bacterial STIs.
We use a novel methodology to test whether AIDS mortality was an important driver of the decline in syphilis prevalence in South Africa. Modelling studies have demonstrated that if AIDS mortality is more likely to affect individuals who play a more central role in STI acquisition and transmission within a sexual network, then AIDS mortality could reduce STI transmission and incidence rates in that same network.12,13 This generates the following hypothesis: In the absence of antiretroviral therapy, areas where there was a higher peak HIV prevalence would have experienced a higher AIDS mortality. There would then have been a more rapid and profound decline in syphilis rates in these same areas. To test this hypothesis we assess if there is an association between peak HIV prevalence and the reduction in syphilis and other STI rates in South Africa’s provinces. In a previous analysis we used this methodology to test the association between syphilis and HIV prevalence between the countries of Southern and Eastern Africa. We found that there was a strong positive association between the syphilis prevalence in 11 countries before the HIV epidemic and national peak HIV prevalence estimates in those same countries (R2 = 0.59; p = 0.006). 14 This contrasted with the negative association between syphilis prevalence late in the HIV epidemic and peak HIV prevalence (R2 = 0.32; p = 0.07). In this study, we extend our analyses to compare the association between the prevalence of syphilis, male urethral discharge (MUD), and male genital ulcers (MGU) with peak HIV prevalence at different ecological levels within South Africa.
Methodology
HIV and syphilis prevalence
The provincial HIV and syphilis prevalence estimates for South Africa were taken from annual national antenatal HIV and syphilis surveys. South Africa has conducted antenatal surveys for HIV since 1990 and for syphilis since 1997. The methodology of these surveys has been described in detail elsewhere. 15 In summary, public sector antenatal clinics were sampled on a probability proportional-to-size basis and women attending these clinics for the first visit of their pregnancy were tested for syphilis using a rapid plasma reagin (RPR) test. No confirmatory testing with treponemal-specific assays was conducted.
The prevalence estimates for HIV and syphilis in each of South Africa’s 53 district councils were taken from the 2010 antenatal survey.
16
This was the only year that syphilis prevalence in South Africa’s antenatal surveys was reported for each district council. In the same year the Western Cape Province extended the national antenatal HIV and syphilis surveillance to all public facilities in the province so as to provide more accurate district and sub-district estimates of prevalence.
17
We obtained the HIV and syphilis prevalence for each district council in the Western Cape from this enhanced survey. These data were used to calculate the following variables.
Peak HIV prevalence. It is defined as the highest HIV prevalence in each province between 1990 and 2009. The utility of peak HIV prevalence as a means of comparing different HIV epidemics has been detailed elsewhere.
18
Early syphilis prevalence. It is defined as the syphilis prevalence in the province in 1998, the first year this was measured. In the case of Gauteng and Free State provinces, the 1999 prevalence levels were used. This was based on the large oscillations in RPR test results in these provinces between 1998 and 1999, which were thought to be due to technical factors and the fact that syphilis prevalence figures prior to 1998 in these provinces were more commensurate with the 1999 figures.17,19 Late syphilis prevalence. It is defined as the nadir of syphilis prevalence reached in the year 2002 or later. Change in syphilis prevalence. It is defined as the early syphilis prevalence minus the average post-peak HIV syphilis prevalence (defined as the mean syphilis prevalence between the years 2002 and 2011).
Incidence of MGU and MUD
The early or pre-peak HIV incidence of symptomatic STIs in men was derived from the 1998 Demographic Health Survey (DHS).
20
This survey employed a two-stage sampling strategy in South Africa’s nine provinces and stratified results into urban and non-urban groups. It was designed to be representative for all provinces, urban versus rural areas, and the four major racial groups. In total, 12,860 households were selected for the survey. Fieldwork was conducted between January and September 1998. A questionnaire was administered to all 15- to 49-year-old women in each household. In a random sample of one-half of the selected households (6459 households) all adults over 15 years of age were also identified and interviewed using a different questionnaire for adults. Only men answering this questionnaire were asked in the following manner if they had experienced symptoms of an STI:
The 2003 DHS used a similar two-stage method to sample 10,214 households and was used to provide the late or post-peak HIV estimates of MGU and MUD incidence. 21 In one-half of these households (5155 households) all men between the ages 15 and 59 were approached to recruit 3930 men. The response rates for the eligible men were 79.6% and ranged between 55.6% in the Western Cape and 92.4% in the North West. The fieldwork was conducted between October 2003 and August 2004. The men were asked the same questions relating to urethral discharge and genital ulcers as in the 1998 DHS.
The change in MGU/MUD incidence was defined as the difference between the incidence rates of MGU/MUD in 1998 and 2003.
Tabular summary of changes in prevalence of particular STI pathogens (1991–2003)
Summary of the prevalence of selected STI pathogens in clients with various STI syndromes and in general population samples from South Africa.
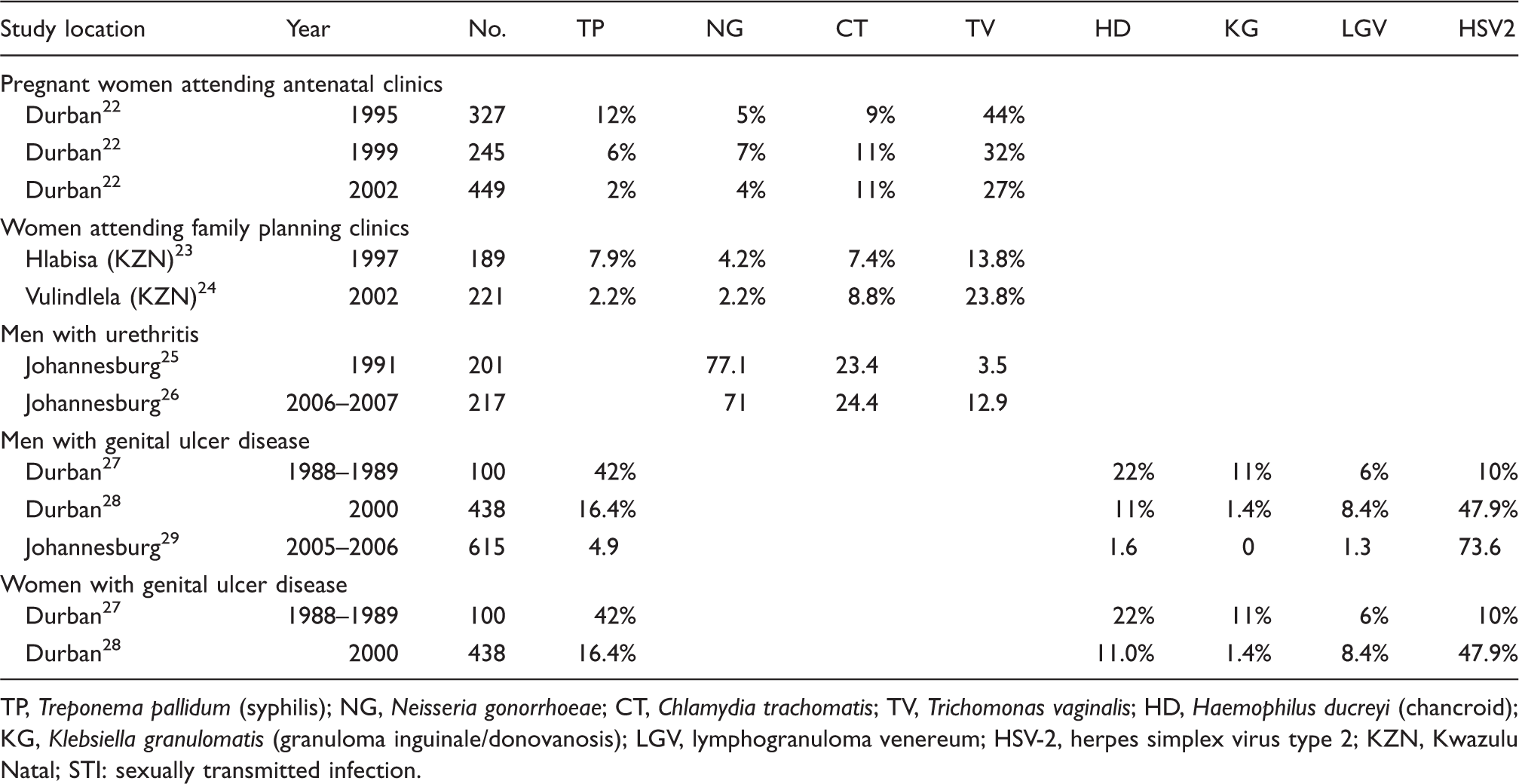
TP, Treponema pallidum (syphilis); NG, Neisseria gonorrhoeae; CT, Chlamydia trachomatis; TV, Trichomonas vaginalis; HD, Haemophilus ducreyi (chancroid); KG, Klebsiella granulomatis (granuloma inguinale/donovanosis); LGV, lymphogranuloma venereum; HSV-2, herpes simplex virus type 2; KZN, Kwazulu Natal; STI: sexually transmitted infection.
The studies providing these estimates were all, except for two, taken from the most recent review of STI sentinel surveillance data by Johnson et al. 5 The two additional studies were recently published prevalence estimates of STI pathogens in patients presenting with MUD and MGU.2,26
Statistical analyses
Pearson’s correlation coefficients were estimated for the relationship between peak HIV prevalence and early and late syphilis prevalence, early and late MUD, early and late MGU and the change in syphilis, MUD and MGU rates. Each of these analyses was performed at the level of South Africa’s nine provinces. In addition, Pearson’s correlation coefficients were estimated for the relationship between HIV prevalence and syphilis prevalence at a district council level for the whole of South Africa and the Western Cape Province. Analyses were performed using Stata 12.1 (Stata, East College Station, TX). Allowance was made for the complex sampling strategies of the DHS surveys using the survey methodology.
Results
Changes in prevalence of syphilis
South Africa’s HIV epidemic demonstrated explosive growth from 1990 (Figure 1). HIV incidence in 15- to 49-year-olds peaked in 1997, and by 2000 close to 200,000 persons were dying of AIDS per year.
30
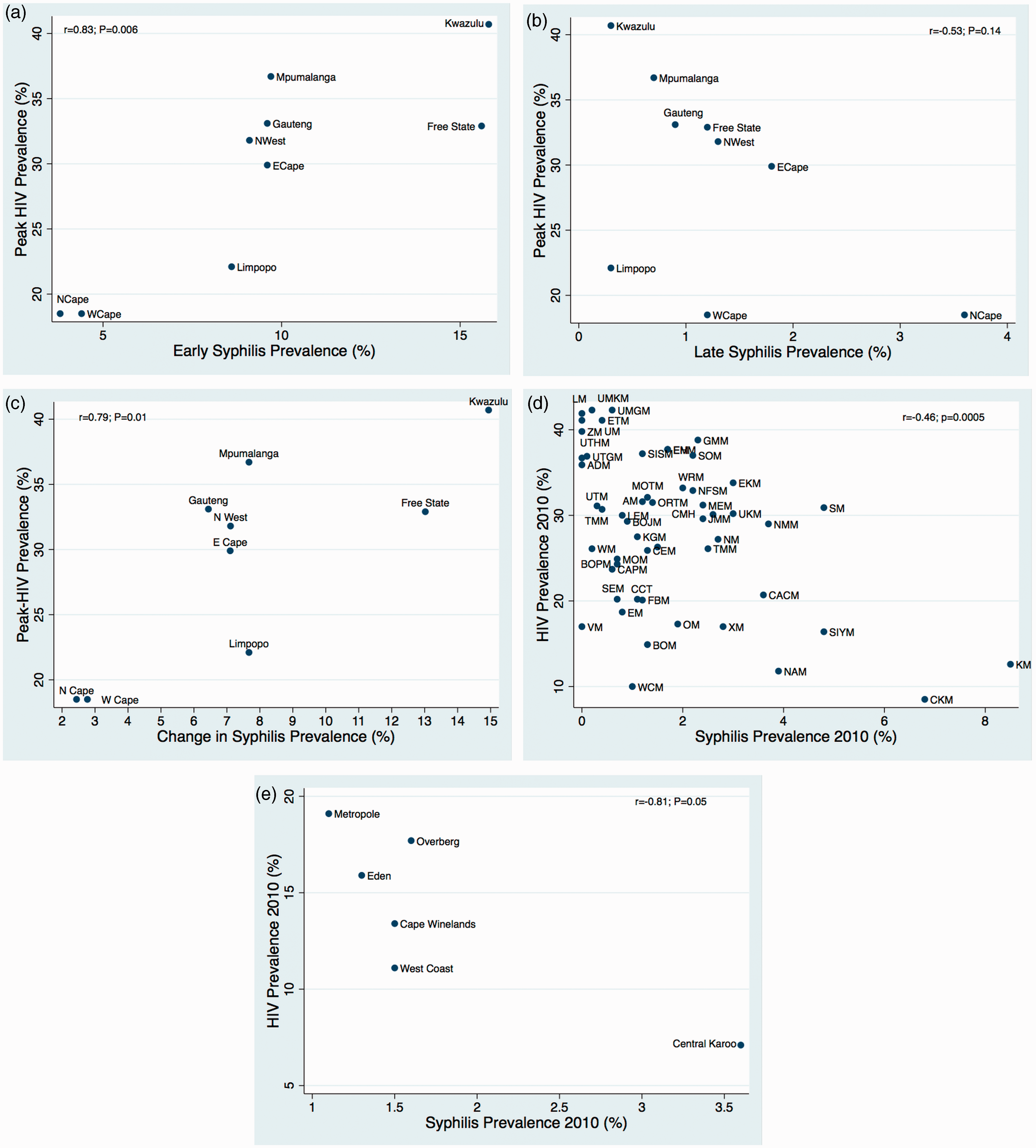
The epidemic curve of syphilis in South Africa exhibited a rapid drop after 1998 (Figure 1). There was a positive association between the syphilis prevalence early in the HIV epidemic and the peak HIV prevalence at the provincial level (r = 0.83; p = 0.006; Figure 2(a)). Later in the HIV epidemic the relationship switched to a negative association. The relationship between peak HIV and nadir syphilis prevalence was also negative, but at a provincial level was not significant (r = −0.53; p = 0.14; Figure 2(b)). In contrast, at a district council level there was a statistically significant negative association between HIV prevalence and syphilis prevalence late in the epidemic (r = −0.46; p = 0.0005; Figure 2(d)). The same relationship was found at a district council level in the analysis of the data from the 2010 Western Cape antenatal survey (r =−0.81; p = 0.05; Figure 2(e)). At a provincial level there was a positive association between peak HIV prevalence and the change in syphilis prevalence (r = 0.79; p = 0.01; Figure 2(c)).
The prevalence estimates of syphilis among women attending antenatal care (blue dashed line) and HIV (in 15- to 49-year-olds – red solid line) between 1990 and 2011 in South Africa (syphilis prevalence from national antenatal surveys and HIV prevalence from UNAIDS estimates). (a) Provincial level association between peak HIV prevalence and syphilis prevalence early in the HIV epidemic (pre-HIV peak). (b) Provincial level association between peak HIV prevalence and syphilis prevalence late in the HIV epidemic (post-peak HIV). (c) Provincial level association between peak HIV prevalence and change in syphilis prevalence, district council level association between HIV and syphilis prevalence in 2010 in the whole country (d) and in the Western Cape Province (e). (The data are from the annual South African antenatal HIV and syphilis surveys).
Change in incidence of STI symptoms
At a provincial level, the incidence of MUD and MGU in 1998 (the period leading up to the peak HIV prevalence) were both positively correlated with peak HIV prevalence at a provincial level (r = 0.66, p = 0.052; r = 0.79, p = 0.011, respectively; Figure 3(a) and (b)). Using 2003 data, these relationships switched to a negative association at a provincial level (r = −0.73, p = 0.130; r = −0.54, p = 0.027, respectively; Figure 3(c) and (d)). At a provincial level there was also a positive association between peak HIV prevalence and the change in MUD and MGU incidence (r = 0.73, p = 0.025; r = 0.86, p = 0.003; Figure 3(e) and (f)).
Provincial-level association between peak HIV prevalence and self-reported urethral discharge (a) and genital ulcers (b) in men in the prior 3 months in 1998 (earlier in the HIV epidemic). Provincial level association between peak HIV prevalence and self-reported urethral discharge (c) and genital ulcers (d) in men in the prior 3 months in 2003 (later in the HIV epidemic). Provincial level association between peak HIV prevalence and change in urethral discharge (e) and genital ulcer (f) incidence between 1998 and 2003 (STI symptom incidence rates from 1998 and 2003 Demographic and Health Surveys).
Discussion
It has long been known that there is a strong positive association between HIV and various bacterial STIs at an individual level in a wide variety of populations. 31 There is also evidence of this relationship at a population level. In a number of countries, groups based on ethnicity or sexual orientation, having higher syphilis prevalence estimates prior to the AIDS epidemic, went on to have higher rates of HIV.32,33 At a country level in Southern and Eastern Africa, national antenatal syphilis prevalence early in the HIV epidemic was positively correlated with peak HIV prevalence. 14 There is also evidence of associations between the prevalence estimates of various STIs including syphilis and HIV in 1999 at the level of United Nations world regions. 34
Therefore, our findings of the positive relationship between early syphilis/symptomatic STI prevalence and peak HIV prevalence at a provincial level are broadly commensurate with those in the literature. The strong association between HIV and syphilis at the individual level means that in the era preceding the availability of antiretroviral therapy (ART), a relatively high proportion of individuals with syphilis would have died of AIDS. When considered alongside changes in sexual networks due to high death rates, AIDS mortality could have been responsible for preventing a substantial portion of syphilis transmission and reducing overall prevalence.8,12 We hypothesized that this effect was strongest in areas where peak HIV prevalence was highest and attained most rapidly.
Our results show that, indeed, the relationship between HIV and the prevalence of syphilis, MUD and MGU changes from positive to negative. A number of other interpretations are, however, possible. First, regions most affected by HIV could have seen more rapid and profound changes towards safer sexual behaviour, a potential for which we could find little evidence in South Africa. 35 Second, there could be confounding by some unmeasured factor such as population levels of semi-immunity to Treponema pallidum and other STIs. 36 Third, our results could represent a chance finding. Fourth, the incidence rates for urethral discharge and genital ulcer were based on self-reported symptoms that are susceptible to a number of biases. We could find no evidence that provinces more affected by HIV responded with more rapid and widespread introduction of syndromic management of STIs. 9
This analysis suffers from a number of serious limitations. Despite being the best quality nationally representative time series syphilis prevalence data we could identify from the sub-Saharan region, the data from the South African antenatal surveys had numerous deficiencies. RPR testing was performed without any confirmatory testing by treponemal assays. As HIV is one of a number of causes of false positive RPR result, the HIV epidemic could have influenced RPR-based estimates of syphilis prevalence. 37 However, the fact that the syphilis prevalence dropped rather than rose as HIV prevalence increased suggests that this was unlikely to have played a large role. RPR results can also vary by a one dilution titre between different batches, adding a further potential misclassification bias. 38 There was a considerable flux of the South African provincial RPR-based syphilis prevalence estimates in the early years of the survey. These have been attributed to technical laboratory issues. 17 A further limitation was that we used peak HIV prevalence as a proxy for AIDS mortality. Future studies could evaluate if there is a relationship between AIDS mortality and syphilis prevalence declines in a time-linked fashion. Non-response rates for the 2003 DHS were relatively high and response rates did differ by province. Nonetheless, the timing and magnitude of the decline in MGU found in the analysis of the DHS data is broadly commensurate with that found from the syphilis prevalence data from the antenatal clinic data and other data suggesting a rapid decline of syphilis and other bacterial STIs around this time period (see Table 1).2–5 Furthermore, our results of a change in the direction of association between STI prevalence between pre- and post-peak HIV prevalence mirror those found at the country level in Southern and Eastern Africa. 14
While we did not investigate the relationship between HIV and syphilis at an individual level, other studies from South-Eastern Africa have demonstrated that there has been little change in this relationship despite the rapid declines of syphilis.31,39 This is an important point as it demonstrates the utility of combining population- and individual-level analyses in STI surveillance. Analyses of the relationship between HIV and syphilis in South-Eastern Africa have often (with a few notable exceptions 9 ) excluded population-level analyses. The report on the enhanced 2010 Western Cape antenatal survey, for example, noted, ‘…the anomalous finding that it [syphilis] is highest in the district with the lowest HIV prevalence and lowest in the district with the highest HIV prevalence. This suggests that the value of continuing the syphilis component of the antenatal survey [in order to gain insight into the HIV epidemic] is limited’. 17 The authors of the South African 2011 antenatal survey came to the same conclusion and as a result the latest antenatal survey did not test for syphilis. 40
There has been a resurgence in a range of bacterial STIs including syphilis, gonorrhoea and lymphogranuloma venereum in high-income countries following the widespread introduction of ART.10,41,42 This is thought to be due to a combination of factors including the reduced death rates of persons with bacterial STI and HIV co-infection43,44 and the behavioural disinhibition that has followed HIV being transformed into a chronic manageable disease. 45 Evidence of a similar effect is beginning to emerge in sub-Saharan Africa. 46
If the decline in bacterial STIs in South Africa and other countries with generalized HIV epidemics was determined to a significant extent by AIDS deaths, then an increase in the incidence of syphilis (and other STIs) may be a leading indicator that sexual networks are reconfiguring into their high-risk structures that predated the HIV epidemic and that continued surveillance is as important as ever. The data presented here suggest that AIDS mortality and associated changes in sexual behaviour may have contributed significantly to declines in STI prevalence in southern Africa, and hence that recent reductions in AIDS mortality could potentially lead to an increase in STI incidence. Ongoing individual and population-level surveillance of syphilis and other STIs in these countries would therefore seem a prudent policy.
Footnotes
Acknowledgements
The authors thank Dr David Pienaar for access to the Western Cape Syphilis and HIV Report 2010 and Dr Leigh Johnson for comments on an earlier draft of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.