
Abstract
Men who have sex with men experience disproportionate rates of HIV acquisition. Post-exposure prophylaxis following unprotected sexual exposure reduces HIV transmission. Our aim was to assess access to post-exposure prophylaxis for men who have sex with men in Irish emergency departments. We contacted all national 24-hour adult emergency departments describing two scenarios; a seronegative man who has sex with men receiving unprotected insertive anal intercourse from a seropositive partner and secondly a woman sustaining a needle-stick injury from an unknown source. We recorded and compared responses regarding post-exposure prophylaxis advice in each situation. High proportions of emergency departments offered post-exposure prophylaxis for both situations despite minimal evidence to support use in needle-stick injury. Men who have sex with men were less likely to be asked to attend emergency departments for post-exposure prophylaxis administration than a person experiencing needle-stick injury. Men who have sex with men were less likely to be offered baseline serological testing for blood borne infections. Men who have sex with men were as likely as needle-stick injury to receive advice from healthcare workers in emergency departments and consultation durations were similar. This study identifies a need to educate healthcare workers in emergency departments on appropriate use of post-exposure prophylaxis following sexual exposure for men who have sex with men. Health care workers must appreciate the importance of post-exposure prophylaxis presentations as opportunities for intervention and HIV screening.
Keywords
Introduction
HIV infection has increased in men who have sex with men (MSM) despite reductions in other risk groups.1–5 UNAIDS/WHO data from 2012 shows HIV prevalence in urban MSM 13 times that of the general population. 6 Irish Health Protection and Surveillance Centre (HPSC) data follow this trend. Since 2009, the majority of new HIV infections have been diagnosed in MSM, and MSM amount to 48.7% (166 of 341) of new HIV diagnoses in 2012. 7 Overall HIV prevalence in MSM ranges from 3.1 to 4.4%, 8 and infection is associated with individuals’ unawareness of HIV status, lower socio-economic grouping, ‘safe sex fatigue’, and increased recreational drug use.9–11 As MSM are at highest risk for HIV acquisition, they are a group in which preventative strategies may be targeted. Interventions to reduce onward transmission include increasing HIV testing in MSM, treatment as prevention strategies (TasP) and use of post-exposure prophylaxis (PEP) in defined episodes of high-risk sexual exposure (PEPSE).12,13 Observational studies of occupational HIV exposure demonstrated the efficacy of PEP to reduce HIV acquisition following exposure by 81%. 14 Guidelines for use now recommend PEP up to 72 hours after unprotected anal intercourse.8,15–17 PEPSE counselling is recommended during all MSM sexual health reviews. 18 PEPSE knowledge varies amongst risk groups. Just under half of HIV-positive MSM are aware of PEPSE indications compared to approximately one-third of HIV-negative MSM.19–21 However, MSM awareness is greater than other sexual orientations, including women and men who have sex with women. 22 Campaigns and interventions have succeeded to increase PEP awareness in MSM. 23
Injury from discarded needles in the community creates concern for transmission of HIV; however, HIV transmission via community needle-stick injuries (CNSI) has not been documented to date and should be considered extremely low risk, with non-occupational PEP (nPEP) not recommended for these exposures. nPEP was given in less than two-fifths of patients presenting with community-acquired sharps injuries (26.9–39.5%) and no new cases of HIV were documented at follow up.24–26 Despite anxiety surrounding these episodes, HIV transmission via this exposure has not been documented to date and should be considered extremely low risk.
Good access to PEPSE is a key factor in reduction of HIV acquisition in MSM. Recommendations state PEPSE should be available on a 24-hour basis, with urgent care providers and emergency departments (EDs) assuming responsibility for PEPSE administration out of normal working hours. 8 Evidence suggests a deficit of knowledge of PEP and its uses for non-occupational exposure in EDs. 27 We hypothesised that despite widespread availability of PEPSE throughout the healthcare system, MSM may experience disparate access to PEPSE in EDs as compared to other groups. We compared access to PEP for two scenarios. One with an indication for use – post-sexual exposure in MSM (PEPSE), 8 and the other with no PEP indication – a community-acquired sharps injury from a discarded needle in the (CNSI). 17
Methods
A group of Specialist Registrars working in Ireland’s largest HIV tertiary referral service sought to review PEP access in two defined situations. We created two scenarios based on risk exposures. Ethical clearance was requested but not required by the hospital Ethics Committee. Case 1 was an MSM with a recent episode of unprotected anal intercourse (UPAI) with a casual partner who subsequently disclosed their HIV-positive status. Case 1 was worried about acquiring HIV infection. This would be an indication for PEP use. Case 2 was a woman who received a penetrating sharps injury from a discarded needle in the community (CNSI). She was worried regarding infection from her exposure. PEP is not universally recommended in this case. These two cases were our ‘patients’.
The authors created a list of questions for each scenario (see Appendices 1 and 2). Each case’s questionnaire contained questions relating to exposure and descriptive characteristics. The patient’s main reason for calling was to seek advice for management following a presumed risk exposure. Calls were placed between the hours of 12.00 pm and 9.00 pm during the months of September and October 2012. The authors posed as patients and rang all 31 adult EDs in the Irish Health Services Executive.
The patient asked to be put through to a healthcare worker to advise whether they should attend the ED or follow up elsewhere. Respondents were not told the cases were for study purposes, as we wished to assess individual experience in accessing appropriate care, as opposed to individual knowledge of PEPSE.
Details from all phone calls were documented, including ED staff willingness to engage in discussion via telephone, level of assistance and knowledge of PEP. Standardised questions were used in each scenario (see Appendix 1) and answers were defined as containing (‘competent’) or lacking (‘non-competent’) information contained in an ideal response. Specific details included length of time dedicated to the caller by the ED, mean duration of calls (minutes), number of healthcare providers (HCP) involved per call, whether healthcare providers requested information from colleagues. Other details recorded included respondent’s knowledge and awareness of departmental PEP availability, if PEP would be available in each circumstance, whether the patient should present to ED for formal assessment and if baseline serological blood tests would be performed.
Data analysis was performed using IBM’s Statistical Product and Service Solutions (SPSS). Independent t-testing was used to compare means and Pearson Chi square test to compare proportions.
Results
Consultation details
The majority of telephone consultations were conducted by nursing staff. For case 1, (unprotected receptive anal sexual intercourse, UPSI) 31 telephone consultations were managed by 26 nurses and 4 medical doctors, and 1 call was dealt with by a medical administrative staff member. In case 2, (NSI, CNSI) 31 telephone consultations were managed by 30 nurses and 1 medical doctor.
Phone call details
Comparison of responses to each scenario.
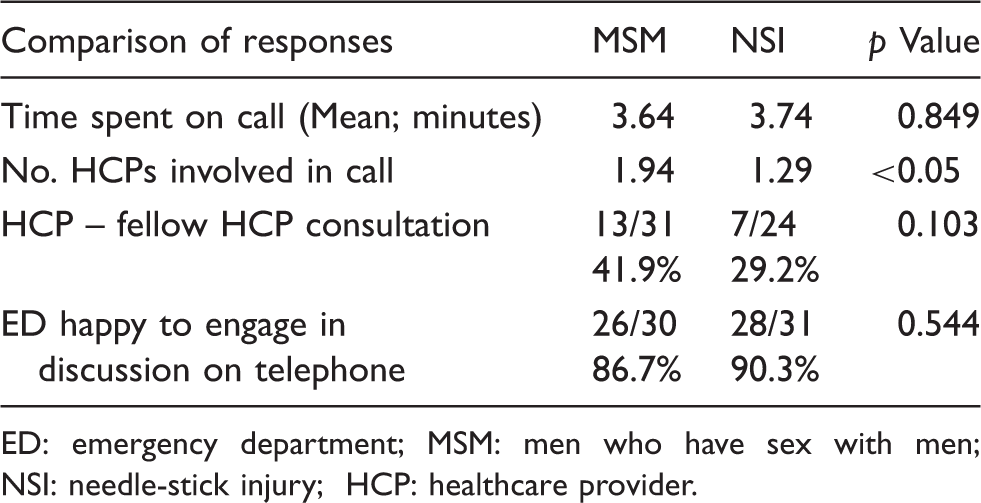
ED: emergency department; MSM: men who have sex with men; NSI: needle-stick injury; HCP: healthcare provider.
PEP knowledge
There was no difference in ED respondent’s knowledge of PEP and indications for use (classified as competent or non-competent). Of the 31 UPSI 14 (45.2%) and of the 30 CNSI 9 (30.0%) telephone call respondents were deemed as having a competent knowledge of PEP (p = 0.103). There was no difference in respondent’s knowledge of PEP availability within their ED; 8 of 23 (34.8%) UPSI respondents and 7 of 14 (50.0%) CNSI respondents knew where to access PEP medication (p = 0.146).
PEP administration
The proportion of ED respondents who stated PEP may be offered in either scenario did not differ – 7 of 24 (29.2%) UPSI respondents and 7 of 30 (23.3%) CNSI respondents (p = 0.944). There was a statistically significant difference in the number of EDs advising the patient to attend the department for further assessment and PEP. Only 7 of 31 (22.6%) UPSI consultations as compared to 15 of 31 (48.4%) NSI consultations were advised to attend the respondent’s ED following the telephone consultation (p = 0.034).
Management
Comparison of PEP knowledge for each scenario.
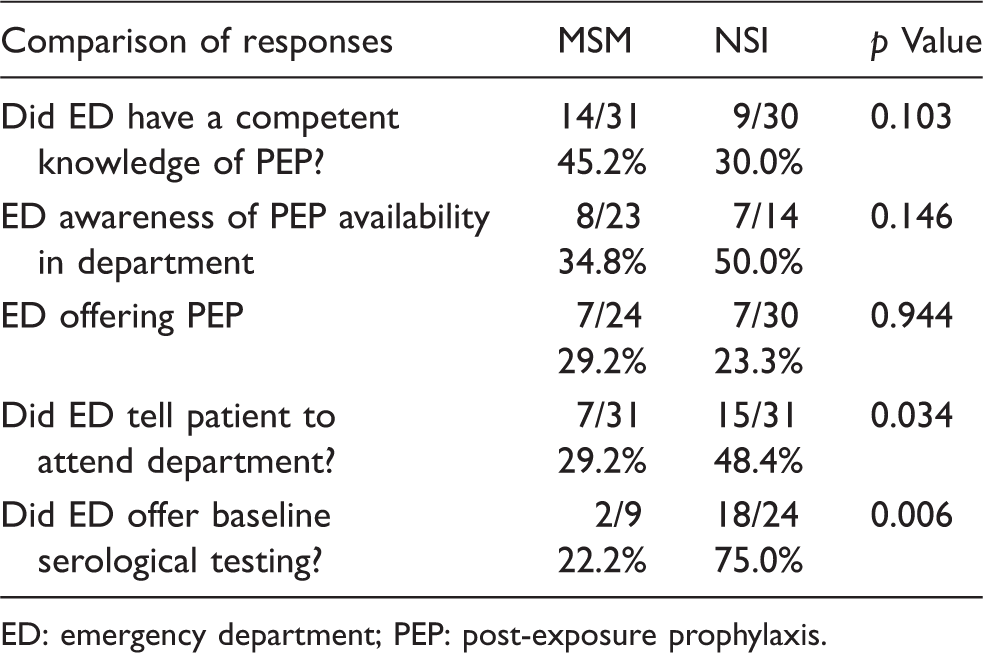
ED: emergency department; PEP: post-exposure prophylaxis.
Discussion
This is the first study to review access to PEPSE for MSM consulting EDs in the Republic of Ireland. MSM were as likely as CNSI to be advised regarding their situation via telephone (86.7% of UPSI vs. 90.3% of NSI) and received similar amounts of telephone consultation time from ED respondents. We demonstrated ED respondent tendency to offer PEP medication was similar in both situations (29.2% of MSM UPSI vs. 23.3% of CNSI), despite no evidence to support use in non-occupational CNSI. 8 MSM were less likely to be advised to attend ED to receive PEP compared to CNSI, and are less likely to access PEP for a situation in which there is strong evidence for use. A deficit in care and appropriate follow up was also identified, with lower numbers of respondents offered baseline serological testing for UPSI than CNSI, and only 51.6% (16/31) of UPSI exposures were advised to attend genitourinary medicine services. Considering the high prevalence of undiagnosed HIV in the MSM community, this represents a missed opportunity to actively screen for HIV in a high-risk population. HIV-positive MSM unaware of their status are 3.5 times more likely to transmit HIV than HIV-positive MSM who knew of their diagnosis. 28 ED knowledge of PEP and indications for use were similar in both situations. We hypothesise factors including departmental pressures including staff availability, unawareness of PEP indications and unfamiliarity with sexual history taking. Lanier et al. 29 demonstrate less than half of healthcare providers conduct sexual history taking with patients. 29 We identified a disparity in access to PEP for MSM, representing missed opportunities to utilise a targeted intervention known to reduce HIV transmission in MSM. Possible reasons include poor knowledge of PEP indication, availability and administration for UPSI. As the majority of ED respondents were nursing staff it may represent an opportunity for PEP-related education of frontline staff members. Reasons for higher tendencies to recommend PEP for CNSI may stem from management of occupational NSI, which is frequently undertaken by EDs. 30 As PEP is ‘intended for use in emergency medical settings where a patient first presents… including needlestick or other sharps injury, sexual exposure… where there is a risk of transmission of infection, in particular blood borne viruses,’ 18 MSM should have access to PEP within EDs. While non-occupational CNSI represent a concern for patients and healthcare workers, it must be appreciated that MSM are a much higher risk group for HIV transmission. Irish data show that of a total 3254 patients accessing care with HIV in 2010–2011, 2898 (89.1%) could identify a mode of transmission. Of these, 50% were heterosexual, 25% were MSM and 21% were intravenous drug users. None identified sharps injuries in the community as a method of transmission. 7 As previously discussed, MSM are the group most at risk for new HIV infection, and should be encouraged to seek PEP for high-risk sexual encounters. Rowley et al. 31 demonstrated the effectiveness of PEP use in MSM, with 31 patients accessing PEP remaining HIV negative at 6-month follow-up, 31 supporting use of PEP to reduce HIV transmission. If MSM are encouraged to seek PEP, access to medication is an essential component of this plan. Limitations of our study include a small sample size of hospitals (limited by the total number of hospitals within this jurisdiction), time pressure on individual department staff members, many of whom took calls whilst managing other responsibilities, leading to difficulty in completing the entire series of datasets per questionnaire. There were a variety of healthcare workers who offered advice. However, this study was not designed to assess individual healthcare personnel PEP knowledge but to assess the reality of an individual receiving the most appropriate advice in a defined at-risk situation. The authors also acknowledge that better study design may involve looking at whether PEP was offered or not for each situation, rather than comparison of two different situations.
In conclusion, this represents an inequality in access to a strongly indicated intervention for MSM exposed to HIV. Publication and dissemination of national PEP guidelines will aid appropriate use of PEP for frontline staff. This study also highlights missed opportunities for HIV screening in an at-risk population, where earlier detection could lead to better health outcomes for patients and help limit onward transmitted infection.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.