
Abstract
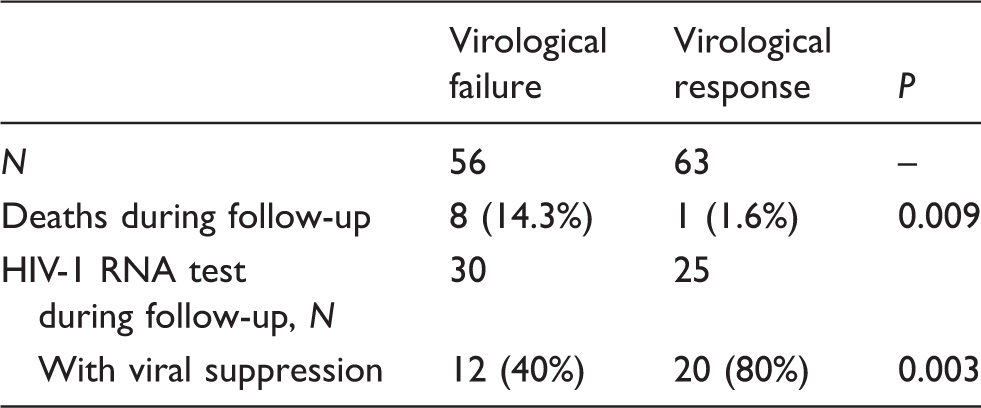
Virological monitoring of HIV-infected patients on antiretroviral treatment (ART) is rarely available in resource-limited settings and many patients experience unrecognized virological failure. We studied the long-term consequences of virological failure in rural Tanzania. Previously, virological efficacy was measured in a cohort treated with ART. In the present study, patients with virological failure (VF; HIV-RNA >400 copies/ml) were followed up and compared to those with virological response (VR; HIV-RNA <400 copies/ml) with regard to mortality, CD4 change and subsequent virological outcome. Fifty-six patients with VF had a median CD4 count of 358 cells/µl (interquartile range [IQR] 223–635) and a median HIV-RNA of 13,573 copies/ml (IQR 2326-129,736). Median CD4 count for those with VR was 499 cells/µl (IQR 290-636). During a median follow-up time of 39 months (IQR 18-42), 8 of 56 patients (14.3%) with VF died, compared to 1 of 63 patients (1.6%) with VR (p = 0.009). All registered deaths were HIV-related. Of 55 patients with subsequent HIV-RNA measurements, only 12 of 30 (40%) patients with VF achieved virological suppression, compared to 20 of 25 (80%) patients with VR (p = 0.003). Virological failure predicted death and subsequent virological failure in patients on ART in a resource-limited setting.
Keywords
Introduction
By the end of 2010, an estimated 34 million people were living with HIV/AIDS globally, 1 of whom 69% reside in sub-Saharan Africa. 2 The scaling up of antiretroviral treatment (ART) in resource-limited settings has led to a more than 100-fold increase in access to HIV treatment in less than a decade, and by 2011, an estimated 6.2 million people were receiving treatment. New infections and AIDS-related deaths are declining, also in high-burden countries. 2 Today, the estimated life expectancy of HIV-positive individuals approaches that of the general population, as long as treatment is initiated in an early stage of the disease and patients are adequately followed up. 3
The key to long-term benefit of ART is sustained suppression of viral replication. 4 In industrialized countries, HIV-positive patients on ART are monitored with HIV-RNA quantification and genotypic resistance testing. Because of high costs and the need for sophisticated laboratory equipment, however, these tests are rarely available in rural Africa. In resource-limited settings, the WHO recommends to monitor treatment and switch to second-line ART based on clinical criteria and CD4 T-cell counts. 5 However, several studies have shown that these criteria are insufficient to correctly identify virological failure.6,7 Hence, the recognition of virological failure might be significantly delayed in such settings, leaving the patients on a failing ART regimen for months or years. The clinical consequences of this are not well described.
In order to elucidate the long-term consequences of virological failure in resource-limited settings, we studied a cohort of HIV-infected individuals treated with ART in rural Tanzania. Clinical, immunological and virological outcomes in patients with previous virological failure were compared to patients with previous virological suppression. The results of the study could inform clinicians and policy makers about the need for viral load testing in similar settings.
Methods
Study setting
Tanzania has a population of nearly 47 million and the adult prevalence (15–49 years) of HIV was estimated in 2008 to be 5.7%. Access to ART has increased dramatically over the past decade, with support from international donor agencies. By December 2010, nearly 400,000 people were receiving ART. 8
Haydom Lutheran Hospital (HLH) is located in a rural area in northern Tanzania. ART has been offered since 2003 in accordance with the WHO guidelines.5,9 First-line treatment was stavudine or zidovudine, combined with lamivudine, plus either nevirapine or efavirenz. From December 2006, second-line treatment became available: lopinavir/ritonavir, in combination with at least two of the following (based on resistance results): didanosine, abacavir, tenofovir, zidovudine or lamivudine. Patients were monitored with regular CD4 T-cell counts, but HIV-RNA testing was not available except for research purposes.
Study design
A cohort study of patients consecutively starting ART was established in 2003. In a previous survey, 236 patients treated with ART for at least 6 months underwent viral load testing between 2007 and 201010,11 (Figure 1). Based on these results, a number of patients with treatment failure switched to second-line ART.
Timeline: chronological presentation of the study, illustrating the follow-up time.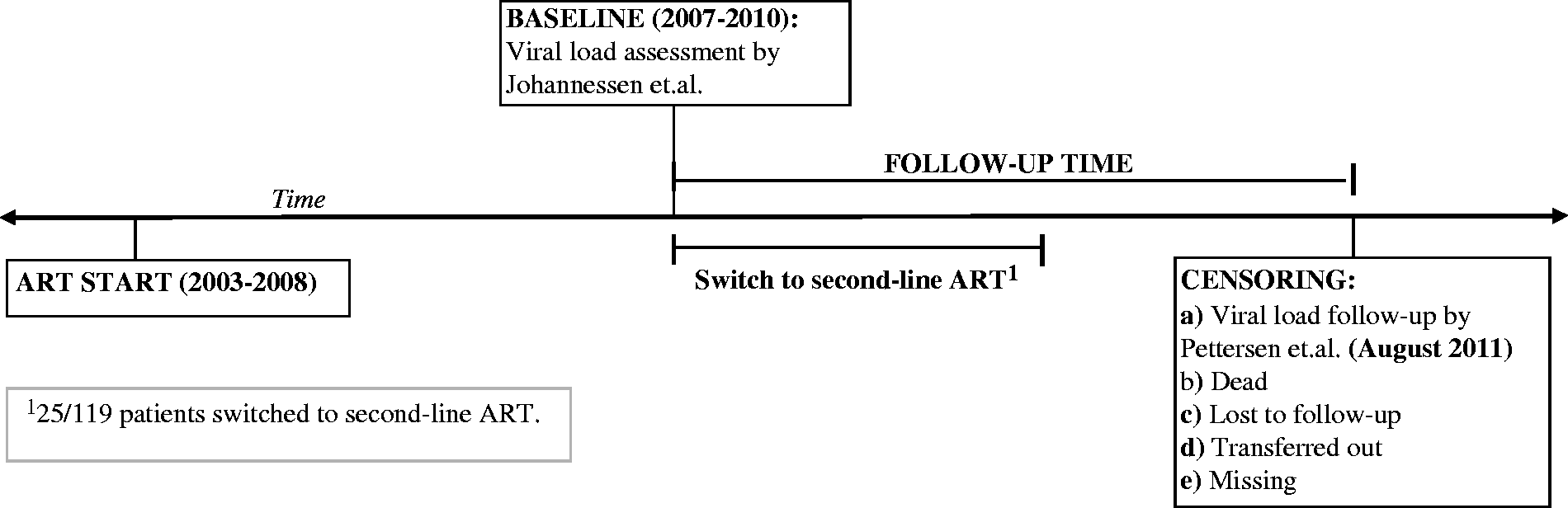
Fifty-six patients (children and adults) from the past virological efficacy survey had virological failure (VF; HIV-RNA >400 copies/ml) and were included in our study (Figure 2). For each patient with virological failure, another patient with virological response (VR) was selected by choosing the patient with the closest hospital ID number who had HIV-RNA < 400 copies/ml. The two groups ended up uneven because some patients with presumed VF were excluded post hoc (due to misclassification or unconfirmed treatment failure). Baseline was defined as the date when VF or VR was first confirmed.
Study profile: the dashed line marks inclusion in the study.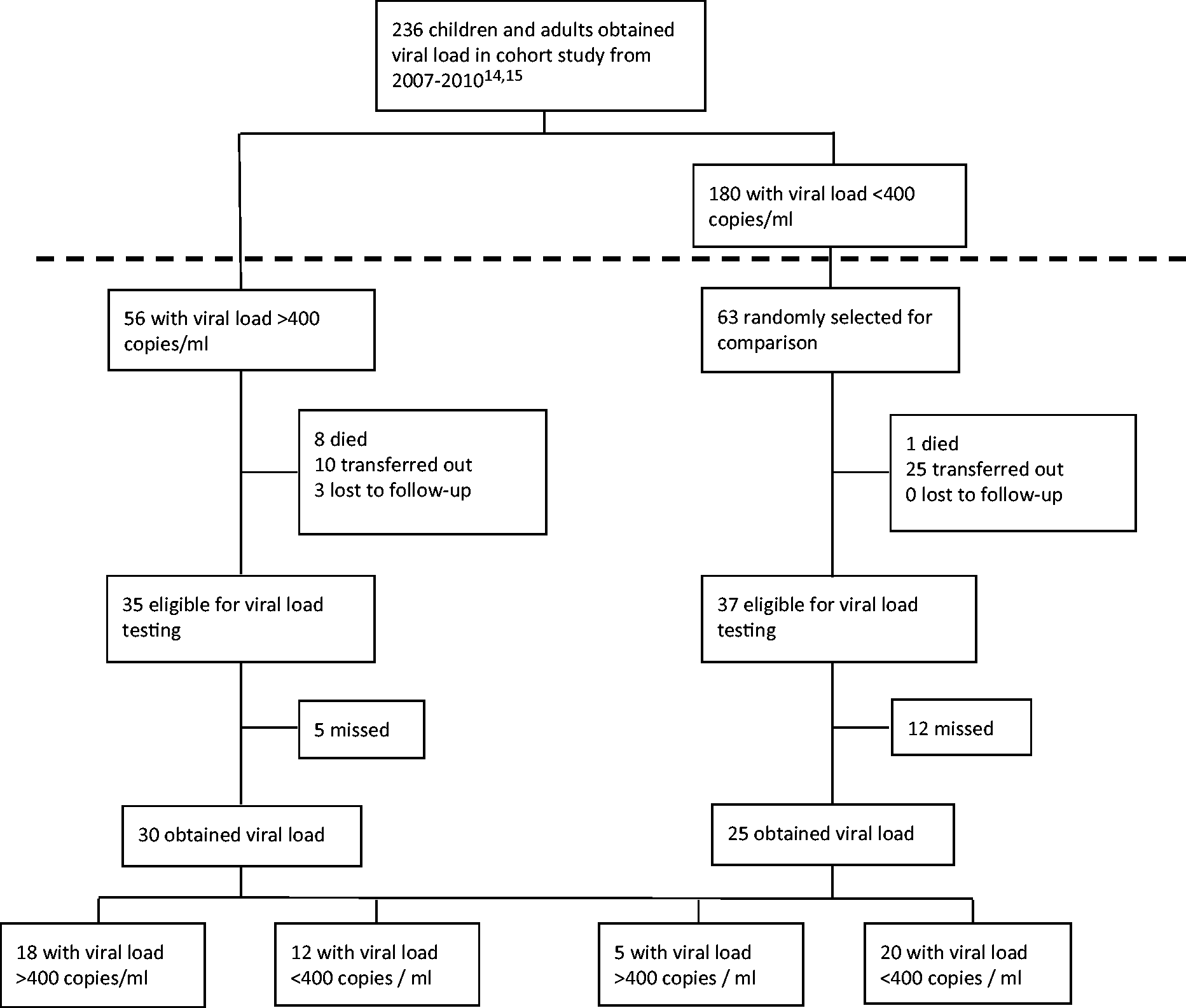
All patients were followed up until August 2011. Blood samples for viral load testing were collected in July and August 2011, when patients attended their monthly control. For those who died, were transferred out, lost to follow-up or missing, the follow-up time was right-censored at the date of the last known contact with the clinic (Figure 1). Demographic, clinical (death) and immunological (CD4 T-cell counts) data were collected from medical charts at the clinic. Death during the follow-up time was ascertained by home-visitors.
All data were typed and stored anonymously in the study database. The National Institute for Medical Research in Tanzania and the Regional Committee for Medical Research Ethics in Norway granted ethical approval, and all patients gave written consent to participate in the study.
Laboratory methods
Haematology and CD4 T-cell counts were measured at Haydom Lutheran Hospital using the Sysmex KX-21 Haematology Analyzer (Sysmex Corp., Kobe, Japan) and FACSCount flow cytometer (Becton Dickinson, San Jose, CA, USA), respectively. HIV-RNA analyses were performed at Muhimbili National Hospital, Dar Es Salaam, Tanzania, using either the Cobas TaqMan 48 Analyzer (Roche Diagnostics, Branchburg, New Jersey, USA), or the Cobas Amplicor HIV-1 Monitor v1.5 (Roche Diagnostics). Due to logistical constraints, a subset of the HIV-RNA analyses from 2011 were performed at Oslo University Hospital, using the Cobas TaqMan 48 Analyzer (Roche Diagnostics). Lower limit of detection ranged from 20 to 400 copies/ml depending on the assay; hence, a cut-off at 400 copies/ml was used to define virological failure.
Resistance data were analyzed at Oslo University Hospital, Norway, using the ViroSeq HIV-1 Genotyping System (Abbott Molecular, De Plains, IL, USA). All specimens with viral load >1000 copies/ml were tested. Only drug resistance mutations listed in the Spring 2008 update from the International AIDS Society were considered. 12 Resistance profiles to antiretroviral drugs were interpreted according to the Stanford University HIV Drug Resistance Database. 13
Plasma samples for virological analyses were centrifuged within 1 h of venipuncture, and frozen at −20°C. The samples were transported at ambient temperature for less than 20 h to the reference laboratories, in accordance with the manufacturer’s instructions.
Statistical methods
Mann–Whitney U test was used for comparison of continuous data throughout, since some of the data were not normally distributed. Continuous data were presented as median values and corresponding interquartile range (IQR). Categorical data were summarized using proportion.
The main three endpoints of interest in this study were death, subsequent virological failure and immunological progression. CD4 cell counts were plotted every six months, using the nearest measurement (±3 months). Difference in clinical and virological outcome was analysed using Chi-squared test or Fisher’s exact test as appropriate. Risk of mortality was calculated with logistical regression. Differences in progression of CD4 T-cell count between the groups were analysed with Mann–Whitney U test.
SPSS version 19.0 (SPSS Inc., Chicago, IL, USA) was used for all the analyses. All tests were two-sided and the level of significance was set at p < 0.05.
Results
Population characteristics
Patient characteristics at the time of virological testing.
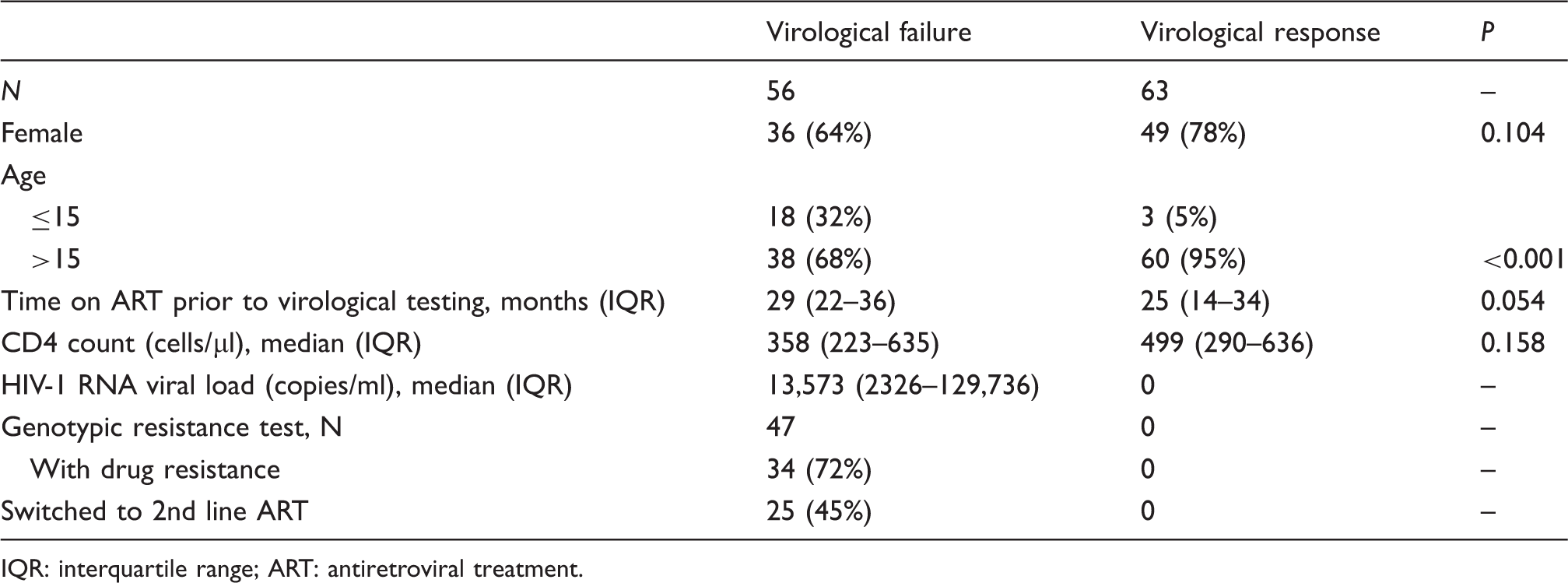
IQR: interquartile range; ART: antiretroviral treatment.
Time on ART before first viral load testing was 29 months for the VF group (IQR 22–36) and 25 months for the VR group (IQR 14–34). Median follow-up time after baseline was 28 months for the VF group (IQR 18–42) and 40 months for the VR group (IQR 18–44). Twenty-five of the 56 patients with VF (45%) switched to second-line treatment after recognition of virological failure. None of the patients in the VR group changed to second-line ART. Median time from viral load testing to treatment switch was seven months (IQR 4–11). Reasons for late switching or not switching included delayed reporting of laboratory results, patient’s refusal and clinician’s discretion. All patients switched to a regimen based on a boosted protease inhibitor (lopinavir/ritonavir).
Clinical outcome
During the follow-up time, nine patients died (7.6%), three were lost to follow-up for more than 12 months (2.5%) and 35 were transferred to other clinics (29.4%). Seventeen patients (14.3%) still in care did not attend during collection of blood samples. The study profile is presented in Figure 2.
Clinical and virological outcome during follow-up.
Median follow-up time from virological testing to death was 12 months (range 8–23). Three of those who died in the VF group had changed to a second-line ART regimen after detection of virological failure. The registered causes of death were all related to HIV/AIDS: diarrhoea/enteritis (n = 3), renal failure (n = 1), pulmonary tuberculosis (n = 1), tuberculous meningitis (n = 1), cytomegalovirus infection (n = 1) and cerebral toxoplasmosis (n = 1). For one patient, the cause of death was missing.
Immunological outcome
Median CD4 T-cell count was lower in the VF group compared to the VR group every sixth month from baseline up to 3.5 years later. However, the difference did not reach statistical significance at baseline (p = 0.158), 1 year (p = 0.266), 1.5 years (p = 0.149) and 2 years (p = 0.133). After 2.5 years (p = 0.017), 3 years (p = 0.018) and 3.5 years (p = 0.036), the difference in median CD4 count was statistically significant.
Virological outcome
An additional HIV-RNA viral load was measured in the 55 patients who showed up for their routine check-up in July/August 2011; 30 with VF and 25 with VR. Most patients received first-line ART; however, 19 of the patients with virological failure received second-line treatment.
Virological failure at baseline predicted subsequent virological failure: 18 of 30 patients with previous failure (60.0%) had subsequent virological failure, compared to 5 of 25 with previous virological response (20.0%; p = 0.003; Figure 2).
In the VF group, 13 of the 18 patients (72.2%) with subsequent virological failure were receiving second-line ART at the time of the last HIV-RNA measurement. The switch to second-line ART was not randomized, but based on patients’ preferences and the clinician’s discretion; therefore, a comparison of first-line versus second-line ART would not be appropriate.
Resistance
Forty-seven patients in the VF group had isolates successfully sequenced at baseline, of whom 34 (72%) harboured resistance to first-line ART (Table 1). The most frequent mutations were M184V, conferring resistance to lamivudine and emtricitabine, and Y181C, G190A/S and K103N, conferring resistance to non-nucleoside reverse transcriptase inhibitors. Twenty-two (64.7%) of the patients with detected mutations switched to second-line treatment. Resistance at baseline did not predict death: 6 of 34 patients (17.6%) with baseline resistance died during follow-up, compared to 2 of 13 patients (15.4%) without baseline resistance (p = 1.00).
Discussion
In this study from rural Tanzania, virological failure of a first-line ART regimen predicted a poor long-term outcome. Among patients with virological failure, 14.3% died during the follow-up time, compared to only 1.6% of the virological responders. This demonstrates two important points: on one side, the excellent prognosis of HIV-infected patients in rural Africa if they achieve full viral suppression, which has also been demonstrated earlier. 14 But on the other side, it shows that patients with virological failure, most of whom are asymptomatic, might die prematurely in the absence of timely detection of treatment failure and prompt action to improve adherence and optimize treatment.
In settings without access to viral load monitoring, the WHO recommends to detect treatment failure by clinical (new or recurrent WHO stage 4 condition) or immunological (impaired CD4 cell response) criteria 15 ; however, recent studies have shown that these criteria have poor sensitivity and specificity in detecting true virological failure.16,17 Using the WHO criteria, the majority of patients with treatment failure will not be detected until they develop severe immunodeficiency or opportunistic disease, at which stage widespread resistance is likely. 18 Furthermore, many patients will be misclassified as treatment failures despite virological response, and hence risk unnecessary switch to complex and expensive second-line therapy. 7 This stresses the importance of improved access to viral load monitoring in resource-limited settings, which might also be cost-effective if generic assays are used. 19
There are several possible explanations for the negative long-term outcome after first-line failure in our study. Most importantly, a delayed switch from a failing ART regimen has been shown to increase mortality in previous studies.20,21 Interestingly, in our study, virological failure predicted both death and subsequent virological failure, despite the fact that many patients had already switched to second-line treatment. However, the treatment switch was delayed for a median of seven months due to various logistical constraints, which might have negatively affected the prognosis. This underlines the need for point-of-care viral load kits designed for use in rural, resource-limited settings, like our study site in Haydom.
Drug resistance was not associated with increased mortality in our study, contrary to previous reports from North America and China.22,23 However, in line with our results, Swindells and colleagues found no evidence of drug resistance being linked to adverse clinical outcome in a rigorously designed case-control study of patients with virological failure. 24 The authors of the latter study speculate that the continued residual activity of ART might prevent clinical deterioration despite resistance mutations. Hence, the underlying (presumed) poor adherence – rather than resistance per se – might be the most important explanation of the excess mortality in patients with virological failure.
Our study has some limitations. First, the sample size is small, which makes our results less robust, and our findings should be confirmed in larger centres. Second, there were more children in the VF group than in the VR group, and theoretically the poorer prognosis in the VF group could have been merely a marker of poorer prognosis in children. However, only one child died during follow-up, the remaining seven deaths in the VF group were adults, so this cannot explain the differences observed. Third, patients who failed to attend for viral load measurements might have biased the study. It is possible that this group represents patients with poor compliance and worse clinical outcome, and that the negative clinical and virological outcome might be underestimated. However, this would not affect our main conclusions. The main strength of our study was the long observation time in a rural setting.
In summary, our results indicate that virological failure predicts mortality and subsequent virological failure in patients on ART in a resource-limited setting. Only 1.6% of the virological responders died during follow-up, which confirms the excellent prognosis for HIV-infected patients who receive ART if viral suppression is achieved. On the other hand, the high mortality observed among patients who failed to achieve virological suppression underscores the need to identify virological failure at an earlier stage and intensify adherence counselling and monitoring of these patients, before they develop life-threatening complications. Access to viral load testing and better follow-up of patients with virological failure is warranted to improve survival in rural, resource-limited settings.
Footnotes
Author contributions
The first two authors contributed equally to this work.
Acknowledgements
We are grateful to the patients for participating in our study and to the health professionals at Haydom Lutheran Hospital. We acknowledge the laboratory technicians in Dar Es Salaam and Oslo for their excellent services.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the South-Eastern Norway Regional Health Authority (Helse Sør-Øst RHF) for support through research grants.