
Abstract
To explore the heterogeneity of CD4 responses following highly active antiretroviral therapy, the patterns of CD4 recovery of HIV-1-infected Chinese patients who have been on their first antiretroviral regimen for ≥5 years were analysed. The CD4 trajectories were traced, smoothed and differentiated into three defined profiles. Half (56.3%) were ‘satisfactory responders’, with CD4 gain of >100 cells/μL and a peak of >350 cells/μL, plateauing before the end of Year 5. Thirty-three (24.4%) were ‘continuing responders’ whose CD4 rise persisted at Year 4–5. The remaining 26 (19.3%) were ‘poor responders’. Presentation with AIDS before therapy was common not just among ‘poor’ but also paradoxically the ‘continuing’ responders. While a majority had responded well to antiretroviral therapy, older patients and those with AIDS diagnosis before initiation of therapy may never achieve a satisfactory level even with effective treatment. Categorization of HIV patients by their CD4 trajectory may support the prediction of immunological outcome over time, and ultimately inform treatment choices.
Introduction
CD4 T-cell count is a useful surrogate of immune function and an important marker for monitoring the progression of HIV disease. Studies have shown that immunodeficiency is associated not only with AIDS but also non-AIDS defining diseases. 1 Once highly active antiretroviral therapy (HAART) is initiated, CD4 cell count increases rapidly in the first few weeks, followed by a slower recovery contributed to by newly-produced T cells. 2 Low baseline CD4 count before HAART has been shown to be a strong predictor of mortality and AIDS. 3 Ineffective restoration of CD4 cells while on HAART is also associated with AIDS, non-AIDS disease 4 and mortality. 5 Factors influencing CD4 count after HAART include age,6–10 gender, 11 baseline CD4 count,5–10,12,13 HIV RNA level,6,14 virological response to HAART,6–8,12 duration of HIV infection9,12 and clinical AIDS prior to HAART. 13 While starting therapy at lower CD4 counts is undesirable, a large number of HIV-infected individuals in many countries only managed to commence HAART at a much lower baseline CD4 count, 15 thus jeopardizing the clinical outcome.
Currently, there is significant heterogeneity in research findings on the trajectory of CD4 counts following HAART. Some studies suggested that the count plateaus after 2–4 years,9,10,16 others showing a continued rise,8,9,16 while the overall pattern appears to vary with the degree of viral suppression,13,16,17 and either baseline or concurrent CD4 cell count.9,10,16,17 Delineation of the CD4 count trajectory is further complicated by the variation in HAART regimens. The heterogeneity of CD4 responses could be particularly relevant in the Chinese populations who have been shown to have lower CD4 counts in healthy individuals. 18 Through understanding the patterns of CD4 recovery, evaluation of specific effects of HAART regimens can become possible. In addition, patients can be classified into different response groups such that monitoring of each can be developed. Against this background, we set out to: firstly define and classify the CD4 trajectories since HAART initiation in a cohort of Chinese HIV patients and secondly explore factors which may be associated with the specific CD4 patterns.
Methods
Study population
Clinical data were collected from all HIV-1 infected, treatment-naive, Chinese patients receiving their first HAART regimen at the Integrated Treatment Centre (ITC) between 24 June 1997 and 31 December 2012. ITC serves as an outpatient clinic for about 60–70% of all HIV-positive patients under care in Hong Kong. The data retrieved included demographics, HIV status (HIV diagnosis date, transmission route and HIV-1 subtype), clinical status (diagnosis of AIDS defining illness, and date and cause of death, if appropriate) and therapy status (pre-HAART CD4 and HIV RNA measurements, first HAART regimen, its start and end date). CD4 count (cells/µL) and HIV RNA (copies/mL) were recorded regularly (3–4 times per year) for each patient by a central laboratory.
To evaluate the CD4 recovery patterns following effective treatment with HAART, cases were selected if they (a) were aged ≥16 at the time of diagnosis, (b) had more than three CD4 and plasma HIV RNA measurements, (c) had CD4 data at the beginning and month 60, (d) have been on first HAART regimen for ≥60 months, and (e) had achieved sustained HIV RNA suppression (≤500/mL) throughout the five years (without any AIDS-defining illness), though isolated blips (≤2000/mL) were allowed.
CD4 trajectories smoothing and classification
CD4 trajectories for enrolled patients were smoothed using a locally-weighted regression (Loess) by quadratic polynomial. 19 Each smoothed value was determined by the neighbouring data points within the defined span, weighted by the distance from the smoothed value, 20 with missing values estimated in Loess. Effective CD4 recovery was defined by a rise of >100/μL and an ultimate level of ≥350/μL. The trajectories were classified into mutually-exclusive patterns, the criteria of which were derived from literature based on clinical rationale. Sensitivity analyses on parameters were performed to support the definition.
Statistical analysis
The Loess smoothing was conducted using the R statistical environment. Clinical characteristics and outcome were compared between the three groups by odds ratio (OR) with 95% confidence interval (CI) and Mann–Whitney U test in IBM SPSS Statistics® 21. Missing values were excluded from corresponding analysis.
Ethical consideration
This was a retrospective cohort study, involving anonymised data already collected for clinical management, without the need for contacting patients. Institutional approval for access to the data was obtained from Department of Health in compliance with the Personal Data (Privacy) Ordinance. Approval of the Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee was obtained.
Results
Patient characteristics
Characteristics of recruited Chinese HIV patients (n = 135).
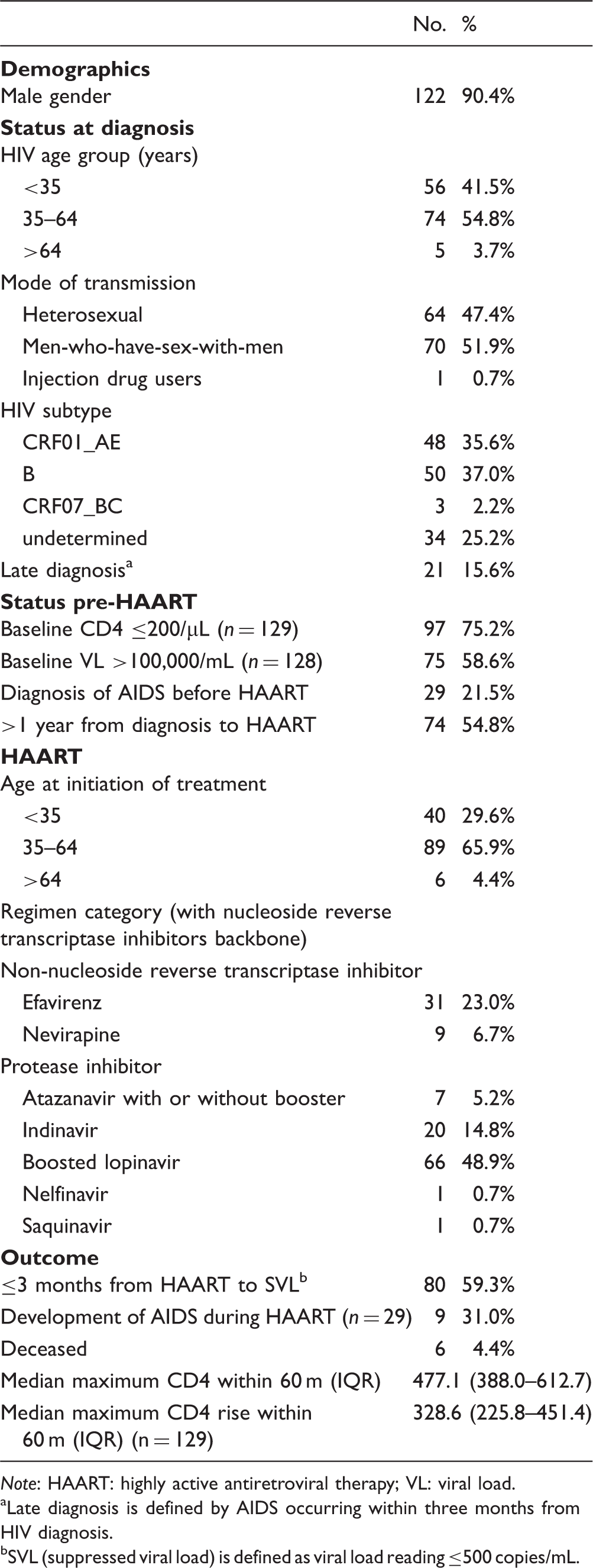
Note: HAART: highly active antiretroviral therapy; VL: viral load.
Late diagnosis is defined by AIDS occurring within three months from HIV diagnosis.
SVL (suppressed viral load) is defined as viral load reading ≤500 copies/mL.
CD4 responses and trajectories
The total follow-up time, as defined by the interval between first and last CD4 measurements while on one’s first regimen, was 10,951 months (average = 81 months per person). Slightly more than half (53.3%) had achieved a CD4 count >500/μL by Year 5, while about 80% attained the minimum threshold of 350/μL. Overall, 26 (19.3%) were classified as ‘poor responders’, 76 (56.3%) as ‘satisfactory responders’, and 33 (24.4%) as ‘continuing responders’ (Supplementary Figure 1).
‘Poor responders’ had characteristically flat CD4 trajectories from month 0 to 60. Rise of CD4 above baseline, if present, was ≤100/μL, and that the ultimate CD4 count was ≤350/μL. A few presented with sharp rises and falls but without any ultimate net gain of CD4 cells. For ‘satisfactory responders’, the final CD4 count was invariably ≥350/μL. There was a rise above baseline by >100/μL in the early period (Year 1–2) followed by a plateau by Year 3–5, such that the net gain of CD4 at Year 3 and 5 was <100/μL. Some (n = 63) had continuous rise throughout the five years, but the amplitude of increase between Year 3 and 5 was below 100/μL. The remaining ‘continuing responders’ gave a rising trend of CD4 throughout the five years. Apart from the increased CD4 count above baseline by >100/μL and a final value >350/μL, there was a continuing rise of >100/μL between Year 3 and 5 (Figure 1).
Selected examples of CD4 trajectory curves before and after smoothing.
Factors associated with CD4 patterns
Comparisons between trajectories for different response profiles (n = 135) – ‘satisfactory responders’: CD4 rise ≥100/μl and reaching plateau ≥350/μl before month 60; ‘poor responders’: flat CD4 trajectory throughout; ‘continuing responders’: satisfactory response with rising CD4 count at month 36–60.
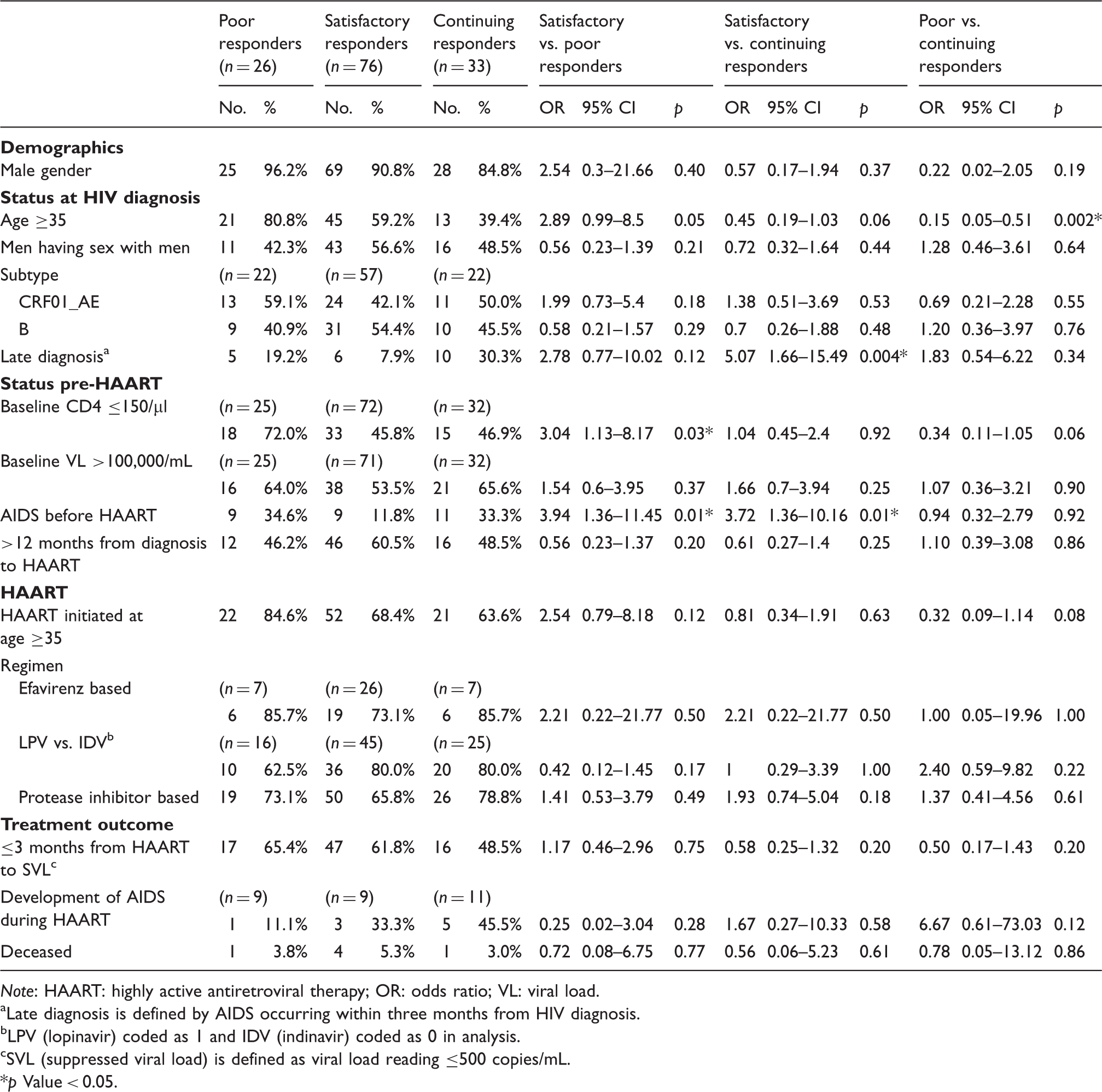
Note: HAART: highly active antiretroviral therapy; OR: odds ratio; VL: viral load.
Late diagnosis is defined by AIDS occurring within three months from HIV diagnosis.
LPV (lopinavir) coded as 1 and IDV (indinavir) coded as 0 in analysis.
SVL (suppressed viral load) is defined as viral load reading ≤500 copies/mL.
*p Value < 0.05.
From a different perspective, patients with late HIV diagnosis, as defined by AIDS occurring within three months from HIV diagnosis, were less likely to be ‘satisfactory responders’. Likewise, patients with AIDS diagnosis before HAART initiation were more likely to be either ‘poor responders’ (OR = 3.94) or ‘continuing responders’ (OR = 3.72). In this cohort, a majority of protease inhibitor (PI)-treated patients commenced indinavir or lopinavir. There was no difference between the two in their response category. As for treatment outcome, there was no significant difference in the time taken for achieving viral load suppression in the three CD4 response categories. In addition, there was no statistically significant difference in the change of CD4 in the first year between satisfactory and continuing responders (Mann–Whitney U = 1031, p = 0.14). It was not until year 3 that significant difference between the two response groups on CD4 change was observed (Mann–Whitney U = 910, p = 0.02). Multivariable logistic regression was performed by inputting variables that were significant in univariate analysis. AIDS before HAART remained the main predictor for distinguishing between ‘poor responder’ and ‘satisfactory responder’, while an age of ≥35 at HIV diagnosis was the distinguishing feature of both ‘poor responders’ and ‘continuing responders’ (results not shown).
Discussion
This is the first study conducted in an ethnic Chinese population for classifying HIV patients by their pattern of CD4 response following HAART. By including only patients who had been put on their first regimen, we removed the potential bias resulting from multiple changes in antiretroviral regimens. A CD4 cutoff of 350/μL has been chosen, as derived from the lower limit of the reference range in healthy Chinese populations (ranging between 292/μL and 415/μL),18,21 a level about 100/μL lower than that in Caucasians.22,23 Studies have shown that CD4 counts usually rise by >100/μL in the first year of treatment,9,10,13,16 a value that we adopted as a surrogate of minimum immunological responses. While a vast majority in our cohort had started HAART with low CD4 counts <200/μL, most went on to reach 350/μL within five years of treatment. The proportion of those achieving a target of >500/μL was however lower than Caucasian studies (51.7% vs. 59%),8,9 a discrepancy which may be related to a generally lower pre-treatment CD4 counts in the Asian population.17,24
Although restoration of immunity does occur consistently following HAART, the question remains as to why interpatient variability is so high as regards the rates and duration of CD4 change. We took a novel approach by dividing all patients into three distinct groups based on their pattern of response. Our results showed that the main predictors of a satisfactory response are a good baseline CD4 count and an absence of AIDS at initiation of HAART, which are in line with results elsewhere.5–10,12 Our own sensitivity analysis has shown that the numbers in each group was sufficient to generate reliable significance testing for comparing the CD4 patterns. Interestingly, both ‘continuing responders’ and ‘poor responders’ shared a similar association with a diagnosis of AIDS before treatment. Patients with continued increases in CD4 count beyond five years are likely those who started with a more impaired immune status but with good potential for immune recovery, while ‘poor responders’ had such severe immunological damage that functional recovery could not be achieved. This has been explained previously with reference to thymic involution occurring in the ageing population. 25 It is likely that the CD4 count of ‘continuing responders’ will eventually plateau once the T cells have reached their full potential. It is possible that the CD4 trajectory may vary with the HAART regimen, though this could not be confirmed in our study. A large meta-analysis reported that boosted PI therapy was significantly linked to greater rises in CD4 count than the other classes of drugs at 48 weeks; but no analysis was performed on individual regimen. 26 Another study reported no difference in on-treatment CD4 count between initial HAART regimens, 17 although there were no restrictions on changing regimen once started.
To conclude, our study has enabled us to define the CD4 trajectories of an exclusively Chinese HIV population over a prolonged time frame of five years. Compared to Caucasian populations, a smaller proportion in our cohort has ultimately reached a level of >500/μl. In our study, patients with the lowest CD4 counts at HAART initiation and older patients had a worse outcome and they may never achieve a satisfactory CD4 count on treatment. We acknowledge that there are inherent limitations in the study. Foremost, almost all patients had acquired HIV through sexual transmission and very few were injection drug users, which may limit the generalizability of our results to HIV populations in China or to other ethnic populations. Patients having less than three CD4 measurements were excluded. This was however unlikely to have led to any significant deviation from the main observations. Other factors that may influence the CD4 trajectories but not measured included CD8 T-lymphocyte count6,9 and hepatitis C coinfection status. 10 The impacts of different HAART regimens also need to be further explored. Nevertheless, by aiming to initiate HAART earlier before disease progression, the potential for immune recovery is increased and therefore, risk of mortality and morbidity could be reduced in these patients, which may apply to all ethnic groups.
Footnotes
Acknowledgements
The authors thank all patients and staff at the Integrated Treatment Centre for their participation and assistance in the maintenance of the database.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Direct Grant of the Medical Faculty, The Chinese University of Hong Kong (project code: 4054074) and the Health and Medical Research Fund (project reference no. CU-14-03-01), of Food and Health Bureau of the Hong Kong Special Administrative Region Government. Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong is acknowledged for supporting the conduct of the research.
Disclaimer
The opinions and assertions contained herein are private views of the authors and do not necessarily reflect those of the Centre for Health Protection, Hong Kong Department of Health. Initial exploration of related data has been presented at the Eleventh International Congress on Drug Therapy in HIV Infection 2012, Glasgow, UK.