
Abstract
This study examines the relationship between CD4 count and cervical cytological abnormality in HIV-positive women attending two district general hospital genitourinary medicine clinics in the East of England. It aims to determine whether the rate of cervical cytological abnormalities differs in HIV-positive women with CD4 count >350 cells/µl and those with CD4 count ≤350 cells/µl; and to compare the rates of abnormalities with that of the general population. We retrospectively reviewed data from a cross-sectional audit undertaken between December 2010 and December 2011 and analysed them using multivariable statistics. There was a significant association between recent CD4 count ≤350 cells/µl and cervical cytological abnormality (p < 0.001). A total of 6.3% of women with recent CD4 counts >350 cells/µl had abnormal cervical smear results, compared with 6.6% of the general population in the screening period 2010–11 and 7.2% of the general population in the screening period 2009–10. In our study population of women with recent CD4 counts >350 cells/µl, the proportions of mild, moderate and severe dysplasia were also similar to national figures. This raises important questions about the cost effectiveness of blanket annual screening for HIV-positive women.
Introduction
HIV infection and its related immunosuppression are associated with increased prevalence, incidence and progression of cervical squamous intraepithelial lesions/cervical intraepithelial neoplasia (SIL/CIN). 1 Cervical cancer is an AIDS-defining cancer. The use of highly active antiretroviral therapy (HAART) improves immune function with increased regression and decreased incidence of SIL;2–5 however, there are limited data on the level of immune function required to have a protective effect. Such data would be valuable for developing an effective cervical screening practice in the UK. In the absence of this information, the British HIV Association (BHIVA) and the NHS Cervical Screening Programme (NHSCSP) continue to recommend annual cervical cytology for all HIV-positive women.6,7
The current system for screening is far from perfect for HIV-positive women in the UK. Audits have shown that the uptake of yearly cervical screening in women with HIV is low.8,9 However, annual screening may be unnecessary for HIV-positive women with good immune status. Consequently, increasing the screening interval may improve the efficiency of the cervical screening programme.
Current BHIVA guidelines recommend starting antiretroviral therapy in patients with chronic infection when the CD4 count is ≤350 cells/µl. An American observational cohort study 10 found that HIV-negative women and HIV-positive women with CD4 counts greater than 500 cells/µl and negative test results for human papillomavirus (HPV) at baseline both had a similarly low cumulative incidence of SIL/CIN. Another study found that the frequency of low-grade lesions was greater in the HIV-positive group with CD4 cell count <350 cells/µl. 11 Furthermore, a prospective cohort study of 100 HIV-positive women demonstrated that women with abnormal cervical cytology were significantly more likely to have a lower mean CD4 count (372 cells/µl) than those with normal cervical cytology (549 cells/µl). 12 These data suggest that, whereas women with lower CD4 counts are significantly at risk of SIL/CIN, those with high CD4 counts are at no greater risk than HIV-negative women; as a result, there may be a case for the screening interval to be increased in HIV-positive women with high CD4 counts.
To our knowledge, there are no data from the UK examining the prevalence of cervical cytological abnormalities in HIV-positive women with CD4 >350 cells/µl and comparing it with the prevalence in the general population.
Methods
Study design
This was a cross-sectional analysis set in two district general hospital genitourinary medicine clinics in the East of England, of women attending between December 2010 and December 2011. Data were collected between December 2011 and March 2012 as part of an audit into uptake of cervical screening.
Participants
The last 100 HIV-positive women to attend each clinic were selected to make a total of 200. Eligibility criteria included age between 24 and 65, recent smear test (within one year) and attendance at one of the two clinics for their routine HIV care during the study period. One hundred and ninety-seven women were considered valid. Three were excluded as one had a hysterectomy and two had inadequate smear tests.
Variables
Exposure variables
Independent variables included in the analysis were age, ethnicity, recent CD4 count (defined as a routine CD4 count performed within six months of smear), previous CD4 count (measured one year before), previous abnormal smears, whether in receipt of HAART, duration of HAART, and HIV viral load as measured during a routine visit within six months of smear. Except where specified, exposure variables were measured at the time of their most recent smear test.
Outcome variables
The outcome variable was abnormal cervical cytology. In the study ‘abnormal cervical cytology result’ refers to borderline changes, mild dysplasia, moderate dysplasia, severe dysplasia and invasive carcinoma during the study period. This grouping was chosen to fit with the NHSCSP annual reporting of cervical screening statistics. When compared with the Bethesda system for the reporting of cervical cytological diagnoses, borderline changes refer to atypical squamous cells; mild dysplasia refers to low-grade SIL/histological classification CIN 1; and high-grade squamous intraepithelial lesion/histological classifications CIN 2-3 include moderate and severe dysplasia.
Data sources
Data were collected using case notes, departmental databases and the national database for cytology results (Open Exeter). Missing data were excluded in the statistical analysis.
Ethics approval
According to the policy activities that constitute research at Watford General Hospital, this work met criteria for operational improvement activities exempt from Ethics review as it was primarily intended to improve local care by auditing the uptake of yearly cervical screening in subgroups of HIV-positive women attending the clinics.
Statistical analysis
The association between the exposure variables and abnormal cervical cytology was investigated using univariate analysis. Variables with p < 0.2 were included in a multivariable logistic regression model. We tested the validity of the assumption in our model that the exposure effects of the two continuous variables age and duration of HAART are linear, by comparing with a more general model that included quadratic effects. 13 A likelihood ratio test found no significant evidence in favour of including such non-linear effects. SPSS version 20.0 was used for analysis. The level of significance was defined as p ≤ 0.05. Logistic regression models, independent T test, Chi-squared test or Fisher’s exact test was used as appropriate.
Results
Patient characteristics
Clinical and demographic characteristics of study patients grouped according to CD4 count.
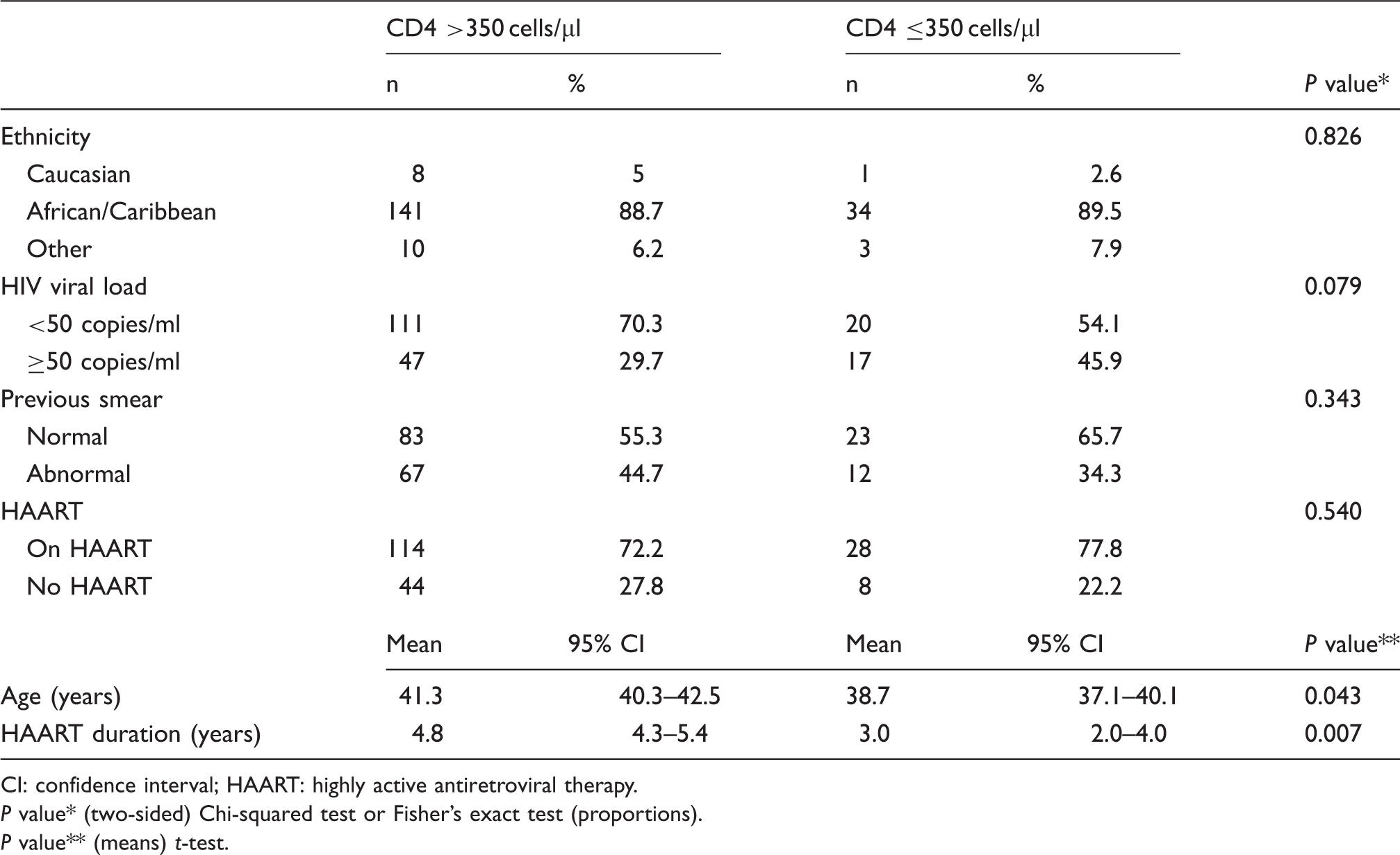
CI: confidence interval; HAART: highly active antiretroviral therapy.
P value* (two-sided) Chi-squared test or Fisher’s exact test (proportions).
P value** (means) t-test.
Cytology results
Cervical cytology results of study patients grouped according to CD4 count.
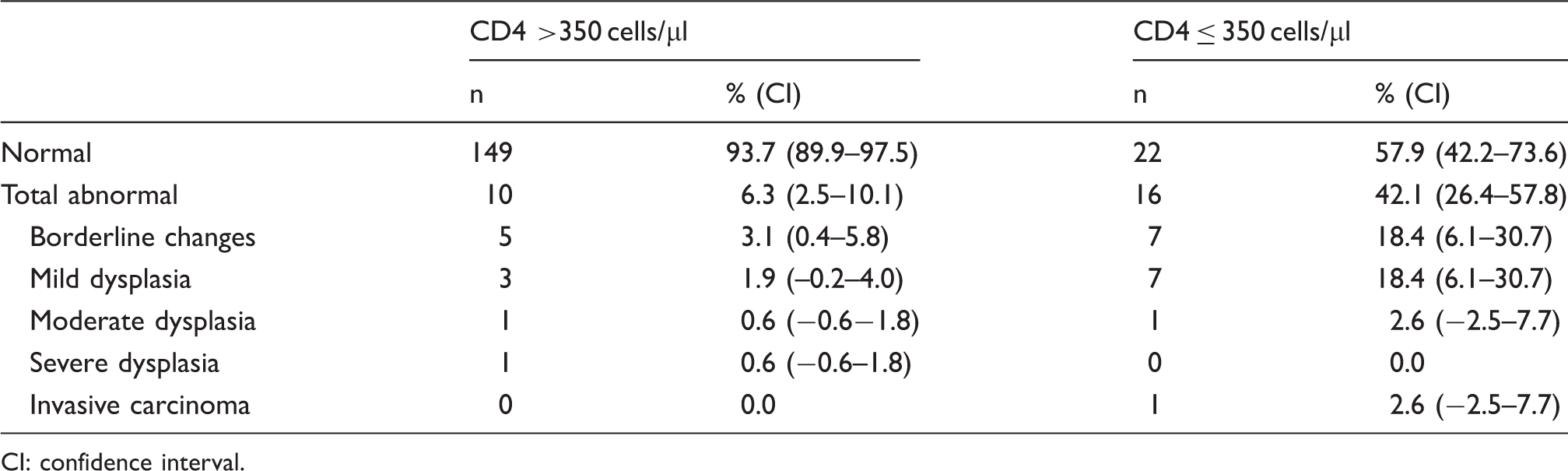
CI: confidence interval.
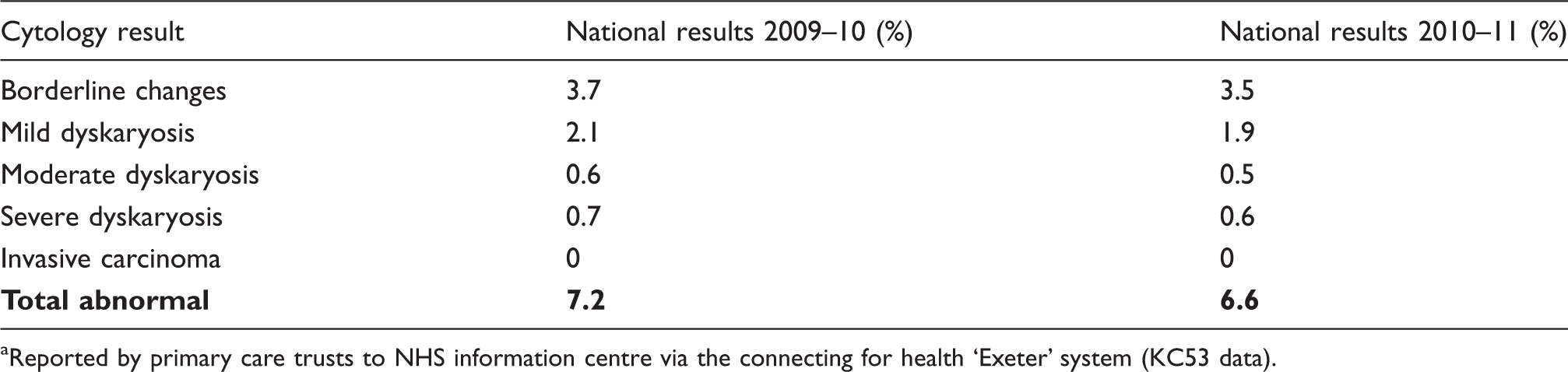
Reported by primary care trusts to NHS information centre via the connecting for health ‘Exeter’ system (KC53 data).
Multivariable analyses
Univariate and multivariable analysis. Clinical variables and their association with abnormal cervical cytology.
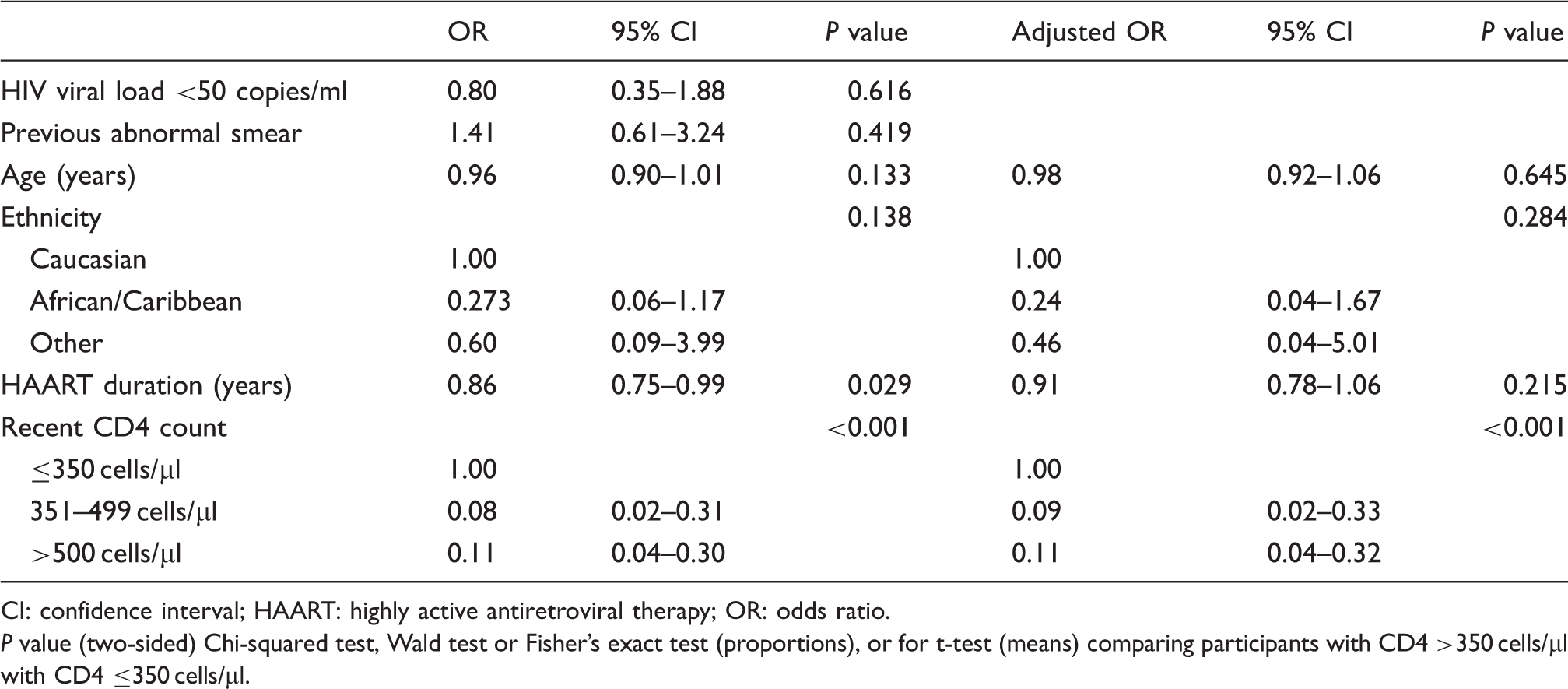
CI: confidence interval; HAART: highly active antiretroviral therapy; OR: odds ratio.
P value (two-sided) Chi-squared test, Wald test or Fisher’s exact test (proportions), or for t-test (means) comparing participants with CD4 >350 cells/µl with CD4 ≤350 cells/µl.
We also evaluated the association between previous CD4 counts and cervical cytology results using data that were available from 100 patients. Univariate analysis showed an association (OR 0.22; 95% CI 0.09–0.57; p = 0.002). However, when we included the recent CD4 count, HAART duration, age and ethnicity and performed a separate multivariable analysis, there was no significant association (OR 0.48; 95% CI 0.14–1.67; p = 0.247).
Discussion
The prevalence of cervical cytological abnormalities in women with recent CD4 counts >350 cells/µl in our study was similar to those reported for the general population by NHSCSP. Indeed, 93.7% of our study population had normal cervical smear results, compared with 93.5% in the general population in the screening period 2010–11 and 92.8% in 2009–10. Furthermore, in our study, women with CD4 count >350 cells/µl had similar proportions of mild, moderate and severe dysplasia to national figures. None of the women with CD4 count >350 cells/µl had invasive carcinoma. There was approximately a 90% reduction in the risk of cervical cytological abnormalities in women with a CD4 cell count of >350 cells/µl compared to those with CD4 count ≤350 cells/µl.
Our study found no significant difference in the CD4 counts of those with moderate-to-severe dysplasia and those with mild dysplasia. This is in contrast to an Italian study of 101 HIV-positive women where mean CD4 count in those with high-grade lesions was significantly lower (278 cells/µl) than in those patients with low-grade lesions (413 cells/µl). 15 However, in their population, there was a significantly higher prevalence of dysplasia (37%) than in our population. That study also showed an association between high viral loads and dysplasia. 15 Our study failed to show any association between HIV viral load and dysplasia. Possible explanations for the higher rate of dysplasias in women with lower CD4 counts may be reduced HPV clearance in that group, increased length of HIV infection and reduced access to care and prior long-term cervical screening.
Our findings must be considered in light of the study’s limitations. It was a retrospective study, which comes with limitations in obtaining all the required data. A major limitation is the small sample size, as reflected in the small size of the CD4 ≤350 cells/µl subgroup. We were able to get data regarding previous CD4 counts on patients recruited from only one of the sites. Some of the data were gleaned from notes, which may be subject to information bias. We used cytology, not colposcopy results, to define endpoints in our analysis: cytology is subject to false-negative results. Other risk factors for cervical cancer and possible confounding variables including smoking, socioeconomic status, length of HIV infection and previous HPV infection were not included. Although the statistical methods used in the analysis account for confounders and missing data as much as possible to reduce bias in our results, we were not able to adjust for population selection bias. The study population included only women who had recently attended for HIV-related care. In addition, we have compared the cervical cytology results of these women to those reported for the general population of England by NHSCSP. The NHSCSP data are not explicit as to whether the data include women living with HIV; however, this may be assumed as it states that all adequate screening tests reported by Primary Care Trusts in England are included. If the NHSCSP data does include women living with HIV then their results could skew the data; however, as the number of women living with HIV in England is relatively small their impact on the overall results would also be expected to be relatively small.
Despite these limitations, our findings are strengthened by the fact that this is one of the largest studies looking exclusively at the effect of these clinical variables on cytological abnormalities in the UK in the HAART era.
Our findings are important given the economic burden of blanket yearly screening. As patients are living longer with HIV, yearly screening for all women may prove less achievable and increasingly expensive. In our study only 30% of the women had consistently taken up yearly cervical screening since their diagnosis. A UK audit of another cohort of HIV-positive women found that of those who were eligible for screening, 27% had never had cervical cytology. Of those with a cytology record, 23% were overdue for their recall and, of those with negative cytology, only 54.9% were recommended to have repeat cytology in 12 months. 8 There are many possible factors that influence uptake, including failure to disclose their HIV status to general practitioners due to concerns about confidentiality. As a result, women may not be given accurate recall information following a normal smear. Another audit found that only 55.5% of clinics in a group of nine regional genitourinary clinics met the NHSCSP standards for performing annual smears. 9
An American study showed that adding HPV testing to cervical cytology smears obtained in the year of HIV diagnosis and modifying subsequent screening intervals based on the results was efficient and cost-effective and can be used to modify current recommendations for annual cervical cytology. 16 The data on the prevalence of HPV in HIV-infected women are limited. A prospective observational cohort study of HIV-positive women in the UK demonstrated a lower prevalence (23%) of high-risk HPV in HIV-infected women with a normal smear 17 ; in fact the prevalence was similar to that for HIV-negative individuals (25%). The current screening practice in the UK involves liquid-based cytology and HPV triage. This should help improve our knowledge about the prevalence of HPV in HIV-positive women with abnormal smears. The cytology results of the women in our study did not include an assessment of the presence of HPV infection.
Our findings suggest that in women with CD4 count >350 cells/µl, the national screening practices of HIV-negative women may be applicable. However, larger studies are needed to support the findings of this study. We propose that three-yearly cervical screening with HPV triage in accordance with the national cervical screening programme may be applicable in women with CD4 >350 cells/µl. In our study population, 42.1% of women with CD4 ≤350 cells/µl had cervical dysplasia. CD4 count ≤350 cells/µl should be considered an indication for more frequent screening. It would, however, remain important to target women with other risk factors for cervical cancer (high-risk HPV, smoking, etc.) and offer more frequent screening.
Footnotes
Acknowledgements
The authors would like to thank Mrs Toni Neil and Dr Mo Kawsar for assisting with data collection and Dr Helen Mullan for her helpful comments regarding this manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.