
Abstract
Antidepressant medication is well established for the treatment of depression but little is known about its effectiveness for HIV populations in sub-Saharan Africa. This study examined the effectiveness of antidepressant treatment and predictors of treatment response among depressed HIV patients in Uganda. Data were obtained from two open-label trials in which 184 HIV patients were diagnosed with depression and started on antidepressants. Data at treatment baseline and month 6 were compared to assess treatment response, and baseline predictors of response were assessed. A total of 154 completed month 6, of whom 122 (79%) had responded to treatment and were no longer depressed (Patient Health Questionnaire-9, score < 5). Bivariate analysis found that education, CD4 count, general health functioning, physical health, pain, quality of life and social support variables were associated with antidepressant treatment response; however, only secondary education and social support independently predicted treatment response in logistic multiple regression analysis. Baseline depression severity was not associated with treatment response. In conclusion, antidepressants are effective in treating both moderate and more severe depression among persons living with HIV in Uganda, and education [OR (95% CI) = 4.33 (1.33–14.11)] and social support [OR (95% CI) = 1.54 (1.03–2.30)] were most predictive of treatment response.
Introduction
As in other parts of the world, research reveals that about half of all persons living with HIV/AIDS (PLHA) in sub-Saharan Africa (SSA), including in Uganda, have elevated depressive symptoms,1–4 including 10–30% with clinical depression.2,5 It is well documented that depression has a negative impact on psychological well-being and quality of life,6,7 and evidence also supports its relationship to poor adherence to and outcomes of HIV treatment,8–11 engagement in sexual risk behaviour12,13 and difficulties in work performance and functioning.14,15
The wide-reaching harmful effects of depression highlight the need for effective clinical management of depression in PLHA, yet depression treatment and mental health services are largely absent from HIV care programmes in Uganda,16,17 as mental health resources are limited across much of SSA and other low- and middle-income countries.18–20 Consequently, depression is rarely diagnosed and often remains untreated.21,22 Several treatment modalities have been shown to be effective in treating depression 23 but antidepressants may be the most scalable and most easily task-shifted to primary care providers given the scarcity of trained mental health professionals in SSA. 24
The efficacy of antidepressants in treating depression among PLHA has been well documented in Western countries such as the US, 25 but we are not aware of any such studies or case studies in SSA. There is no reason to think that antidepressants would not be equally effective with PLHA in SSA as they are elsewhere but findings in the literature have been mixed regarding whether antidepressants are equally effective for mild-to-moderate depression as they are for more severe forms of the condition.26–28 This has important implications in Uganda where our studies have consistently shown that 70–80% of depressed PLHA have mild-to-moderate depressive severity. 15 As expected, the literature on predictors, pre-treatment variables that are associated with response to depression treatment of antidepressant response among PLHA in SSA is also non-existent. Identifying demographic, psychosocial and clinical predictors to treatment response can be important to identify risk and protective factors, guide treatment strategy, as well as inform treatment decisions, particularly, for understudied populations.17,29
This study (a) assessed the effectiveness of antidepressant medication in reducing depressive symptoms for PLHA in Uganda in an open label trial and (b) examined whether treatment response was differentially related to baseline depression severity as well as other patient demographic, psychosocial and physiological predictors.
Methods
Participants
Data from two studies of antidepressants for HIV patients were merged for this analysis. One was a longitudinal cohort study of patients starting antiretroviral therapy (ART) in which depression was assessed and those diagnosed with Major Depression Disorder (MDD) were treated with antidepressants. The other study enrolled experienced patients (regardless of whether or not they were on ART) who had been diagnosed with depression and were about to start antidepressant therapy.
In Study 1, patients about to start ART were enrolled in a longitudinal prospective cohort study designed to examine the effects of depression and antidepressant treatment on multiple health outcomes of ART. Patients were recruited from four HIV clinics operated by Mildmay Uganda—its headquarters clinic (Mildmay Centre) in Lweza on the outskirts of Kampala, and three clinics located in the rural or peri-urban towns of Mityana, Naggalama and Mukono. Primary eligibility criteria for initiation of ART were having a CD4 cell count ≤250 cells/mm3 or a diagnosis of WHO HIV disease stage III or IV (AIDS diagnosis). Patients who were diagnosed with MDD were followed up one month later and prescribed antidepressants if they still meet the criteria for MDD.
In Study 2, ART and non-ART patients from Mildmay Centre who had just been prescribed antidepressants for depression and were medically stable (defined as having no current acute opportunistic infections, having been in care at the clinic for at least six months, and not planning to start ART or within the first month of having started ART) were approached to participate between March and July of 2011, after which the MINI-International Neuropsychiatric Interview (MINI) was used to confirm a diagnosis of MDD and eligibility.
The patients at all of these clinics are generally from the lower socioeconomic strata, and care is provided free of charge. Psychiatric care is not provided at these clinics as part of usual care, with the exception of Mildmay Centre, where a psychiatric consultation clinic is held one half-day per week for patients who are referred by their primary care providers. Participants in both studies were required to provide written informed consent.
Procedures
Study 1 consecutively enrolled patients between September 2009 and February 2011 during assessment visits for ART eligibility. During this visit, Masters level psychologists assessed eligibility criteria for ART initiation and screened for depression using the Patient Health Questionnaire (PHQ-9), 30 and those who scored >9 or who were suspected to possibly be depressed were referred to the study psychiatrist for evaluation and confirmation of MDD diagnosis using the MINI. 31 Participants completed assessments at initiation of ART (baseline), and six and 12 months after the start of ART.
Study 2 recruited medically-stable patients who were initiating depression treatment with psychiatric medical officers at Mildmay Centre between March and July 2011. Patients who were just prescribed antidepressants by the psychiatric medical officers were referred to study psychologists, who confirmed medical stability and diagnosis of MDD based on the MINI. Assessments were administered at that initial assessment visit (baseline) and at month 6 follow-up.
In both studies, either fluoxetine (starting dose of 20 mg/day, with dosage increments of 20 mg as warranted) or imipramine (starting dose of 50 mg/day, increased to 75 mg after two weeks, followed by increments of 25 mg as warranted) was used to treat depression by psychiatric medical officers hired and trained by the study. Participants were compensated 10,000 Uganda Shillings (US$4) for their participation after each assessment. The protocols were approved by the Institutional Review Boards at RAND and Mildmay Uganda, as well as the Uganda National Council for Science and Technology.
Measures
The surveys administered at baseline and month 6 included measures of demographics, depression, health-related physical functioning and quality of life, and psychosocial functioning. All measures were translated into Luganda using standard translation and back-translation methods and were administered by trained Masters-level psychologists. Administration time for the survey was between 30 and 45 min.
Demographic and background characteristics included age, gender, education level (classified as primary school or less vs. at least some secondary education), relationship status (binary indicator of whether the participant was married or in a committed relationship vs. single, divorced or widowed), urban location (those attending the Kampala clinic) versus rural (attending one of the other three clinics) and current work status (binary indicator of engagement in food or income generating activity in the past seven days).
Depression
The MINI diagnostic interview depression module was used to diagnose for MDD and determine eligibility into the study. The MINI 32 is a relatively simple 15-min diagnostic tool designed for use with lay health providers and considered the gold standard diagnostic instrument in low and middle income countries (LMIC) settings, including Uganda. The translated Luganda version is a valid and practical approach to confirm depression diagnosis and to rule out bipolar disorder, psychosis and substance abuse. 33 The 9-item Patient Health Questionnaire (PHQ-9) 30 was used to measure depressive symptom severity over the past two weeks. Each of the nine items corresponds to the symptoms used to diagnose depression according to DSM-IV (Diagnostic and Statistical Manual of Mental Disorders, 4th edition) criteria. 34 Total scores range from 0 to 27 are categorised into the following severity levels of depression: none (0–4), mild (5–9), moderate (10–14), moderately severe (15–19) and severe (20+). 30 Although concerns have been raised regarding cultural variability of depression, studies on Ugandan conceptualisation of depression found that Ugandan symptom profile was consistent with the DSM and concluded that conventional depression measures, such as the PHQ-9, are adequate.1,17,35 Furthermore, the PHQ-9 has been used successfully with HIV-infected individuals in studies within SSA. 36
Response and adherence to antidepressant therapy
The PHQ-9 total score at month 6 was used to determine treatment response, with scores less than five representing full response, scores of 5–9 representing partial response and greater than nine being non-response. This method for determining antidepressant response has been used in other antidepressant research. 37 At Month 6, we assessed adherence to antidepressant therapy by asking respondents how many days did they miss taking a dose of their antidepressant medication in the past seven days, which we used to create a binary indicator of whether or not any doses were missed.
Physical health
CD4 count and WHO HIV disease stage (stages I to IV, with III and IV representing an AIDS diagnosis) were abstracted from the client’s medical chart. The Medical Outcomes Study HIV Health Survey (MOS-HIV) is a measure to assess health-related physical functioning and quality of life in people living with HIV, and it has been validated in Uganda. 13 The MOS-HIV contains the following 10 subscales: physical functioning (six items assessing respondent’s ability to engage in activities of daily life); general health (five items assessing respondent’s perception of their general health, resistance to illness and health outlook); role functioning (two items to assess impact of patients’ health on their ability to perform on the job, around the house or at school); pain (single item assessing bodily pain and its interference with normal activities); social functioning (single item assessing whether social activities have been limited by health); mental health (five items that assess symptoms of mental health problems); energy/fatigue (four items); health distress (four items that assess degree of discouragement due to health problems); cognitive functioning (four items measuring cognitive difficulties with reasoning, memory and attention); quality of life (single item) and health transition (single item measuring amount of change in physical or emotional health in the past four weeks). All subscale scores were transformed to a standardised score of 0–100 with higher scores representing better functioning.
Psychosocial well-being was assessed with measures of stigma, social support and alcohol use. Internalized HIV stigma was assessed with an 8-item scale developed by Kalichman et al. 38 Examples of items include ‘Being HIV-positive makes me feel damaged’ and ‘I am ashamed that I am HIV-positive’; response options range from one ‘disagree strongly’ to five ‘agree strongly’, and a mean item score is calculated. Higher scores represent greater stigma. Social support was assessed using a single item adapted from the AIDS Adult Clinical Trials Group (AACTG) assessment battery, 15 ‘I can count on my family and friends to give me the support I need’, and a 4-point rating scale from one ‘strongly disagree’ to four ‘strongly agree’; higher scores represent greater support. We assessed alcohol use by asking participants if they have used any alcohol in the past 30 days.
Data analysis
Descriptive statistics were used to examine sample descriptives and frequency distributions. Bivariate statistics (two-tailed independent t-tests and Chi square tests) were used to examine variables associated with response to antidepressants and study completion status. Logistic multiple regression analysis was used to identify independent predictors of treatment response. Separate regression analysis was performed for Month 6 study completers, and an intention-to-treat analysis where participants who were lost-to-follow-up at Month 6 (dropouts) were combined with antidepressant non-responders.
Results
Sample characteristics
In Study 1, 798 HIV patients starting ART were enrolled, of whom 79 were diagnosed with MDD and started on antidepressants. In Study 2, 105 clients on ART were diagnosed with MDD and agreed to start antidepressants. Hence, a total of 184 HIV patients initiating antidepressants were included in the analysis for this paper. The two samples differed on their baseline HIV health status, with sample 1 (CD4 = 128.8, SD = 83.8) generally being less healthy than sample 2 (CD4 count = 345.9, SD = 242.7), who had been stable on ART treatment for at least six months. We combined the two samples to examine the antidepressant effects across a wider range of HIV patients. Thus, all associated health related variables (CD4, physical functioning, pain, health transition and quality of life) are included in the analysis.
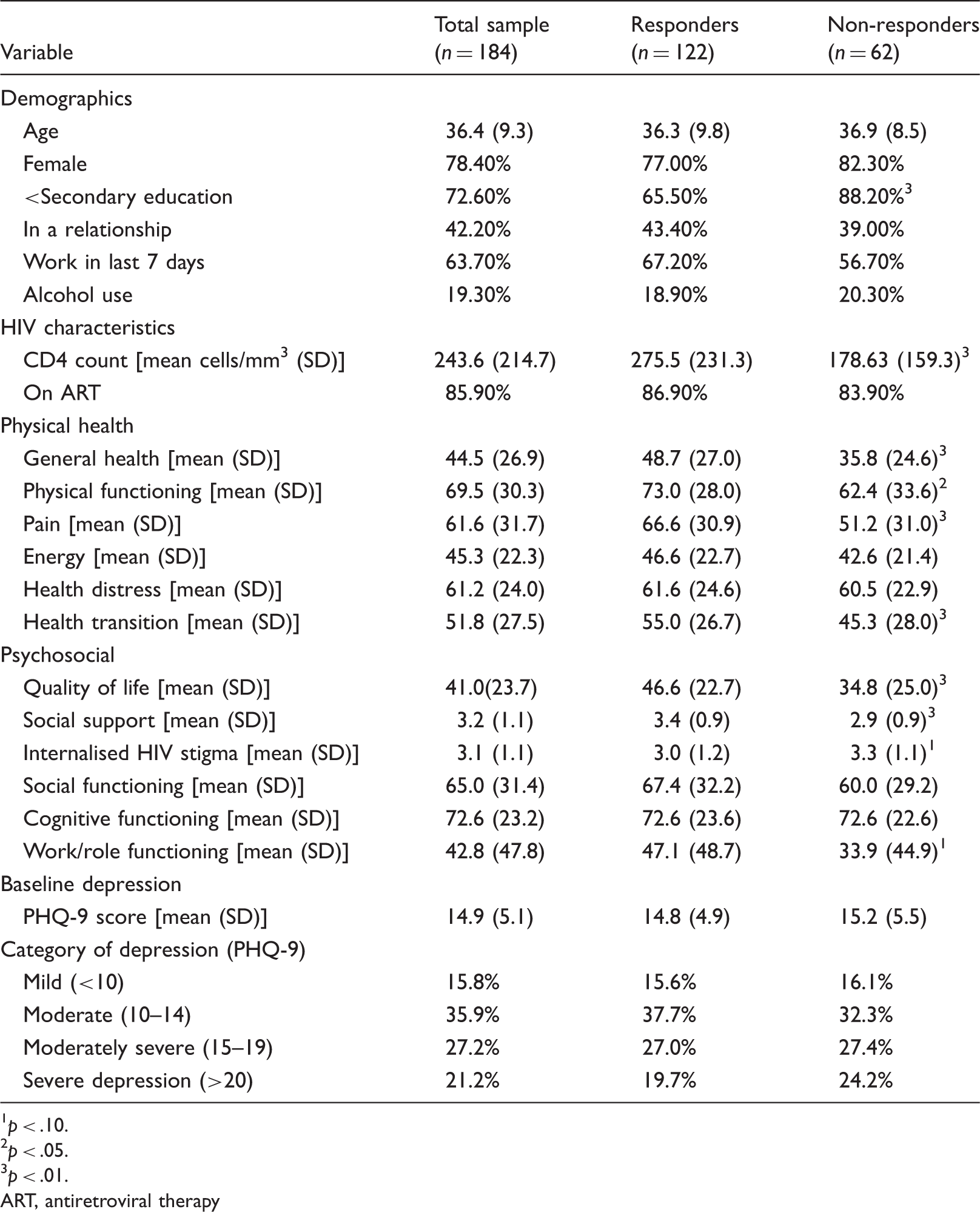
Sample characteristics of participants at baseline, reported by antidepressant responders versus non-responders.
p < .10.
p < .05.
p < .01.
ART, antiretroviral therapy
Baseline depression
The average PHQ-9 depression score for the sample was 14.9 (SD = 5.1); 16% had scores between 5 and 9, which signified mild depression (although these participants went on to meet criteria for MDD on the MINI), 36% scored between 10 and 14 (moderate depression), 27% scored between 15 and 19 (moderately severe depression) and 21% had severe depression (scores of 20 or greater).
Depression treatment and response
The majority (90%) of patients were treated with fluoxetine, and only one patient had their antidepressant switched (from fluoxetine to imipramine due to non-response) during the course of the study. Of the 154 clients who completed the Month 6 assessment, mean PHQ-9 was 2.6 (SD = 3.8), with 122 (79%) responding fully (PHQ scores<5), 22 (14%) responding partially and 10 (7%) not responding to antidepressant treatment. For analysis, we combined partial and non-responders resulting in 32 (21%) non-responders. Using an intention-to-treat approach in which the 30 non-completers are considered non-responders, the non-response rate increases to 34% (n = 62). Among the Month 6 completers, the proportion of respondents who reported any missed antidepressant doses in the past week did not differ significantly between responders and non-responders (22% vs. 29%; p = .50).
Comparison of responders and non-responders
Table 1 shows the bivariate comparison of means and proportions between responders and non-responders with regard to demographics, health-related functioning and quality of life, and psychosocial well-being at baseline. Education level was the only demographic variable that differed between the groups, with more non-responders having less than a secondary education (88% vs. 66%; p = .002), compared to responders. Responders also were healthier and had a higher mean CD4 count (276 vs. 179; p = .003) at baseline. Separate bivariate analyses for the two samples found that sample 1 had a higher percentage of responders than sample 2 who were less healthy (Sample 1: 87.2% responders vs. Sample 2: 66.7% responders). With regard to health-related quality of life, responders reported better health functioning than non-responders on several subscales including general health (48.7 vs. 35.8; p = .002), physical functioning (73.0 vs. 62.4; p = .040), pain (66.6 vs. 51.2; p = .002), quality of life (46.6 vs. 34.8; p = .013), health transition (55.0 vs. 45.3; p = .009) and marginally greater role functioning (47.1 vs. 33.9; p = .073). With regard to psychosocial well-being, responders reported significantly greater social support (3.4 vs. 2.9; p = .002) than non-responders. Responders and non-responders did not differ on continuous or categorical measures of depression severity at baseline, nor were there any site differences. This bivariate analysis was repeated using only data from study completers, the results of which revealed the same group differences but with several associations being marginally significant due to the smaller sample size (data not shown).
In a logistic multiple regression analysis to assess multivariate predictors of antidepressant response, all variables associated with response at the p < .10 level (secondary education, CD4, general health, quality of life, role functioning, social support), except for pain and physical functioning, were entered into the model as independent variables. We excluded pain and physical functioning in order to limit multicollinearity as these variables were highly correlated with each other and with perceived general health (correlation coefficients all >.60). The significant independent predictors of response to antidepressant therapy were having any secondary education [odds ratio (OR) (95% CI) = 4.33 (1.33 – 14.11)] and greater social support [OR (95% CI) = 1.54 (1.03 – 2.30)].
Discussion
This study may be the first published study to examine the effectiveness of antidepressants in treating depression among HIV-infected patients in SSA and demonstrated in an open label trial that antidepressants are also effective for this population in developing countries as they are in developed countries.39–41 Contrary to a recent meta-analytic study showing that antidepressant effect was minimal to non-existent compared to placebo for mild-to-moderate depression, 26 this study found that depression severity was not associated with response to antidepressant treatment, and that antidepressants were effective for milder forms of depression as well as more severe depression. This is particularly useful in Uganda, where a larger percentage of patients have milder forms of depression that are associated with similar impairments in work, social, health and psychological functioning, as those with more severe depression.42,43
Our 79% rate of remission appears to be consistent with 70% recovery rate in a landmark placebo-controlled antidepressant trial in India for non-HIV patients. 44 However, it is much higher than that found in STAR*D (28–33%), 45 the largest placebo-controlled antidepressant trial to date, which often yields lower response rates than open label trials. It may be that in both India and Uganda, the sample is also focused on a highly-stigmatised, chronically-ill patient population receiving services in an extremely under-resourced setting. Given that mental health care is rarely available in LMIC, all participants in our study were treatment naïve, as they have not been offered mental health care previously, which may make it more likely that they respond to treatment. Participants in medication trials in the US may likely have tried other treatments, therefore may likely include a higher percentage of treatment-resistant patients.
In terms of identifying patient factors that can be predictive factors, bivariate analyses found that positive response to treatment was significantly related to higher education, CD4 count, health functioning and social support. However, only education level and social support independently predicted antidepressant treatment response. Consistent with STAR*D, 46 education was found to have greater overall predictive power for antidepressant treatment response than depression symptom burden, comorbidities and even health functioning. Higher education can function as a protective factor because it is often associated with greater knowledge about health and health management for patients with chronic illnesses,47,48 suggesting that more-educated clients may have a greater understanding of depression and depression treatment, and thus more apt to adhere well and benefit from treatment. This would also support the value of psychoeducation about treatment and depression at the outset of therapy, which was not an emphasis of the treatment model provided in the study but should and could be integrated in antidepressant delivery.
The correlation of social support and depression treatment response highlights the critical role of social environment on mental health.49,50 Those who have more social support are more likely to have greater access to information, and thus greater knowledge about their illness and treatment, as well as greater emotional support to cope with HIV stigma. Our findings are consistent with other studies showing the buffering effects of social support related to HIV disease progression, 51 including slower decline in CD4 cells, 52 slower symptom onset51,53 and longer survival. The positive effect of social support for both depression and HIV/AIDS suggests that interventions should promote active coping behaviours that increase social support.
The strong efficacy of antidepressant therapy observed in this study together with other research showing the public health consequences of depression 54 provide further support for the need to integrate depression care into HIV services in developing regions such as SSA. 55 This evidence of antidepressant efficacy is timely in light of initiatives such as the Grand Challenges in Global Mental Health (GCGMH), 56 a cross-national initiative to promote mental health integration into priority platforms including primary care 16 and HIV. 55 A severe shortage in trained mental health professionals is a key barrier to provision of depression care in countries such as Uganda, 17 where there is approximately one psychiatrist for every one million citizens, but task-sharing, protocol-driven models of depression treatment implemented by primary care providers have been shown to be effective in other resource-constrained settings.21,57
The study has a number of limitations. Without random assignment and a placebo control group, internal validity is threatened. Our lack of intermediary measures of treatment response hampered our ability to provide a more finely-tuned assessment of response timing but the advantage of assessing response six months after treatment initiation is that such a response is likely to be more robust; a placebo-like response would likely have resulted in a relapse into depression by month 6. Combining two different samples may introduce some concerns regarding internal validity. However, combining data from participants who differed on their stage in ART treatment also provided a wider range of health functioning, and therefore a more accurate assessment of the relationship between HIV health factors and antidepressant treatment response than if these samples were analysed individually. Finally, we relied on patient self-report of symptoms to rate response rather than clinician-rated measures, which may have more accurately assessed symptom severity and treatment response.
Although there may be limits to generalisability given different contextual factors that may impact treatment response, emerging data from around the world are suggesting that depression treatments, including antidepressants, are effective across settings and may cross the cultural and contextual divide. However, predictors to treatment response may differ across settings and should be examined to explicate how context may influence treatment response. This is a noteworthy area of research to explore, given the limited studies on antidepressant efficacy in SSA.
In summary, these results suggest that antidepressants are effective for the broad range of depression severity among HIV patients on ART in SSA, and identification of patient predictors may improve the way depression treatment is delivered in HIV service settings in SSA. These findings suggest that interventions for HIV patients with depression should be comprehensive and include education about health and mental health, as well as promotion of health and mood management behaviours, particularly, focused on increasing social support.
Footnotes
Acknowledgements
We thank the providers and patients who made this study possible.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by a grant from the NIMH (Grant No. 1R01MH083568-01A2; PI: G. Wagner).
Research ethics
The protocols were approved by the Institutional Review Boards at RAND and Mildmay Uganda, as well as the Uganda National Council for Science and Technology.