
Abstract
This paper looks into the differences of sexual risk behaviours and prevention services among men who have sex with men and women and men who have sex with men only. The data from a cross-sectional survey of 159 men who have sex with men and women and 1186 men who have sex with men only in western China is analysed. It is found that men who have sex with men and women, with multiple anal sex partners, have higher rates of selling and buying sex than men who have sex with men only, but obtain less HIV-related knowledge from partners or HIV consulting and testing services. More efforts should be made to promote safer sexual behaviours and reduce the barriers for access to health services.
Keywords
Introduction
Among men who have sex with men (MSM), sex with women is a relatively common phenomenon. Previous studies estimated the occurrence of bisexual behaviour at about 26%–31% among MSM in China.1,2 Because of traditional social norms, homosexuality in China is highly stigmatised and results in MSM's high social pressures to conform to heterosexual standards. In order to fulfill family obligation and conceal sexual orientation, they may tend to marry and have children with women. Men having sex with men and women (MSMW) are more likely to engage in unprotected sex with female partners than male partners.3–6 A meta-analysis of HIV-risk behaviours conducted in China showed that only 23.3% of MSMW had reported consistently using condoms with their regular female partners. 1 ‘Tong-qi’, a Chinese term referring to wives who are married to MSM, are highly vulnerable to HIV infection due to their unprotected sexual contacts with their highly at-risk husbands. The HIV prevalence among Tong-qi increased from 0.18 per 1000 person-years in 2002 to 0.88 per 1000 person-years in 2010 in China. 7 Given the high rates of HIV infection and the low rates of condom use among MSM's female partners, it could be the case that bisexual men end up as a bridge that accelerates the transmission of HIV and other sexually transmitted infections (STIs).
Previous studies have documented that HIV prevalence was higher among MSMW (15.3%) than among MSM only (MSMO) (11.1%) 5 and MSMW had a 30% greater chance of being infected with HIV compared with MSM. 6 Evidence from research in America suggested that MSMW were less likely to use HIV prevention services and undergo HIV testing than MSMO, but few studies have been conducted that explore this issue in China. 8 Moreover, in intervention programmes, prevention efforts at the local level often recognise MSM as a matter of preference; and irrespective of whether they have sex with women or not, so a public health strategy may not distinguish MSMW from MSM.
To design more effective intervention programmes, we need to understand sexual risk behaviours, and the extent to which bisexual behaviour serves as a bridge for infection of the female population. This study investigated sexual behaviours and HIV-related services among MSMW and MSMO in three provinces of western China: Guangxi, Sichuan, and Chongqing. The aims of this paper were (1) to quantify the differences in socio-demographics and HIV knowledge of MSMW and MSMO and (2) to examine the extent of sexual risk behaviours and prevention services which may impact upon HIV transmission to the female population.
Methods
We conducted a cross-sectional study in three provinces of southwestern China, including Sichuan, Guangxi, and Chongqing. Due to the hard-to-reach and secretive nature of the MSM population, we used the snowball sampling method to recruit participants. Each seed helped to recruit potential participants by peer referral. The inclusion criteria were (1) self-reportedly engaged in anal or oral sex with men in the past six months; (2) aged 16 years or older; (3) willing to provide informed consent, and (4) not male sex workers. All eligible participants were asked to complete a self-administered quantitative questionnaire in about 30–40 minutes and compensated with 50 yuan. Each participant was invited to test for HIV after the interview. Anonymity and were confidentiality were strictly controlled in this research. Our study was reviewed and approved by the review boards of Chinese CDC and Chongqing Medical University.
Measures
In the descriptive analyses, study participants were categorised as MSMO and MSMW based on their self-reported sex with men only or sex with men and women in the past six months. Sex with a man was classified as anal or oral sex, and sex with a woman was classified as vaginal, anal, or oral sex. 4
Socio-demographic characteristics information was collected, including age, education, family status (marriage, children), income, age of first sex, and sexual orientation. HIV knowledge was assessed by 13 items, and the level of perceived HIV risk and the quality of the relationship with family members were also assessed.
Sexual risk behaviour information included: multiple male anal sex partners, anal sex role, alcoholism, illicit drug use, and buying and selling sex. Questions on HIV-related services included: condom distribution, lubricant distribution, dissemination of HIV knowledge between partners, HIV counselling and testing in the last year.
We also assessed the rates of consistent condom use with different types of partners (regular and casual men partners, male sex workers, and female partners) of MSMO and MSMW. Consistent condom use was defined as using condoms every time during sexual intercourse in the past six months.
Statistical analysis
We compared socio-demographic characteristics, self- perceived HIV risk and HIV knowledge of MSMO and MSMW using the Cochran-Mantel-Haenszel (CMH) test for categorical variables and Wald test for continuous variables. Logistic regression was employed to examine important risk and prevention factors of bisexual behaviours, which was performed using Statistical Analysis Software (SAS) version 9.2. All important variables associated with MSMW at the level of p < 0.1 were included in the multivariate logistic regression model, and the social-demographic characteristics and research centres as the confounding factors. Adjusted odds ratio (AOR) and 95% confidence intervals (CI) were calculated to evaluate the extent of sexual behaviours that may act a bridge for HIV transmission into general population. We estimated variance and confidence interval of consistent condom use with different types of partners of MSMO and MSMW, using SPSS version 18.0.
Results
A total of 1407 MSM were recruited, and 1402 participants completed a self-administered questionnaire. The refusal rate was 0.35%. With male sex workers excluded, 1345 MSM were included in our study. The number of participants in Guangxi, Sichuan, and Chongqing were 602, 299, and 444 respectively.
Demographic characteristics
Socio-demographics and HIV knowledge of men who have sex with men and women (MSMW) and men who have sex with men only (MSMO).

The two results were from the Wald tests. The other results in this table were from CMH tests.
Sexual risk behaviours and use of HIV-related services of MSMW and MSMO
The correlation between sexual risk behaviour, HIV prevention service usage, and being men who have sex with men and women (MSMW).

There are missing data among 1345 cases, so the actual number of objects in multivariate analysis were 1268.
As is shown in Table 2, after adjustment for socio-demographics characteristics in the multivariate logistic regression model, having multiple anal sex men partners and using illicit drugs remained significantly associated with being MSMW. HIV prevention service and dissemination of HIV knowledge between partners were still significant, whereas HIV testing was not significantly associated with sex with men and women in the case of controlled socio-demographic variables.
Consistent condom use with different types of partner
Consistent condom use was defined as ‘always’ using a condom with that partner or partner type. Figure 1 shows that a small proportion of MSMW had used condoms consistently with female partners in the past 6 months (39.2%). Of MSMW and MSMO who had regular male partners, 69.62% and 73.02% used a condom every time, respectively. Among those who had casual male partners, the proportion of consistent condom use was 67.54% and 74.16%, respectively. The proportion of consistent condom use with male sex workers was 66.67% for MSMW and 48.39% for MSMO. There were no significant differences in the proportion of consistent condom use between MSMW and MSMO with different types of men partners (p > 0.05).
Proportion of consistent condom use with different types of sexual partners for men who have sex with men and women (MSMW) and men who have sex with men only (MSMO).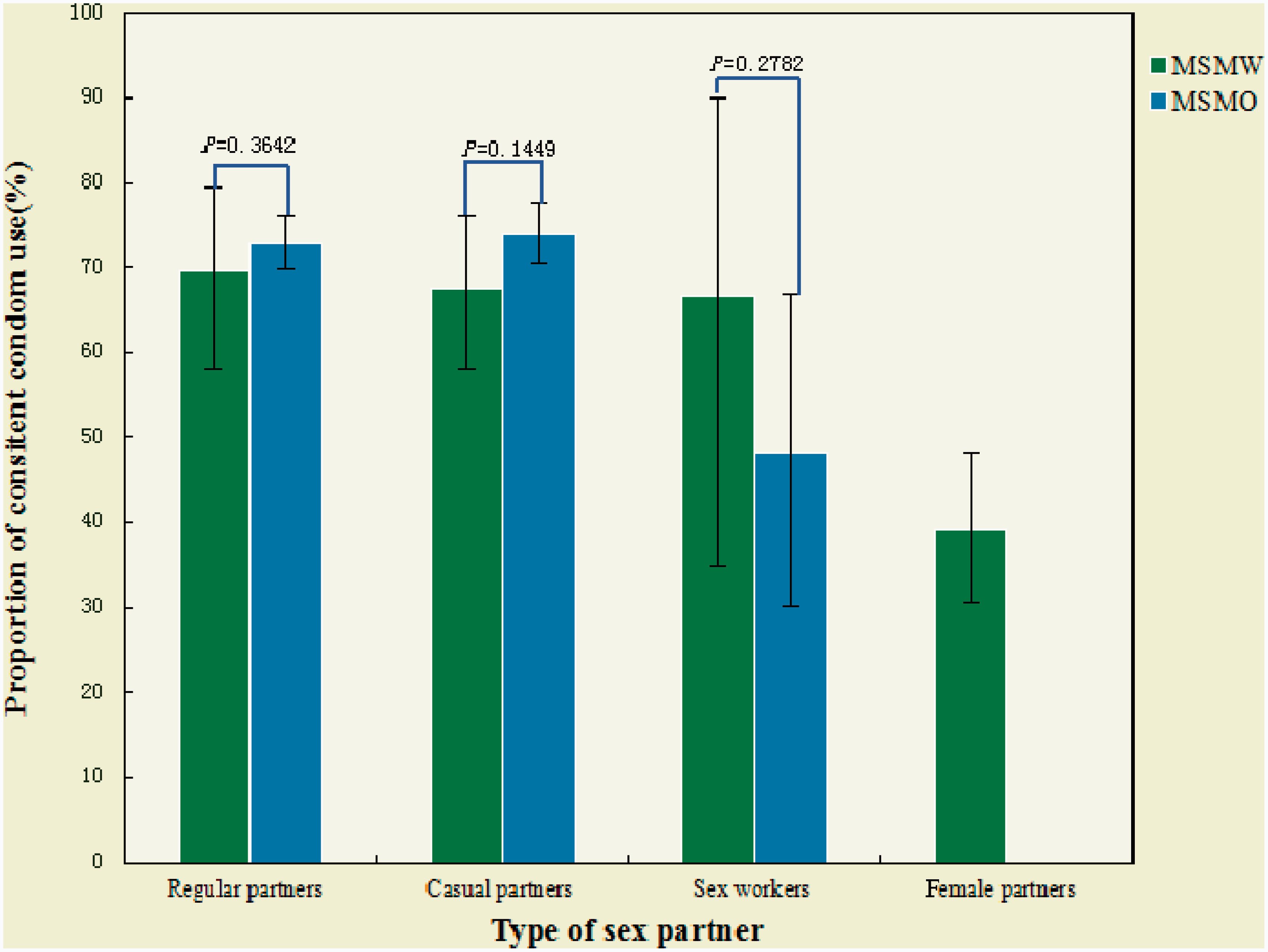
Discussion
This study brings to attention MSMW in China as a priority population with a potentially high risk for HIV transmission. Overall, close to 12% of the MSM participating were MSMW. They were more likely to engage in sexual risk behaviours and less likely to have used HIV-related services than MSMO. MSMW likely present a greater risk of HIV transmission to women,4,5 so efforts are needed to focus on development of sexual behaviour change and health care.
We found that MSMW tended to be older than MSMO; this supports the research finding that sexual behaviours do change over time. 9 But MSMW's trajectories toward multiple partners and HIV risks appear to begin in adolescence. 10 Hence, young MSM deserve dedicated attention in public health research focused on HIV prevention.
MSMW were likely to self-identify as heterosexual, and this identification may prevent them from disclosing their sexual orientation to their female partners, potentially reducing condom use, perceived risk of HIV, and HIV testing of partners. 11 This calls for attention to be paid to the women partners of MSMW, their level of understanding of their male partner's MSM activity, and their awareness of risk of HIV infection in China.
There is substantial evidence that MSMW are more likely than MSMO to engage in illicit drug use.4,11,12 Our data corroborate that point. Syndemic theory posits that as individuals are confronted with adversity, particularly in the forms of social marginalisation, they develop psycho-social health problems such as substance abuse and depression. 13 As few studies have been dedicated to psycho-social health among MSM in China, we recommend future studies could take into account possible psychological factors that may possibly affect MSM risk behaviours.
Condom use with their female partners among MSMW was low. Research carried out in southwestern China recently showed that HIV prevalence among MSMW (15.3%) was higher than that among MSM (11.1%). 5 Thus, the risk of HIV transmission from these men to the female population is high in western China. Given that the desire to have children may compete with the concern to protect partners, education programmes should be sensitive to the whole MSM community and emphasise the importance of consistent condom use with female partners. Current guidelines that do not include specific information about ‘HIV infection risk to female partners’, ‘safer sex with women’ and ‘disclosure of sexual orientation to women’ may require greater efforts to address this prevention need.
In general, the older and married MSM are more likely to use HIV prevention services due to their more conservative perception of HIV infection. 14 However, we found that MSMW were less likely to use a HIV-related service than MSMO, which is not consistent with a previous study in Beijing. 15 This may partly account for the fact that MSMW may bear more social pressure from family obligation and lack of support from partners. MSM marrying due to social pressure often triggers spousal conflict and may result in divorce. 16 Thus we suggest that relevant governmental bodies distinguish MSMW from MSM with more attention paid to the former so that they can access more clearly-targeted care, interventions, and HIV preventive services. Moreover, only 55% MSMW in our study had ever taken a HIV test, indicating that a large proportion of MSMW infected with HIV did not know their status and could continue to spread the virus. Social norms that foster stigma on and discrimination against HIV and sexual orientation are barriers for access to HIV testing among MSM. 17 HIV prevention programmes should also address the socio-cultural factors, challenge homophobic stigma, internalised homophobia, and heterosexism to validate MSM's sexual orientations and ensure they are culturally relevant, with the further purpose of promoting the holistic health of MSM. Such efforts might facilitate the disclosure of MSM's same-sex behaviour to their female partners.
Due to the hard-to-reach nature of the population, our study has several limitations that should be noted. First, we used snowball sampling to recruit participants, leaving much room for the enhancement of the representativeness of the samples. Second, only 159 (11.8%) of our samples were MSMW, which may have reduced the statistical power and the results of odds ratios may not be very precise. Third, like any cross-sectional surveys, self-reported data are subject to the potential of social desirability bias. And the associations derived might have been spurious due to misclassification of MSMO and MSMW. Fourth, we assessed the difference in socio-demographics, sexual risk behaviours, and prevention services of MSMW and MSMO during a specific time period. Longitudinal studies are needed to quantify the difference over a longer period of time. Collected data about partnership characteristics and HIV prevention service were insufficient. Further studies are warranted to document more about the female partners' characteristics which could affect MSMW and a qualitative method might be useful to obtain in-depth narratives. Little is known about the HIV-related services of MSMW, and more research is needed to explore the potential facilitators and barriers for access to HIV prevention services.
Despite these limitations, our study has important implications for future interventions. Public health authorities' support should highlight the importance of bisexuals as a potential epidemiologic bridge. HIV prevention programmes such as advocating safe sex and promoting regular HIV testing targeted at bisexual men should be warranted. It is also important that HIV prevention programmes such as counselling and educating MSM's women partners are encouraged in areas where HIV is prevalent among MSM. Same-sex stigmatisation and disclosure should be addressed to improve the social contexts for MSM in China. Long-held conventional wisdom may be hard to change, but the rapid economic development and cultural transition would bring opportunities to promote the social and psychological health of MSM.
Conclusions
As outlined in this article, MSMW is a potentially large risk group, placing their women and men partners at a greater risk of contracting HIV. Interventions to change the existing behaviours are needed to promote safer sexual practice among MSMW, but strategies that address the socio-cultural factors should be warranted to sustain long-term sexual health.
Footnotes
Acknowledgments
We thank all participants and investigators for their help. We are also grateful to the staffs from local offices of Centers for Disease Control in Guangxi, Sichuan, and Chongqing for their aid in the data collection during our research.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Key Project for Infectious Diseases of the Ministry of Science and Technology of China , NO.2012ZX10001007