
Abstract
We present the case of a 61-year-old male with a long-standing perineal and scrotal lesion. Investigations eventually revealed cutaneous tuberculosis, with complete resolution after appropriate treatment. It highlights the variable presentation of cutaneous tuberculosis and the importance of considering the diagnosis in chronic lesions.
Introduction
Patients with genital lesions may present late in the course of their disease, when the features may have been modified by inappropriate treatment. We present a patient with a longstanding perineal and scrotal lesion, misdiagnosed for many years as psoriasis, but eventually shown to be cutaneous tuberculosis, which responded well to treatment. It illustrates the importance of clinico-pathological correlation and highlights that rare diseases can present at unusual sites.
Case report
A 61-year-old man presented with a perineal lesion, which had been present for 20 years. It had been diagnosed at the time as psoriasis and treated with potent topical steroids intermittently since. He had no systemic or local symptoms and his only concern was that the lesion was increasing in size. He had a medical history of ischaemic heart disease and there was no relevant family history. He was a heterosexual married man who had relocated from India in the 1970s, and now worked in an office.
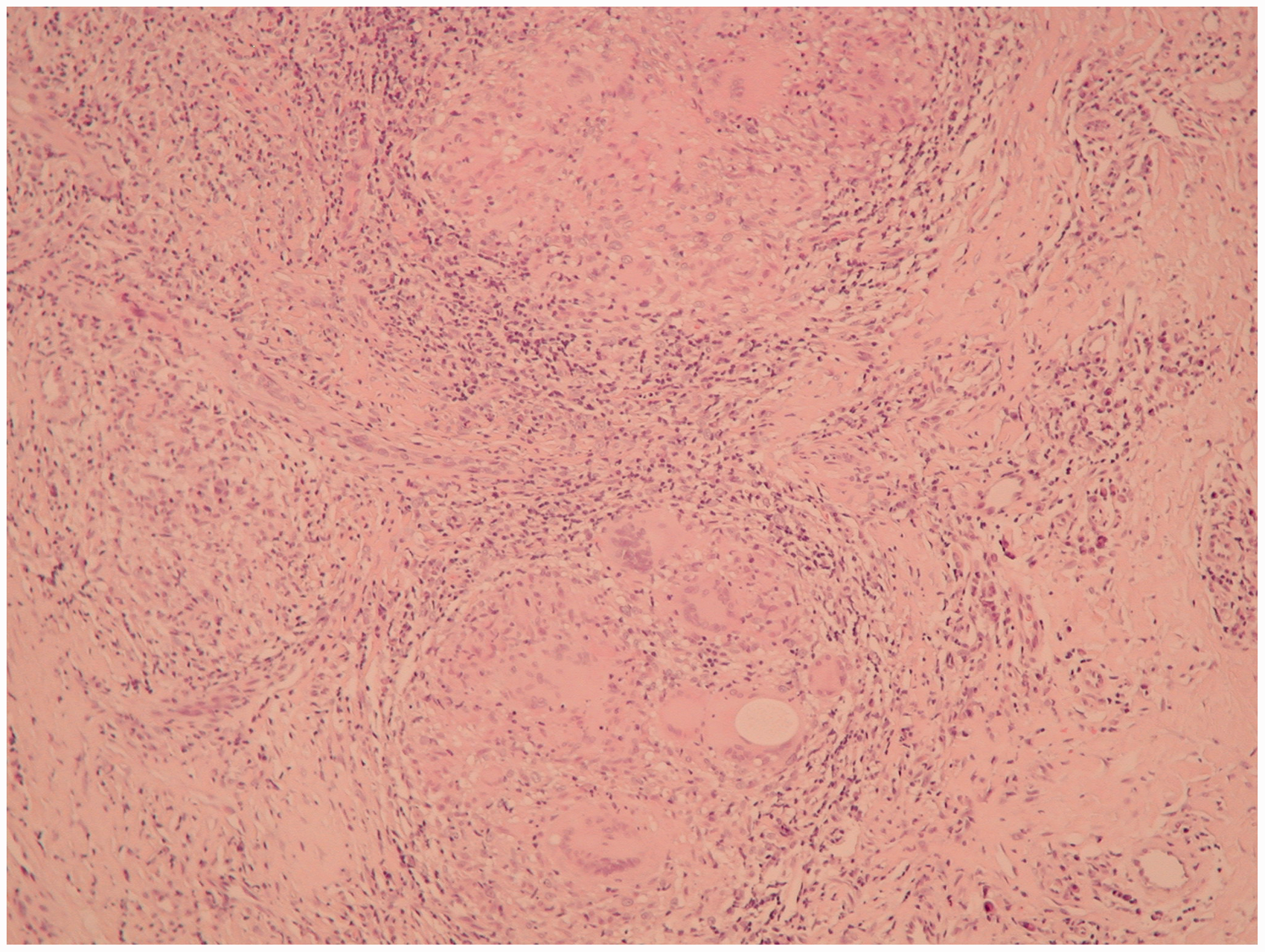
On examination, a firm indurated plaque with superficial ulceration was noted on the perineum extending to the scrotum and right buttock (Figure 1a). There were no palpable inguinal lymph nodes. The clinical differential diagnoses included ano-genital Crohn’s disease, hypertrophic lichen planus, cutaneous lymphoma or a granulomatous disorder such as sarcoidosis or tuberculosis. Laboratory investigations, including haematological parameters, renal and liver function and serum angiotensin converting enzyme were normal and his chest X-ray was clear. A TB-Elispot test was positive. A punch biopsy was taken from the plaque which showed multiple non-caseating granulomata and a dense inflammatory infiltrate (Figure 2). No acid-fast bacilli were seen on Ziehl-Neelsen staining. Fungal stains were negative. A diagnosis of cutaneous perineal tuberculosis was made and he was commenced on anti-tuberculosis therapy (rifampicin, isoniazid, pyrazinamide and ethambutol for two months followed by a further four-month course of rifampicin and isoniazid). There was a dramatic response within just three weeks of starting treatment. He completed a six-month course of therapy and the plaque completely resolved with some post-inflammatory hypopigmentation (Figure 1b).
(a) Ulcerated perineal plaque; (b) resolution of plaque after treatment. Skin biopsy showing non-caseating granulomata and inflammatory infiltrate.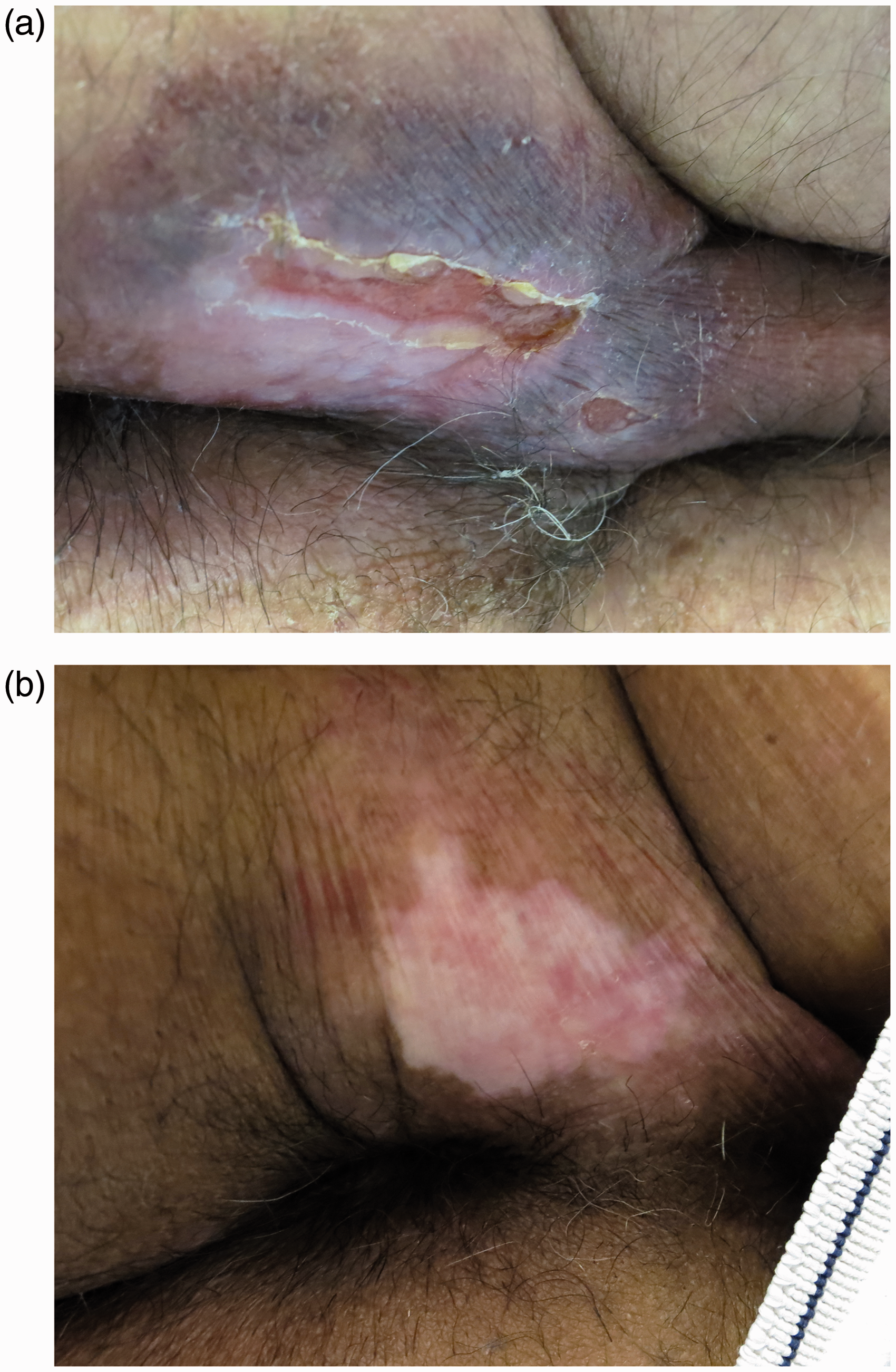
Discussion
Extrapulmonary tuberculosis accounts for 15% of all cases and can affect any organ. 1 Ano-perineal tuberculosis is a very rare form of extrapulmonary disease, accounting for less than 1% of cases. It presents in many ways 2 making diagnosis a challenge. It can exist alone, or be associated with gastrointestinal tuberculosis, via direct extension or haematological or lymphatic spread. Anal fistula is the most common presentation but other lesions include ulceration (as in this case), abscess, anal stricture, discharge and haemorrhoidal thrombosis with or without other systemic features.3–6 It is important to recognise this rare presentation as it requires specific anti-tuberculous treatment. 7
The appearance of cutaneous lesions in the ano-genital area can be significantly altered due to the moist environment and this renders clinical assessment alone challenging in making a final diagnosis. In this case, there were no deep fissures or other clinical signs to suggest cutaneous Crohn’s disease and he had no gastro-intestinal complaints. If bowel symptoms are present, it is important to exclude gastrointestinal tuberculosis as this can mimic Crohn’s disease. 8 He was otherwise well with no other symptoms to suggest sarcoid or systemic disease. Occasionally, sarcoid-like histological patterns are seen in patients with cutaneous tuberculosis and positive immunoassays are helpful. 9 A thorough history and examination is the starting point in diagnosis and helps to identify extra-cutaneous foci of infection. Tuberculin-skin-testing can be negative in a quarter of cases and acid-fast bacilli may not be present. Biopsy is important but acid-fast bacilli may only be seen in 8% cases. 10 Although culture is perhaps the most reliable method to detect the presence of mycobacteria, it takes a long time and the yield is often low, and has been estimated at 53% in one study. 10 Polymerase chain reaction can also be used. However, the enzyme-linked immunospot assay for interferon-gamma (TB Elispot) has been shown to be very helpful in the diagnosis of cutaneous tuberculosis 11 with a sensitivity of 91.6%. 12 A negative test therefore makes the diagnosis of tuberculosis unlikely. Treatment is with standard anti-TB therapy 13 and the diagnosis is further supported by the prompt resolution of lesions.
This case highlights the variety of presentations of cutaneous tuberculosis, and even at unusual sites it should be included in the differential diagnosis of chronic lesions.
Footnotes
Acknowledgements
We would like to thank Dr Wassim Al-Salti, Consultant Histopathologist for help with the histology and photomicrographs, and Dr Angela Jones, Consultant Respiratory Physician for advice on anti-tuberculous therapy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.