
Abstract
In the context of a shift from exceptionalism to normalisation, this study examines recommendations/evidence in current pan-European/global guidelines regarding pre-test HIV testing and counselling practices in health care settings. It also reviews new research not yet included in guidelines. There is consensus that verbal informed consent must be gained prior to testing, individually, in private, confidentially, in the presence of a health care provider. All guidelines recommend pre-test information/discussion delivered verbally or via other methods (information sheet). There is agreement about a minimum standard of information to be provided before a test, but guidelines differ regarding discussion about issues encouraging patients to think about implications of the result. There is heavy reliance on expert consultation in guideline development. Referenced scientific evidence is often more than ten years old and based on US/UK research. Eight new papers are reviewed. Current HIV testing and counselling guidelines have inconsistencies regarding the extent and type of information that is recommended during pre-test discussions. The lack of new research underscores a need for new evidence from a range of European settings to support the process of expert consultation in guideline development.
Introduction
HIV testing and counselling (HTC) is considered essential for effective HIV prevention and treatment. 1 The recent shift away from ‘HIV exceptionalism’ towards normalisation of testing suggests that HIV should be treated more like other infectious diseases requiring early diagnosis to ensure appropriate prevention and treatment. 2 A more routine approach to offering HTC – provider-initiated testing and counselling (PITC) – has been recommended for, and adopted in, clinical settings since 2002 in order to achieve higher rates of HIV testing. 1 This is reflected in guidelines in the US, 3 UK 4 and by the WHO/UNAIDS, 5 which promote voluntary, opt-out (rather than opt-in) HIV testing strategies as a standard part of medical care for patient populations. 6 These efforts to increase the offer and uptake of testing by reducing barriers and stigma associated with an HIV test are typically considered easier to achieve through reduced pre-test counselling (based on the assumption that there is no need for special counselling skills beyond that required for normal clinical practice) and the removal of written informed consent. 7
Clinical guidelines and recommendations about best clinical practice are statements designed to assist health practitioners and patients making decisions about appropriate health care in specific circumstances.8–10 A number of regional and global guideline documents exist to support and promote best practice regarding the decisions and processes carried out in health care settings before an HIV test is undertaken across the WHO European Region. These include regional documents from the European Monitoring Centre for Drugs and Drug Addiction (EMCDDA), 11 HIV in Europe, 12 the European Centre for Disease Prevention and Control (ECDC), 13 the European Office of the International Union against Sexually Transmitted Infections (IUSTI) 14 and the WHO Regional Office for Europe, 15 and global documents from UNAIDS and WHO.5,16
In the context of the shift towards normalising HIV testing, to date, little work has examined recommendations contained in these guidelines about what should happen prior to testing a patient for HIV. This paper is based on broader research that has been undertaken by the Centre for Social Research in Health at UNSW Australia, commissioned by HIV in Europe, to review testing and counselling guidelines across European country contexts. In this paper, we review and synthesise the best practice HIV testing guidelines relevant to European contexts, relating to pre-test counselling and informed consent, and document the extent of variation in recommendations. In addition, we review, and where research is available, update the evidence used to support these recommendations.
Methods
Identification of guidelines
Global and regional guideline documents were identified via a targeted internet-based search of published documents on websites of organisations known to be involved in offering guidelines around HIV service delivery in health care settings. We identified four guideline documents that are relevant to countries in the WHO European Region: ‘Guidance on provider-initiated HIV testing and counselling in Health Facilities’ by WHO/UNAIDS 5 ; ‘Scaling up HIV testing and counselling in the WHO European Region, policy framework’ by WHO Europe 15 ; ‘HIV testing: increasing uptake and effectiveness in the European Union, ECDC guidance’ by the ECDC 13 and ‘2014 European Guidance on HIV testing’ by IUSTI. 14
National guidelines, which are designed for specific national contexts, were outside the scope of this review. Guidelines that are not published in English, or focus on the delivery of HTC outside the WHO Europe Region, were also excluded from the review. HIV in Europe’s guidance on HIV indicator conditions 12 was excluded as this focussed primarily on the identification of people to test. Guidelines that focus specifically on issues pertaining to particular population groups (e.g. couples, 16 drug users,11,17 refugees, 18 institutionalised adolescents or adults 19 ) were also excluded.
Data extraction and synthesis
Criteria used for grading scientific evidence.
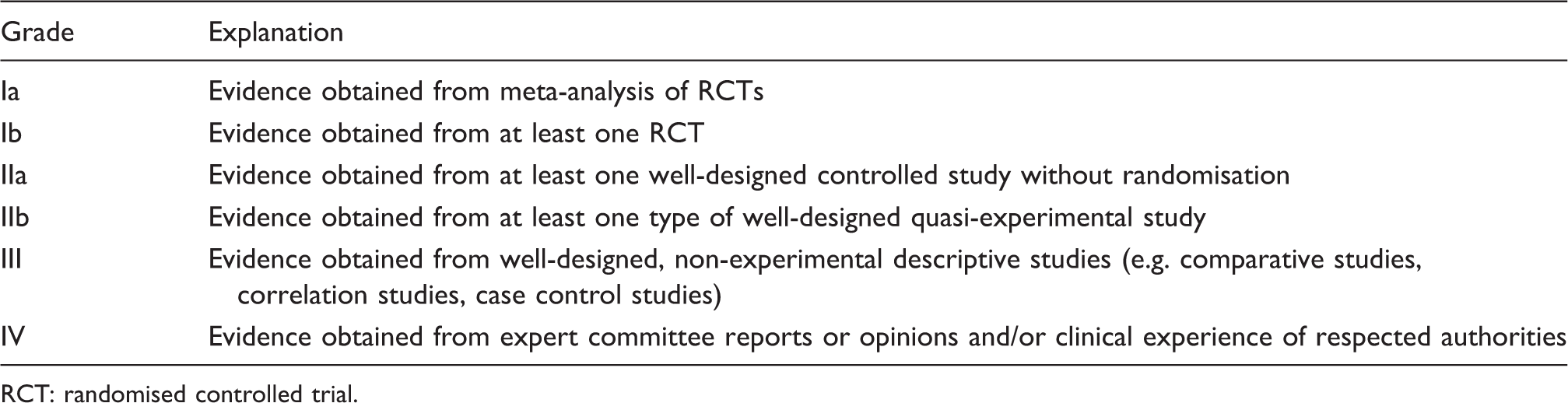
RCT: randomised controlled trial.
Literature review
A literature review was undertaken to update the evidence used to support existing recommendations. Two major electronic databases (PubMed, Web of Science) were searched for studies published between 2000 and November 2014. The following search terms were used: HIV testing OR HIV counselling. The review process consisted of several stages: 4138 papers were identified from the initial search; after screening of titles, a total of 533 articles were added to an EndNote database for management and further screening; duplicate titles were removed; the remaining 482 article titles/abstracts were examined to determine relevance for further review based on the criteria outlined below; the full text of 38 papers was collected for final review; findings from the final eight papers are included in this paper. The final eight papers were graded using the criteria outlined in Table 1. 20 Papers were excluded if they focussed on issues pertaining to HIV post-test issues, reported on research in developing country settings or were undertaken in relation to emergency department or community-based settings, or rapid testing.
Review of guidelines
Gaining informed consent
There is general consensus in guidance from WHO/UNAIDS, 5 WHO Europe, 15 ECDC 13 and IUSTI 14 that informed consent must be gained from all individuals prior to having an HIV test, individually, in private and confidentially. This guidance is based predominantly on expert opinion, although current IUSTI guidelines 14 also refer to the previous set of IUSTI guidelines 22 as well as the UK testing policy 4 in support of this recommendation.
There is also consensus that verbal consent is sufficient; written consent is not required. WHO/UNAIDS 5 recommend institutions or jurisdictions requiring written consent for testing review current policy to fall in line with this consensus. IUSTI 14 refers to Grade IV studies in support of this position but does not provide details of the specific studies. The ECDC guidelines 13 refer to three US Grade III studies23–25 and four Grade IV opinion/case study-based articles2,26–28 to illustrate that verbal consent is adequate and separate consent for HIV is not required. However, the ECDC guidelines also highlight two Grade IV articles29,30 that argue the opposite position: the need to gain patients’ specific consent before HIV testing in order to ensure patient agency in decision making.
In addition to the guidelines reviewed in this paper, it is worth noting that the US HIV testing guidelines 3 refer to two US Grade IIb studies,31,32 one Canadian Grade III study 33 and two UK Grade III studies34,35 to illustrate that rates of HIV screening are consistently higher in opt-out settings that do not require explicit written consent for HIV testing.
Pre-test information
All guidelines recommend providing pre-test information during a pre-test discussion or assessment, with the basic aim of providing sufficient information to a client to gain informed consent before testing.13,14 This is in contrast to undertaking pre-test counselling, which has been defined as ‘a longer intervention including a sexual history and risk assessment designed to perform the same functions as pre-test discussion, but also to establish the person’s likely response to the possible result’. 13 These recommendations are based largely on expert opinion. The latest European HIV testing guidelines from IUSTI 14 also refer to the British HIV testing policy 4 in support of this recommendation. Only the ECDC guidelines 13 provide a reference to published evidence to support this recommendation. This was a US Grade Ib study 36 that illustrates no difference in patients’ decision to accept HIV testing between interventions offering abbreviated versus standard pre-test HIV counselling in prenatal settings, implying that more extensive pre-test counselling is not required.
Beyond the guidelines under review, the US HIV testing guidelines document 3 refers to other published research in support of the recommendation to remove the need for pre-test counselling before an HIV test. It references two US Grade III studies37,38 and one UK Grade IV study 39 to illustrate that prevention counselling is a barrier to uptake of HIV testing. Furthermore, the same studies identified above in relation to informed consent (two US Grade IIb studies,31,32 one Canadian Grade III study, 33 two UK Grade III studies34,35) are provided as evidence to show that rates of HIV screening are consistently higher at opt-out prenatal (i.e. a women will receive an HIV test as part of the routine panel of prenatal tests unless she declines) and STD services that do not require pre-test counselling.
Guidelines explain that pre-test information can be delivered verbally or via other methods such as an information sheet or by educational video. IUSTI’s guidelines 14 refer to a Grade III UK study 40 to illustrate that the provision of an information leaflet about HIV testing can provide or replace much of the information needed prior to obtaining informed consent and is effective in many settings. The ECDC guidelines 13 refer to two US Grade Ib studies41,42 to illustrate that an educational video may be a feasible alternative for providing testing information when trained staff are unavailable for direct, interactive counselling.
Recommendations relating to pre-test information provision.
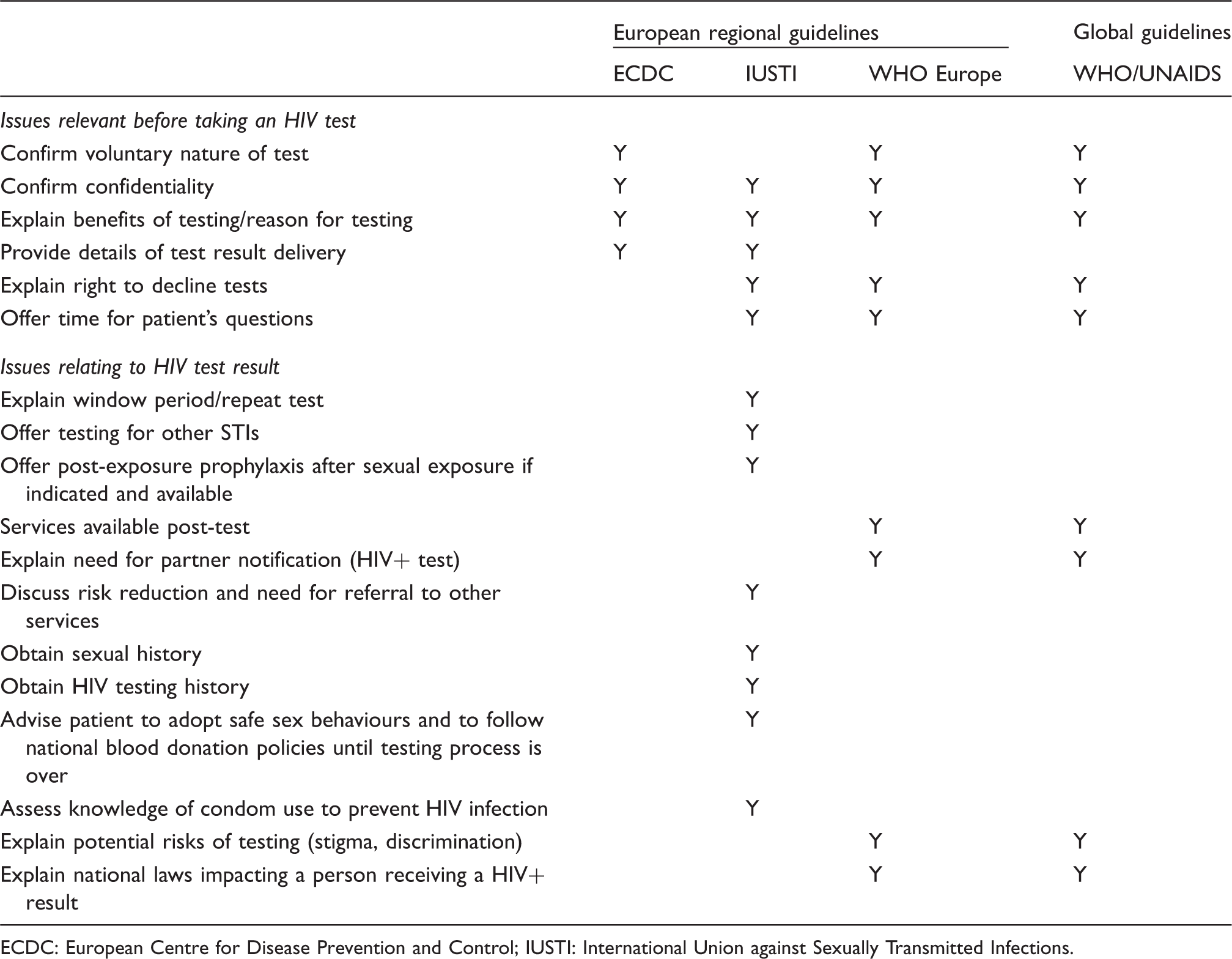
ECDC: European Centre for Disease Prevention and Control; IUSTI: International Union against Sexually Transmitted Infections.
There is general agreement in guidelines about the first aspect. Recommendations about issues to be discussed before an HIV test takes place include: the voluntary, confidential nature of the test; the reason for testing; what the test procedure consists of; information about delivery of test results; the patient’s right to decline a test; the offer of time for patients to ask questions. The ECDC guidelines 13 only provide guidance about this first aspect, whereas regional guidelines by IUSTI 14 and WHO Europe, 15 and global guidelines by WHO/UNAIDS 5 recommend that both aspects are included in pre-test information.
With regard to issues to be discussed that encourage patients to think about possible implications of the test result, there are no shared recommendations. The guidelines by IUSTI include the following issues: information about processes (e.g. window period and possible need for repeat test; offering STI testing; offering post-exposure prophylaxis after sexual exposure if indicated and available); personal information gathering (e.g. sexual history of patient, obtaining a person’s HIV testing history) and prevention and risk reduction information (e.g. discuss risk reduction and need for referral to other services; knowledge of condom use to prevent HIV infection; advise patient to adopt safe sex behaviours and to follow national blood donation policies until the testing process is over). 14 Alternatively, guidelines by WHO/UNAIDS 5 and WHO Europe 15 recommend that pre-test discussion should include information about issues that might arise after receiving an HIV-positive test result. This includes services available post test, the need for partner notification, the potential risks of testing (stigma, discrimination) and relevant national laws. None of these guidelines refer to specific published research to support either of these positions. Instead, recommendations are based on expert consultation.
Recent research informing future guidelines
Our literature search of studies previously uncited in regional/global guidelines revealed limited new research that could be used to inform the development of future HTC guideline testing. Findings from seven independent studies, and one review paper encompassing three of these studies, are summarised below.
Normalised opt-out testing
New quantitative and qualitative evidence was found to illustrate support for opt-out HTC approaches. A Grade III Dutch study 43 in an STI outpatient clinic in Amsterdam illustrated the positive effect of an opt-out strategy on the uptake of testing, with an increase from 71% to 95% between 2006 and 2007. In 2007, 12% of men who have sex with men (MSM) and 4% of heterosexuals with (presumed) negative or unknown HIV serostatus declined HIV testing, and refusals gradually decreased to 7% and 2% by the year end; in 2006, before introducing opt-out testing, 38% of MSM and 27% of heterosexuals declined testing.
A systematic review 44 of qualitative research studies relating to the views and attitudes of MSM concerning HIV testing in high-income countries offers insight into patient perspectives. It identified two UK Grade III studies reporting that patients recommended eliminating the requirement to answer questions about sexual behaviour 45 and as well as blending HIV testing with routine examinations to encourage its normalisation. 46 Another Grade III qualitative UK study 47 found that patients regarded opt-out testing for HIV on general practitioner (GP) registration as acceptable. There was reported concern that screening would still be targeted at groups in which HIV prevalence is higher, based on clinicians’ judgement of patients’ behaviours, sexuality or ethnicity.
Pre-test counselling
One Grade III UK study illustrated the positive impact of using information leaflets instead of verbal pre-test counselling on HIV testing rates. In an audit at a UK clinic, 48 HIV testing was significantly higher after introducing an information leaflet in place of verbal pre-test counselling.
Some relevant findings about patient perspectives can be reported from qualitative studies. A systematic review 44 of qualitative research with MSM in high-income countries identifies two findings. First, attitudes towards pre-test counselling were mixed. A Grade III study 46 found generally positive attitudes towards pre-test counselling, while a Grade IV study 49 found that participants saw counselling as ‘repetitive’ and ‘unnecessary’ and rejected the moralising tone of counselling they had received. Second, the same two studies46,49 identified that confidentiality and anonymity were perceived as important aspects of testing, with almost half of MSM participants stating that they would only test if an anonymous option was maintained. 49 Results from another Grade III qualitative study amongst MSM in Tbilisi, Georgia 50 illustrates that efforts to educate and provide unobtrusive and anonymous HTC services to MSM may be critical to maintain the low rates of HIV and avoid an HIV epidemic in the Republic of Georgia.
Discussion and conclusions
Review and comparison of recommendations in guidelines
There are issues that are agreed upon in all guidelines under review. There is consensus that informed consent must be gained from all individuals prior to having a HIV test, individually, in private and confidentially.5,13–15 There is consensus that verbal consent is sufficient; written consent is not required. There is also agreement that a pre-test assessment or discussion serves the purpose of providing pre-test information rather than pre-test counselling. Pre-test information can be delivered verbally or via other methods such as an information sheet.
We have identified two aspects to pre-test information: (1) issues to be discussed before a HIV test takes place and (2) issues to be discussed that encourage patients to think about possible implications of the test result. There is general agreement about the importance of including the first aspect, forming a minimum standard of information to be provided (i.e. voluntary, confidential nature of the test; reason for testing; test procedure; information about delivery of test results; right to decline a test; time for patients to ask questions). Through limiting pre-test discussion to this information, it is assumed that the HIV test will become easier, quicker and more normal.
However, guidelines differ regarding the second aspect of pre-test information. The ECDC guidelines 13 recommend only a focus on the first aspect and do not discuss the second at all. Guidelines by IUSTI, 14 WHO Europe 15 and WHO/UNAIDS 5 advise that both aspects are included in pre-test information. However, regarding the second aspect, there are no shared recommendations about which information should be covered in pre-test discussions. WHO/UNAIDS 5 and WHO Europe 15 recommend that pre-test discussion should include information about the potential risks of testing (e.g. stigma, discrimination). In addition to the loss of an opportunity for preventative education, a possible concern arising from guidelines produced by IUSTI 14 and ECDC 13 is that patients may not be prepared for the possible social, discriminative and legal outcomes that might arise from undertaking an HIV test in their local context.
Evidence used to support recommendations
Several conclusions can be drawn about the evidence used to support guidelines. First, there is a heavy reliance on expert consultation in the development of current guidelines. Expert consultation offers an important opportunity to draw on expertise and experience in the development of guidelines. Yet, we do not know the extent to which this expert opinion is based on familiarity with available evidence, personal experience and concerns, or patient experiences. Second, we do not know the extent to which experts from all areas of the WHO European Region are involved in guidelines consultation processes. Third, scientific evidence, where referenced, is often more than 10 years old and based on research in the US and UK. Most probably, these research findings cannot be extrapolated to all European contexts, especially in South, Central and Eastern Europe.
Our search for new research about HTC in health care settings (previously uncited in the HTC guidelines under review) highlighted the dearth of studies being undertaken and published. We found only eight new papers to supplement the existing evidence base. These offered support for opt-out approaches for testing, use of an information leaflet to deliver pre-test information and the need for confidential, anonymous HIV testing. Two studies in the UK offered mixed qualitative evidence about patients’ perceived acceptability of pre-test counselling. This review goes some way to answering the question why so little robust evidence is referenced in guidelines – the answer being that all too often this type of evidence may not exist.
Findings from this paper highlight several conclusions to assist with the future development of HTC guidelines. First, some consensus is required about the content of pre-test information, and the outcomes that might arise from a focus on providing only a minimum standard of pre-test information. Input should be sought from experts representing the range of settings across the WHO European Region. This will ensure that general recommendations in future guidelines cater for possible outcomes arising in different parts of the region and assist with the challenge of translating general guidelines into national and local strategies. We also propose that client perspectives are incorporated more explicitly in expert consultation processes through inclusion of clients, or representatives of client groups, in these processes where this is not already occurring.
Second, it is clear that new research is needed to examine the delivery of pre-test procedures and the impact this has on clients’ lives. Such research would assess the effectiveness of pre-test procedures from a range of settings across the WHO European Region. This is particularly important, given the current developments and changes in testing processes, and the introduction of new technologies such as rapid and home-based testing. However, we recognise that developing public health recommendations is a difficult area of evaluation research. Experimental evaluation is often unfeasible and too costly on the scale required, and unethical for clients participating in the control arms of these studies. There is, however, little published research that evaluates the extent to which health care personnel are getting better at offering HIV tests to clients. Rather than advocating more experimental research around successful testing procedures, it would be useful to see greater recording of ‘adverse’ events and poor practice, from the perspectives of clients, as a way of learning about what can be done better in the future.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the HIV in Europe Initiative and supported by the HIV in Europe Steering Committee.