
Abstract
Pre-exposure prophylaxis (PrEP) has been shown to reduce the risk of HIV transmission but has the potential to cause harm if not used properly. Pharmacists are well-positioned to foster PrEP’s efficacy but little is known whether they would endorse it as an HIV prevention tool. The objective of the study was to determine Canadian HIV pharmacists’ support for PrEP and to identify current barriers to promoting PrEP. Canadian pharmacists with experience in HIV care were invited to complete an online survey about their experiences, opinions, and learning needs regarding PrEP from December 2012 to January 2013. Among the 59 surveys received, 48 met criteria for final analysis. Overall, 33 (69%) respondents would provide education positively supporting the use of PrEP and 26 (54%) believed Health Canada should approve PrEP for use in Canada. Familiarity with the concept of PrEP and practice characteristics examined did not appear to be significantly associated with support for PrEP in univariable analyses. The principal barriers to promoting PrEP included inadequate drug coverage and insufficient knowledge to educate others. Many Canadian HIV pharmacists would endorse PrEP for high-risk patients; however, wider dissemination of information and lower drug costs may be needed to make PrEP more widely promoted.
Introduction
With estimates of 35 million people living globally with HIV in 2013, 2.1 million new infections occurring in the same year 1 and no cure on the horizon, new biomedical interventions are gaining momentum to help curtail the HIV epidemic. Pre-exposure prophylaxis (PrEP) is the daily use of antiretrovirals by a HIV-uninfected individual to avert HIV infection. In 2012, after the publication of several landmark studies demonstrating its ability to decrease the risk of HIV sexual acquisition,2–4 the combination antiretroviral emtricitabine-tenofovir disoproxil fumarate (Truvada®) was approved by the United States’ Food and Drug Administration for PrEP use. A year later, efficacy and safety were also confirmed among uninfected injection drug users (IDUs). 5 However, due to concerns regarding adherence, drug resistance and the potential for users to increase risk-taking behavior (‘risk compensation’), there have been divergent opinions among healthcare providers and policy-makers on the role of PrEP and how best to roll out this prevention method.6–9 At present, the manufacturer of Truvada® has not applied for regulatory approval of PrEP in Canada, hence any such use of the product in Canada is off-label.
In Canada, the role of the pharmacist involves collaborating with patients and other healthcare providers to optimise medication use and help achieve positive health outcomes. Canadian pharmacists may be involved in advising physicians and patients on pharmacological and non-pharmacological management, monitoring for drug efficacy and toxicity, and educating patients on correct medication use. Since many aspects of PrEP implementation fall within the scope of pharmacists’ practice and expertise, 10 pharmacists can be a valuable asset to support its proper use. PrEP’s efficacy is critically dependent on medication adherence. 11 Negative results from two trials12,13 were likely driven by low levels of adherence, and research has suggested efficacy as high as 99% with perfect adherence to daily medication. 14 Pharmacists have shown to make an impact by improving patients' medication adherence.15–17 They have extensive experience in medication counselling and other adherence-enhancing strategies such as simplifying therapy and utilising blister-packaging to organise medication administration. Recurrent visits to refill medications provide opportunities for community pharmacists to manage emergent side effects, support sustained PrEP adherence which can decline over time, 18 and prevent drug resistance by monitoring for acute HIV infection. In community settings, they are in a unique position to identify and engage high-risk individuals into care, especially when dispensing medications for sexually transmitted infections (STIs), HIV post-exposure prophylaxis, or providing education on STI prevention methods. Pharmacists working in ambulatory clinics can assist in follow-up care, monitoring blood work for drug toxicity, HIV seroconversion, and cultures for new STI infections. In some jurisdictions, they may also be able to facilitate prescription renewals. However, despite their potential involvement, only one US study has explored pharmacists’ knowledge and perception of PrEP. 19 Little is known on what Canadian pharmacists understand of PrEP, or if they would endorse this prevention strategy, particularly since Truvada® is not approved for PrEP use in Canada. We therefore conducted a cross-sectional survey of Canadian pharmacists to evaluate their attitudes and readiness for PrEP.
Methods
Canadian pharmacists who were members of the Canadian HIV/AIDS Pharmacists Network or the Ontario HIV Professional Specialty Group were invited via email to anonymously complete a 27-item online survey using the Fluid Surveys website from 4 December 2012 to 3 January 2013. Members were encouraged to forward the invitation to relevant colleagues in their jurisdiction and to inform the researchers that they had done so in order to track the number of pharmacists reached. Collectively, based on feedback from pharmacists who forwarded the email to other colleagues, the survey reached approximately 161 pharmacists. Individuals were eligible to participate if they identified as a pharmacist practicing in Canada with some experience in HIV management.
The survey, developed from a review of published literature6–9 and input from medical, pharmacy, and community perspectives, contained a mixture of multiple choice and Likert scale questions that were organised into four sections: demographics and practice-related information, familiarity and previous experience with PrEP, opinions on key issues related to PrEP implementation, and current barriers and learning needs (supplementary file). Participants were permitted to omit any question and could withdraw at any time during the survey. The survey instrument was pilot-tested by three pharmacists for clarity, and conducted in both English and French.
The primary objective was to determine Canadian HIV pharmacists’ support for PrEP, as quantified by the proportion of respondents who answered ‘yes’ to the question: ‘Knowing what you know about PrEP now, would you provide education positively supporting the use of PrEP to a patient at high risk of HIV infection?’ Univariable logistic regression models were used to identify variables associated with support for PrEP.
A key secondary objective was to determine the degree of support for regulatory approval for PrEP. Participants were asked the following: ‘According to one study among men who have sex with men (MSM), oral PrEP provided 44% protection against HIV infection overall and 73% protection in participants who used PrEP consistently (i.e. took the medication at least 90% of the time). Other studies show that PrEP provides a similar level of protection among heterosexual men and women, but a couple of studies have been halted in heterosexual women in Africa because of lack of efficacy potentially due to low levels of adherence among study participants. Considering this level of protection, do you believe Health Canada should approve PrEP for use in Canada?’
Additional secondary objectives included determining: the extent to which patients were inquiring about PrEP, how patients were obtaining PrEP medications, and understanding pharmacists’ beliefs around the implementation of PrEP in terms of efficacy, target patient population, and risks. These results were summarised using descriptive statistics.
Our target sample size was based on the minimum number of participants required to estimate the primary outcome measure with reasonable precision. Because there were no published data on this proportion at the time of study initiation, we conservatively estimated the true proportion at 0.5. Using the equation

The study protocol was approved by the Research Ethics Board of St. Michael’s Hospital and was not externally funded. All participants were given the opportunity to enter their name in a draw for several gift certificates or a tablet computer.
Results
Respondent characteristics, n = 48. a
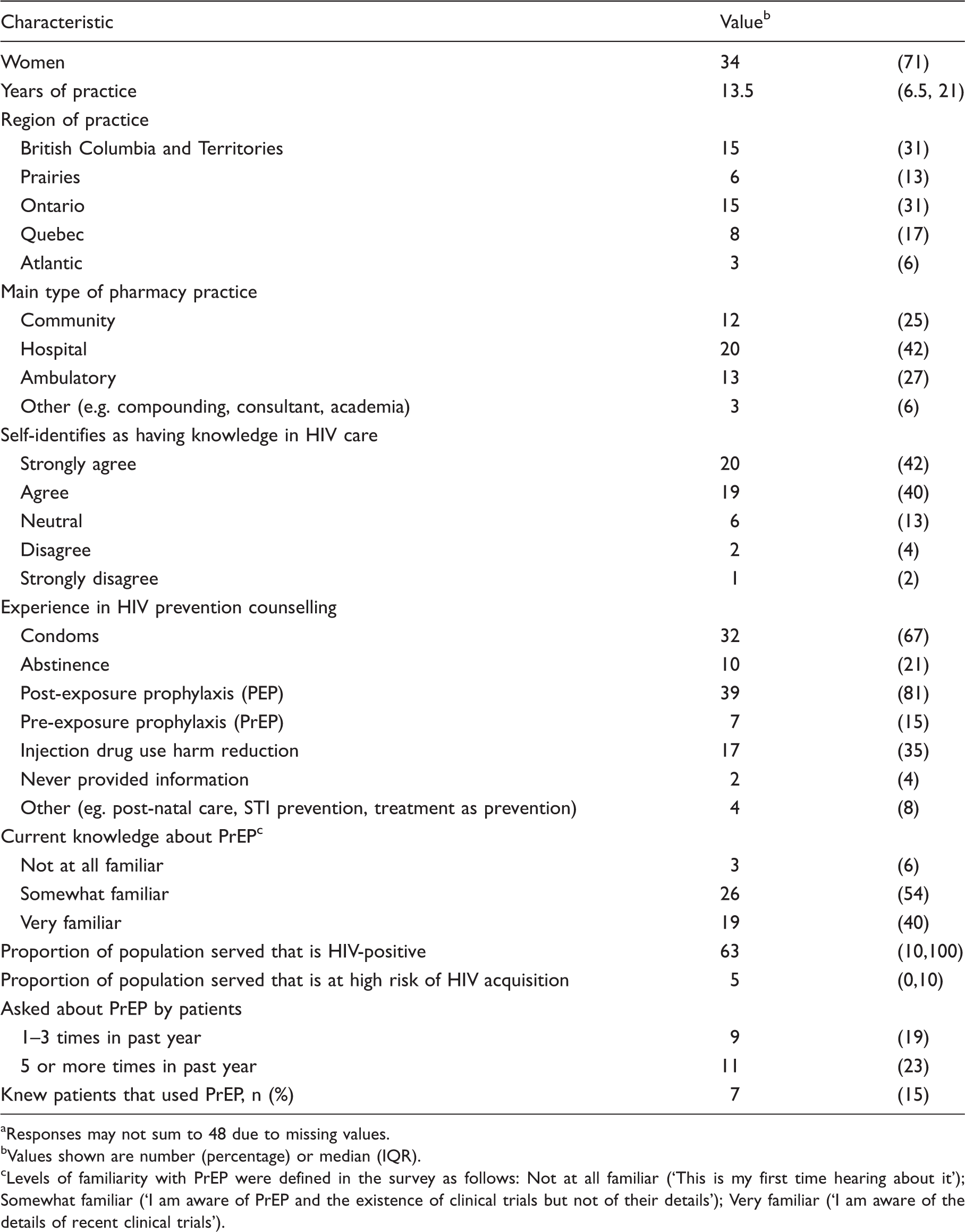
Responses may not sum to 48 due to missing values.
Values shown are number (percentage) or median (IQR).
Levels of familiarity with PrEP were defined in the survey as follows: Not at all familiar (‘This is my first time hearing about it’); Somewhat familiar (‘I am aware of PrEP and the existence of clinical trials but not of their details’); Very familiar (‘I am aware of the details of recent clinical trials’).
The majority (82%) self-identified as having knowledge in HIV care, and nearly all (94%) described themselves as either ‘somewhat familiar’ or ‘very familiar’ with the concept of PrEP. Thirty-six respondents (75%) perceived some of the patients they served would benefit from PrEP, four (8%) did not and eight (17%) were unsure. Almost half of the respondents had prior experience with PrEP in their work, with 20 (42%) stating they had received at least one question about PrEP in the past year, primarily from MSM (90%) or patients in sero-discordant relationships (70%). Fifteen percent of respondents knew a total of 16 patients that had used PrEP in the previous year, reporting that the drugs were mainly obtained through off-label prescriptions (n = 6) or from a HIV-positive partner/friend (n = 2). Prescriptions were reported to have been written for MSM (n = 5), those in sero-discordant relationships (n = 2) and persons using injection drugs (n = 1).
Respondent characteristics associated with willingness to support pre-exposure prophylaxis (PrEP).
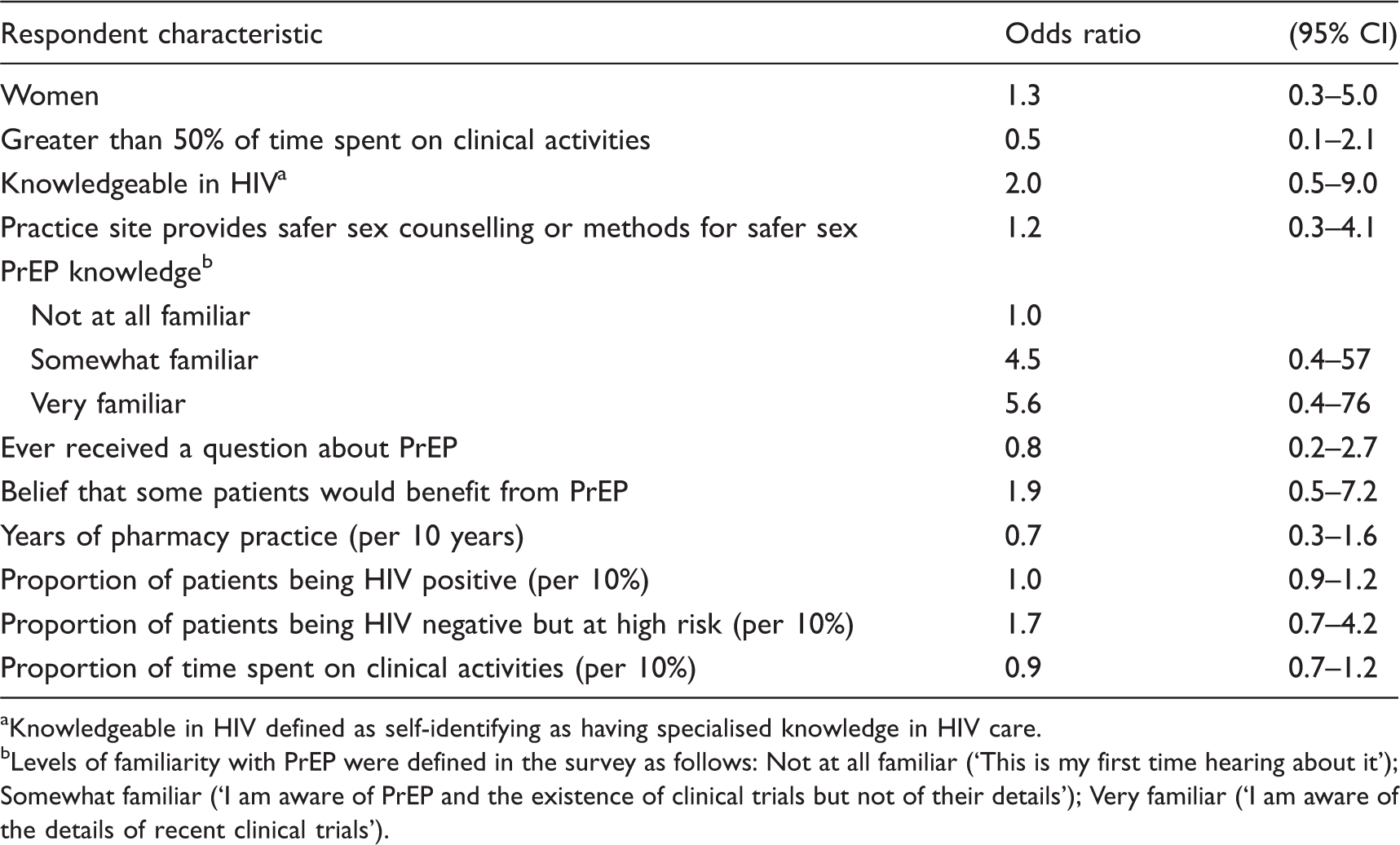
Knowledgeable in HIV defined as self-identifying as having specialised knowledge in HIV care.
Levels of familiarity with PrEP were defined in the survey as follows: Not at all familiar (‘This is my first time hearing about it’); Somewhat familiar (‘I am aware of PrEP and the existence of clinical trials but not of their details’); Very familiar (‘I am aware of the details of recent clinical trials’).
With regard to support for regulatory approval, 26 respondents (54%) considered the level of protection provided by PrEP, as reported from studies available at the time, sufficient for Health Canada to approve PrEP for use in Canada, while seven (15%) did not and 15 (31%) answered ‘maybe’. When further asked to identify the minimum level of HIV prevention efficacy they would consider reasonable for PrEP use to be recommended to high-risk individuals, respondents desired a median (IQR) of 70% (50 to 85%) efficacy, with those supporting PrEP regulatory approval accepting a lower median (IQR) level of protection of 50% (33 to 60%) versus 83% (70 to 95%) among those who answered ‘maybe’ or did not support approval (Wilcoxon p < 0.0001).
Understanding that the medication would cost approximately CAD $830/month, only seven (15%) respondents believed the government (e.g. public drug plans) should provide it without any conditions. Many respondents felt the financial burden of PrEP could be covered by a patient’s private drug insurance (81%), the public drug plan only if criteria such as belonging to a pre-defined high-risk population were met (71%), or by the person requiring PrEP (67%). Also, the majority of participating pharmacists believed there should be some restrictions on who should prescribe PrEP with only 25% in favour of all physicians, regardless of experience, permitted to prescribe PrEP. High levels of support were seen for infectious disease physicians (71%) and all practitioners with HIV or STI care familiarity and prescribing authority, including physicians (83%), nurse practitioners (77%), and pharmacists (71%).
Participants were asked to rank the critical issues to be considered for the implementation of oral PrEP (Figure 1).
Proportion of pharmacists that ranked aspects of PrEP implementation as 1st or 2nd most important.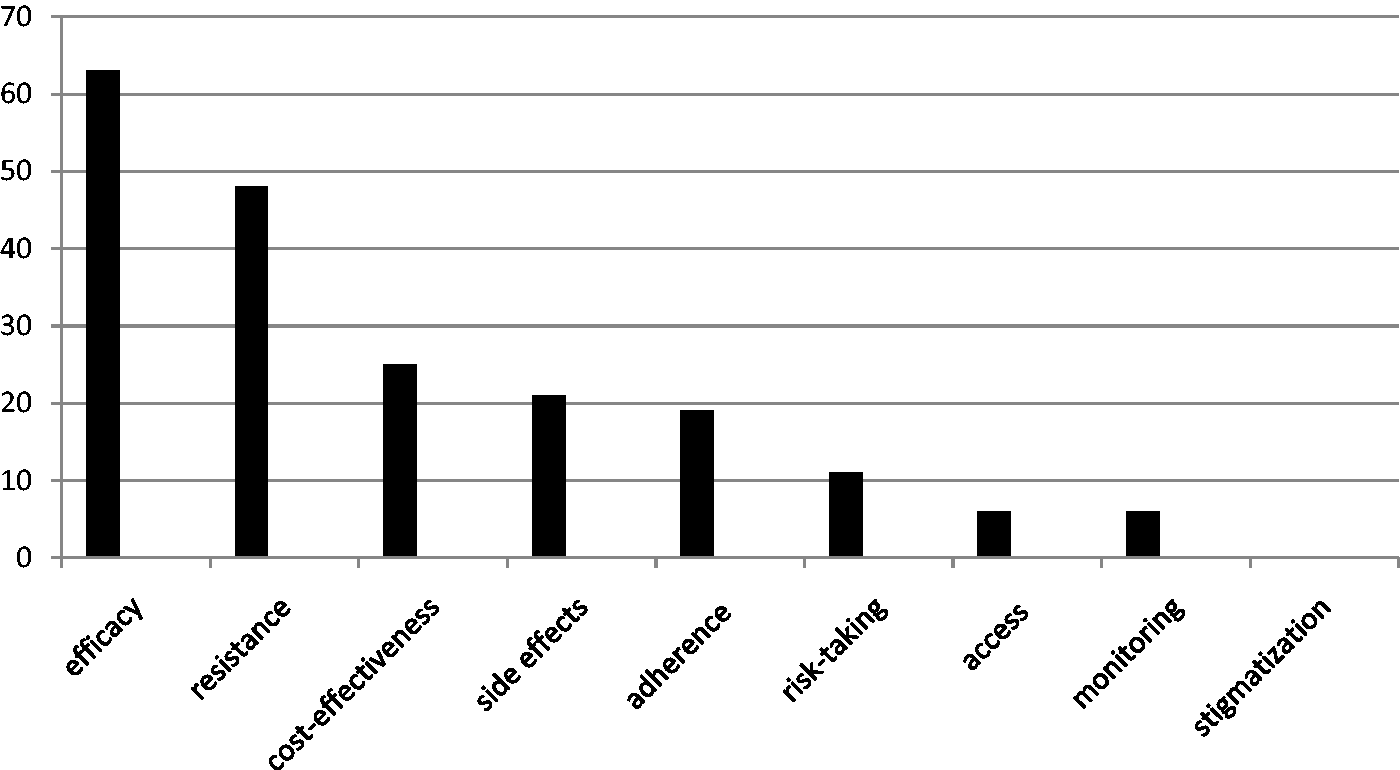
Participants were also asked to rate their levels of agreement with statements on various aspects of PrEP implementation on a five-point Likert scale (Figure 2).
Levels of agreement with statements on PrEP implementation.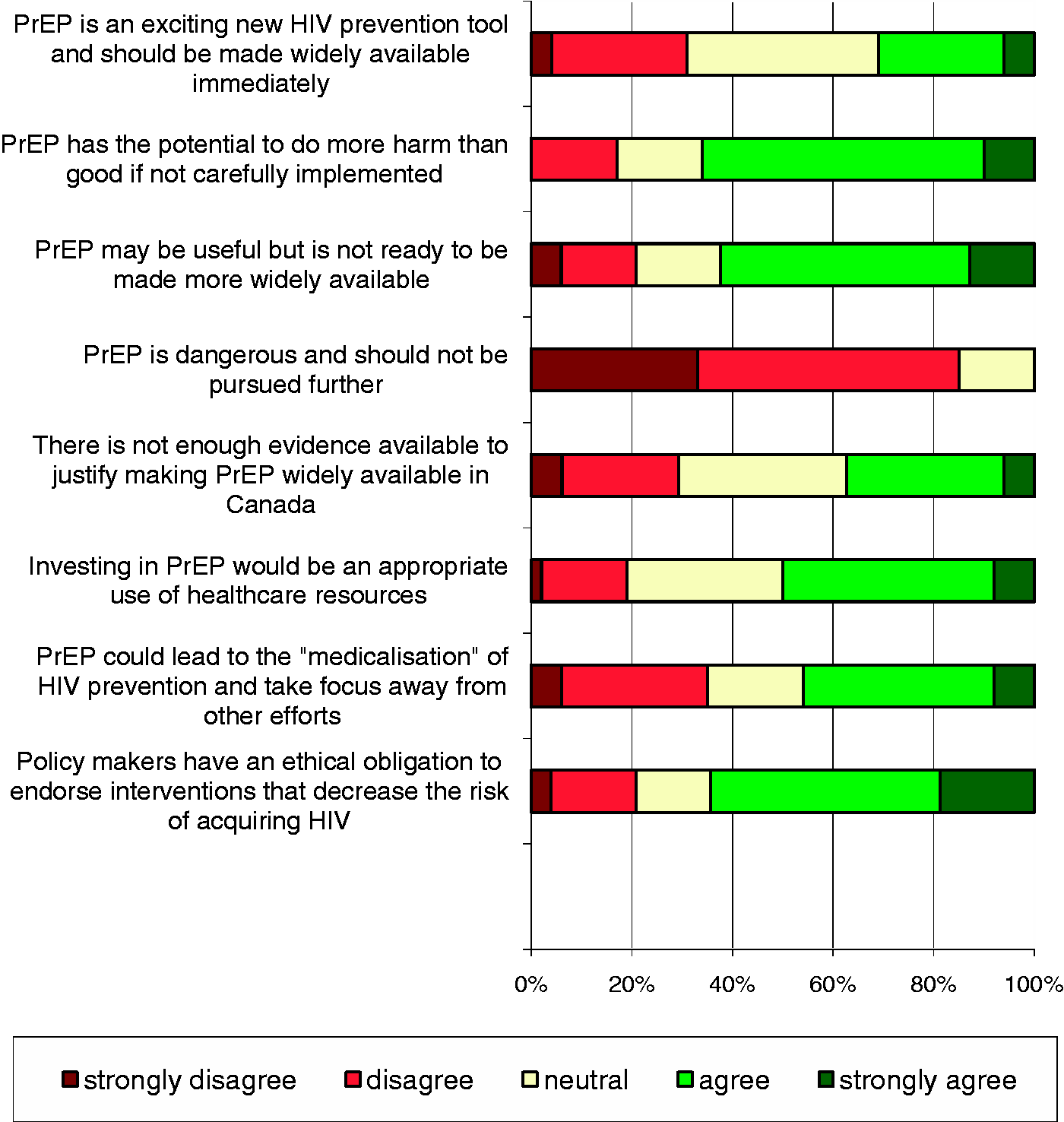
Many (67%) were cautious and agreed that ‘PrEP has the potential to do more harm than good if not carefully implemented’. Before PrEP becomes more widely available, respondents desired more research on its risks (67%) and benefits (65%), affordable drug costs (65%), PrEP-related education of physicians and other healthcare providers (63%), and guidelines on testing and monitoring (54%). Other priorities suggested by individual respondents included additional research in North American populations (n = 1) and further exploration into other biomedical HIV prevention options, including those with more flexible dosing schedules (n = 2).
Current barriers to educating patients about PrEP included drug access (56%), insufficient familiarity with PrEP to provide counselling (31%), lack of clarity regarding which patients would benefit (31%), belief that data are inadequate to support its use (25%), physician colleagues who oppose PrEP thereby rendering education pointless (10%), uneasiness discussing PrEP (8%), and lack of private counselling areas (8%). Patients’ lack of interest and resistance to education from a pharmacist were also identified as barriers (n = 3). No respondent felt educating patients was outside his/her scope of practice. While three pharmacists did not feel they needed any more information, many felt continuing education events or workshops (73%), online learning modules (67%), and access to papers from peer-reviewed medical journals (63%) would be useful in learning more about PrEP.
Respondents agreed that potential opportunities to discuss PrEP with patients include: when providing medication counselling to HIV-positive patients in sero-discordant relationships (85%), when filling a prescription or providing counselling for other STI treatment or prevention methods (60%), including post-exposure prophylaxis (50%), or during any interaction with an identified high-risk individual (6%). In contrast, a small number of respondents did not feel pharmacists should be discussing PrEP (n = 3) or felt a discussion should only occur in a clinic setting (n = 1).
Additional issues were raised in a final open-ended question. PrEP’s inability to prevent transmission of other STIs, including hepatitis C and unplanned pregnancies were highlighted. Also, the possibility that PrEP may reduce the use of other cost-effective methods that are already available was a cited concern.
Discussion
Since pharmacists are trained medication experts, they could play a significant part in PrEP roll-out. Thus, it is important to understand their opinions and learning needs.
Our results suggest that many pharmacists that provide HIV care in Canada have a positive attitude towards PrEP and would be willing to promote PrEP to high-risk patients. However, several aspects of PrEP implementation were identified as warranting additional evaluation. The guarded support seen in our study, as evidenced by the modest level of endorsement for regulatory approval (54%), is consistent with that expressed by other Canadian healthcare and service providers in work by our group.20,21 Indeed, respondents mentioned the same key concerns cited by other knowledgeable groups, including imperfect efficacy, the potential for drug resistance, and cost-effectiveness.8,22–24
Interestingly, 75% of our respondents believed some of the patients they served would benefit from PrEP, yet nearly a third of our respondents (27%) were undecided in their opinion to promote PrEP to a patient at high risk of HIV infection. At the time of our survey, comprehensive PrEP guidelines 25 were not yet available and experiences describing uptake, delivery, or outcomes of PrEP outside of a clinical trial had not yet been reported. 26 It is difficult to speculate if the lack of guidelines or implementation data may have contributed to the hesitant level of support, or if their existence at the time of our study would have provided more reassurance and led to greater support for PrEP.
The top barriers to promoting this prevention method included drug costs/accessibility, unfamiliarity with PrEP data and uncertainty regarding which patients would benefit. It is well-documented that financial constraints contribute to medication access and non-adherence. 27 Across Canada, Truvada® for PrEP use is only available for coverage in Quebec’s public drug insurance formulary. 28 With no immediate plans for regulatory approval of PrEP in Canada, drug costs are likely to remain a major barrier to PrEP's uptake. Similar to the findings in a survey of Florida pharmacists, 19 our results also suggest that filling the knowledge gap even among pharmacists who self-identify as knowledgeable in HIV could increase pharmacists’ willingness and readiness to counsel patients on PrEP. The provision of guidelines that includes clear criteria may help pharmacists identify ideal individuals and maximise the cost-effectiveness of PrEP. 23 Understanding that drug resistance can be minimised if PrEP is withheld in patients with acute HIV infections,3,4,29 pharmacists may also be vigilant in monitoring patients for symptoms consistent with an acute retroviral syndrome. Mobilising informed pharmacists may in turn influence PrEP’s effectiveness as a prevention strategy. If equipping them with essential tools leads more pharmacists to discuss PrEP with patients and assist with adherence counselling and monitoring, patients may be more inclined to take PrEP safely as prescribed. In turn, this may improve efficacy and minimise the development of drug resistance.
Only 40% of our participants were ‘very familiar’ with PrEP-related information despite patient interest in PrEP reported by some respondents. This further suggests the need for more pharmacist education. Surveys have revealed that many men at high risk for HIV acquisition never heard of PrEP.30,31 Among those who were aware, many gained information from newspapers and conversations with friends. 31 Pharmacists should be reliable sources of PrEP information and are uniquely positioned to be an accessible healthcare professional to inform and engage high-risk individuals into care. Additionally, our analysis revealed that patients are obtaining PrEP through informal channels and it is critical that such patients be informed on the proper use of PrEP. Increasing PrEP knowledge is a crucial step in PrEP implementation, which impacts uptake. 26 Future programs should focus on disseminating key research and published guidelines to pharmacists through the media they prefer, including workshops and online learning modules.
Our study has several limitations. First, because our recruitment strategy primarily relied on the memberships of two organisations of pharmacists involved in HIV care, our results may not represent the views of all Canadian pharmacists. Because participation was voluntary, selection bias may have led our survey to over-represent pharmacists with an active interest in PrEP. However, HIV-experienced pharmacists were deliberately selected as they are likely to be involved in the early implementation of PrEP in Canada. Although the response rate was modest (37%), to our knowledge, this is the first survey to capture the perceptions and opinions of pharmacists regarding PrEP in Canada. Second, while we did obtain opinions from across the country, the number of participants in our study precluded more detailed analyses regarding characteristics associated with support for PrEP. Third, although efforts were made to maintain anonymity when capturing data, certain regions of Canada have only a few pharmacists practicing in HIV. It is possible that support for PrEP may have been influenced by a social desirability bias and may not reflect true opinions. Finally, we conducted our study at a time when data on PrEP were still emerging and before clinical practice guidelines on PrEP were widely publicised. As such, respondent opinions on PrEP likely continued to evolve after our survey closed. Indeed, it is noteworthy that a pharmacodynamic model of PrEP efficacy published in late 2012 suggests that PrEP may have 96% HIV prevention efficacy even when taken only four days per week 14 – a result that compares favourably with the minimum level of efficacy desired by those survey respondents who were not in favour of regulatory approval in this study (median 82.5%, IQR 70 to 95%).
Conclusion
PrEP has the ability to prevent HIV transmission and by involving a team of healthcare professionals, success may be maximised. The optimal roles of various healthcare disciplines are yet to be established. Pharmacists can be a valuable asset in this prevention strategy by helping increase awareness and reinforcing PrEP’s proper use in high-risk populations. Many Canadian pharmacists with experience in HIV care seem to have a positive attitude toward PrEP. We found that addressing the cost of medication and providing more PrEP information and training may encourage pharmacists to support PrEP. These findings may be applicable to other settings and should be considered to mobilise more pharmacists globally to promote PrEP as an effective HIV-prevention method.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.