
Abstract
Male-to-female transgender women (TGW) experience high rates of substance use and HIV. A recent substance use trend is the use of prescription medication without a doctor’s consent. No research to date has examined the associations between this non-medical use of prescription drugs and HIV risk behaviour in TGW. In the present study, TGW recruited from community venues (N = 104) in the Mid-Atlantic region of the United States completed surveys assessing demographic information, non-medical use of prescription drugs, other substance use, injection practices and sexual risk behaviour. Twenty-four per cent of the sample reported lifetime non-medical use of prescription drugs across the following categories: analgesics (21.2%), anxiolytics (14.4%), stimulants (12.5%) and sedatives (8.7%). Participants reporting non-medical use of prescription drugs were more likely to report other substance use, needle use to inject drugs, injecting silicone and sharing needles. In multivariable analyses, non-medical use of prescription drugs was associated with unprotected sex, sex after engaging in substance use, and commercial sex work, after controlling for demographic factors. Self-esteem and social support from family served as protective factors for non-medical use of prescription drugs. HIV-prevention programmes focused on TGW in the United States may wish to expand their assessment of substance use to include the use of prescription medications without a physician’s consent.
Keywords
Transgender women (TGW) are individuals classified as male at birth but identifying as female later in life. 1 Probability studies examining HIV prevalence in TGW have not been conducted, despite evidence that TGW are at very high risk for HIV. A recent meta-analysis using data from convenience samples in 15 countries estimated the HIV prevalence in TGW at 19.1% (95% confidence interval: 17.4%–20.7%). 2 A comparable meta-analysis examining HIV prevalence in TGW in the United States (US) found that, in studies conducting HIV testing, 27.7% (95% confidence interval: 24.8–30.6%) tested positive. 3 This review also reported that HIV rates were consistently highest in African-American TGW, relative to other racial groups in the US. Research with TGW shows high rates of sexual risk behaviour, including unprotected sex and sex with multiple partners.4–6 Prior work has also identified commercial sex work (CSW) as a crucial risk factor for HIV infection in TGW. 7 Additional research has documented injection risk behaviours in TGW. 8 In most groups, injection risk is due to the use of illicit drugs. Among TGW, some individuals also inject hormones or inject silicone directly into the body in an effort to change body shape and features. 9 Sharing needles during this process may be an additional HIV risk behaviour for some TGW.
Substance use may represent a method to cope with the discrimination faced by TGW in the United States. 10 High rates of substance use have been found in this group. 11 Excessive substance use is well documented to be associated with sexual risk behaviour. 12 A recent substance use trend in the US is the non-medical use of prescription drugs (NMUPD), the use of medications for managing pain and treating anxiety, attention-deficit disorder and insomnia, without a physician’s prescription. NMUPD has increased in the US and the misuse of prescription drugs has been linked to negative outcomes including dependence and overdose. 13 Although NMUPD appears to have shown the largest increases in North America, 14 some studies in Europe and Australia also show concerning rates of this behaviour.15,16
A few studies have examined relationships between NMUPD and HIV risk behaviour in populations at high risk for HIV. Benotsch et al. found associations between NMUPD and sexual risk behaviour in men who have sex with men (MSM) in Denver, CO (US). 17 Kelly and Parsons found associations between NMUPD and unprotected sex in HIV-negative MSM in New York, NY (US). 18 In a study of opioid abusers, Surratt et al. found that 23.8% reported injecting prescription analgesics and some participants reported sharing needles. 19
Some prior studies have examined resiliency factors as protective factors that reduce the likelihood of engaging in NMUPD.20,21 Given that TGW face considerable stigma, examining resiliency factors may be especially important in this group.
Prior work has not examined associations between NMUPD and HIV risk behaviour in TGW. The present analysis is from a larger study of substance use in transgender adults. 22 Here, we describe analyses specific to HIV risk behaviours in the TGW subset of the larger study. We hypothesised that NMUPD would be associated with sexual and injection HIV transmission risk behaviours. We also hypothesised that resiliency factors (self-esteem, social support) would be protective against engaging in NMUPD.
Methods
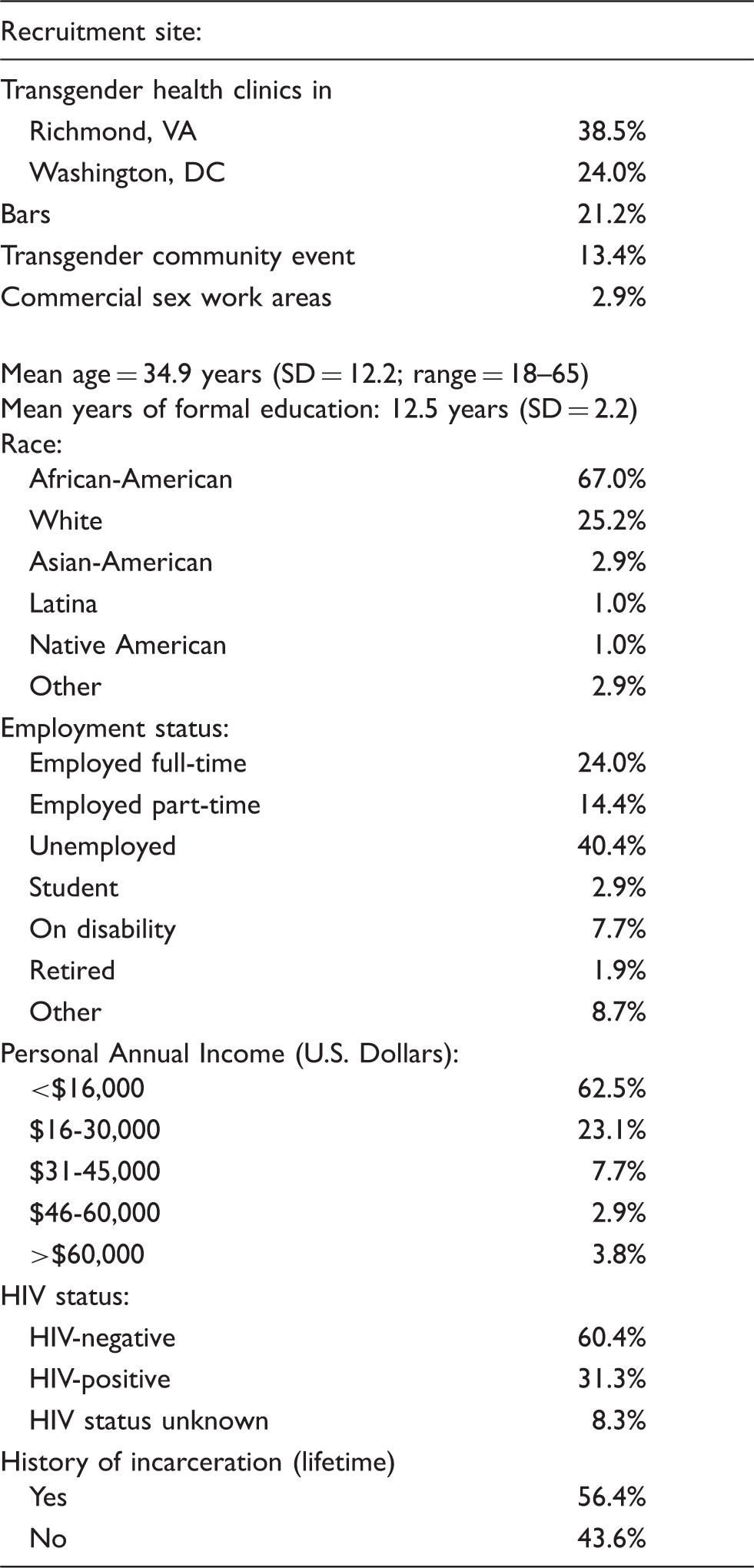
Recruitment sites and characteristics of transgender women in the study sample.
Demographics
Participants were asked to report their age, birth gender, current gender, race/ethnicity, education, employment status and HIV status. Participants also indicated if they had been in jail (lifetime).
NMUPD
Participants were asked to respond with a Yes/No to the question: ‘In your lifetime, have you ever used a prescription medication WITHOUT a doctor’s prescription recreationally – for example, to get high, or because you were curious, or to try something new?’ Participants then indicated their lifetime NMUPD in four categories: analgesics (e.g. Vicodin), sedatives (e.g. Ambien), anxiolytics (e.g. Xanax) and stimulants (e.g. Adderall). Examples of medications in each category were listed on the survey. This measure has been used previously. 17
Other substance use
Participants were asked about alcohol and illicit drug use in the previous three months. Participants also indicated if they had ever used a needle to inject drugs, hormones, or silicone and if they had ever shared needles. This measure is similar to measures employed previously. 23
Sexual practices
Participants were asked to report the number of times they had engaged in unprotected anal and vaginal intercourse in the past three months. Participants also recorded their number of sexual partners in the past three months. In addition, participants indicated if they had exchanged sex for money, drugs, or a place to stay in their lifetime and in the past three months. Participants were also asked the number of times they had had sex after having ‘too much’ to drink, and the number of times they had had sex after using drugs in the previous three months. In addition, participants indicated if they use condoms the first time they have sex with a new partner and if they find out about a partner’s HIV status before having sex. These items were rated on a 4-point scale from 1 (Never) to 4 (Always).
Resilience factors
Self-esteem was assessed with a shortened version of the Rosenberg scale. This measure had adequate internal consistency within this sample (α = .77) and has shown good test–retest reliability in a variety of populations, including those at high risk for HIV. 24
Social support was assessed with a shortened version of the multidimensional scale of perceived social support. 25 This instrument separately measures social support provided by members of an individual’s family of origin and support provided by friends. The measure had excellent internal consistency for both the family support scale (α = .94) and the friends support scale (α = .93).
Data quality assurances and statistical analyses
All surveys were examined for inconsistencies and invalid responses. Missing data were omitted from analyses, resulting in slightly different sample sizes for various statistical tests. Distributions of substance use and sexual behaviour were highly skewed so non-parametric analyses were used. Because many factors can be associated with substance use and sexual risk behaviour, multivariable analyses were used to examine associations between NMUPD and sexual risk, after controlling for the influence of demographic factors. Comparable multivariable analyses examined the role of resiliency factors in protecting against NMUPD.
Results
Participants
As shown in Table 1, participants were predominantly African-American, with modest educational attainment and income.
NMUPD
Almost a quarter of the sample (24.0%) reported lifetime NMUPD. The most commonly used type of medication was analgesics (21.2% of the sample), followed by anxiolytics (14.4%), stimulants (12.5%) and sedatives (8.7%). Participants who reported NMUPD were significantly more likely to report being HIV positive (52.0%) than individuals who did not report NMUPD (23.9%), χ2 (1, N = 96) = 6.47, p < .05. Participants who reported NMUPD were also more likely to report having been in jail in their lifetime (79.2%) than participants not reporting NMUPD (49.4%), χ2 (1, N = 101) = 7.04, p < .01. NMUPD was unrelated to other demographic factors assessed.
NMUPD, other substance use and injection practices
Non-medical use of prescription drugs, other substance use, and injection risk behaviours in a sample of transgender women in Richmond, VA and Washington, DC, USA.
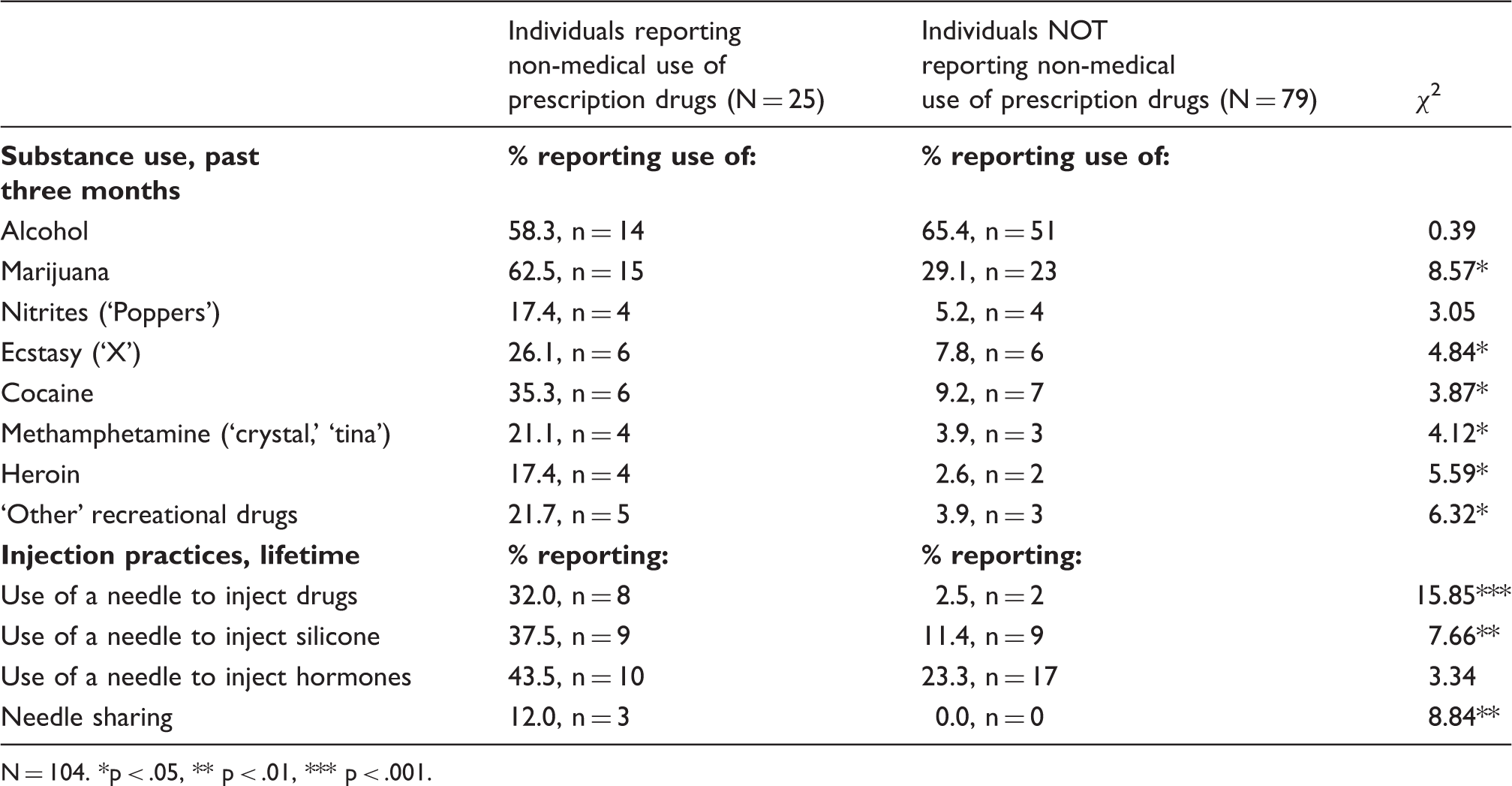
N = 104. *p < .05, ** p < .01, *** p < .001.
NMUPD and sexual risk behaviour
Non-medical use of prescription drugs and sexual behaviour in a sample of transgender women in Richmond, VA and Washington, DC, USA.
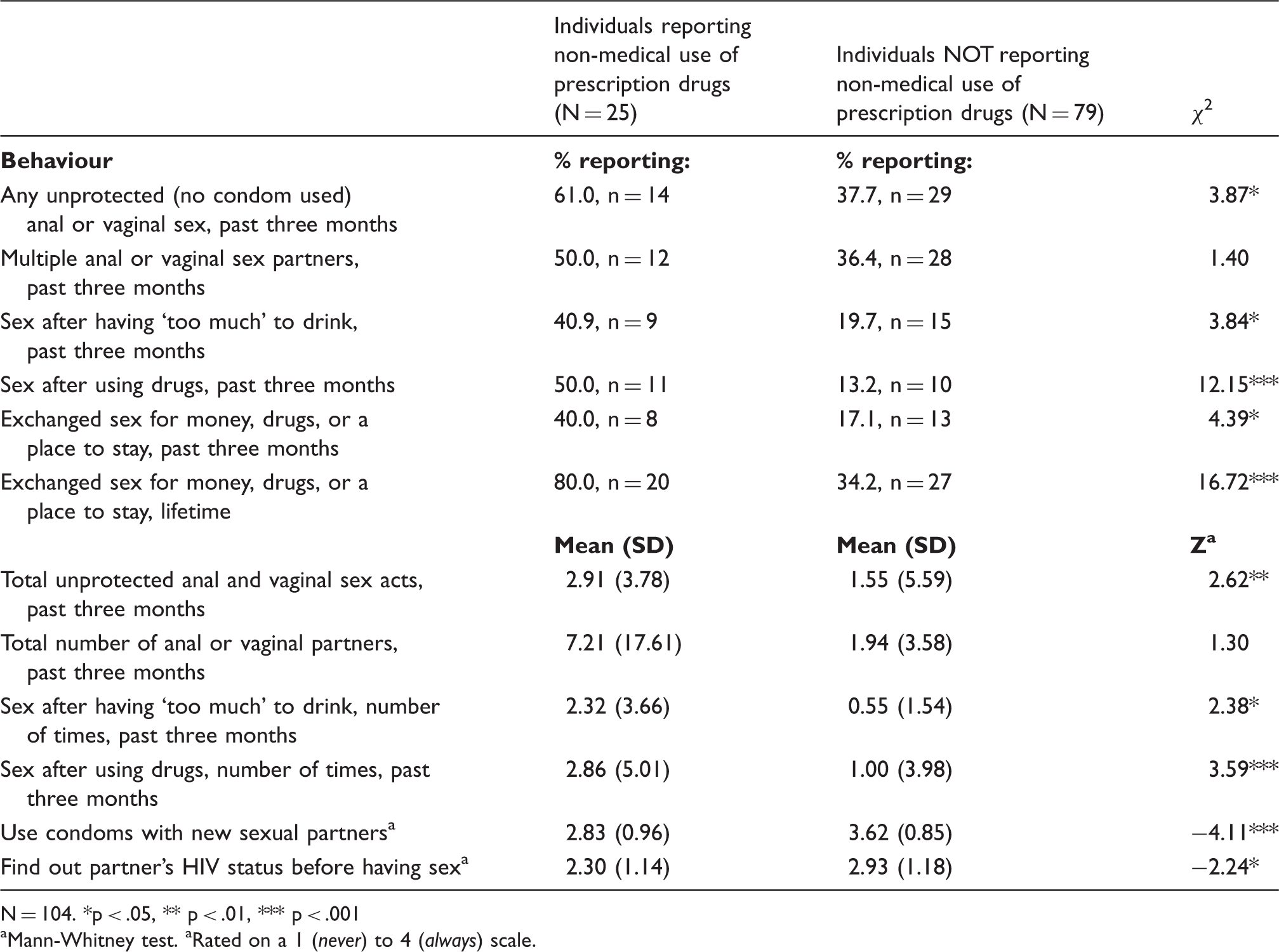
N = 104. *p < .05, ** p < .01, *** p < .001
Mann-Whitney test. aRated on a 1 (never) to 4 (always) scale.
Non-medical use of prescription drugs and sexual risk behaviour in a sample of transgender women in Richmond, VA and Washington, DC, USA.
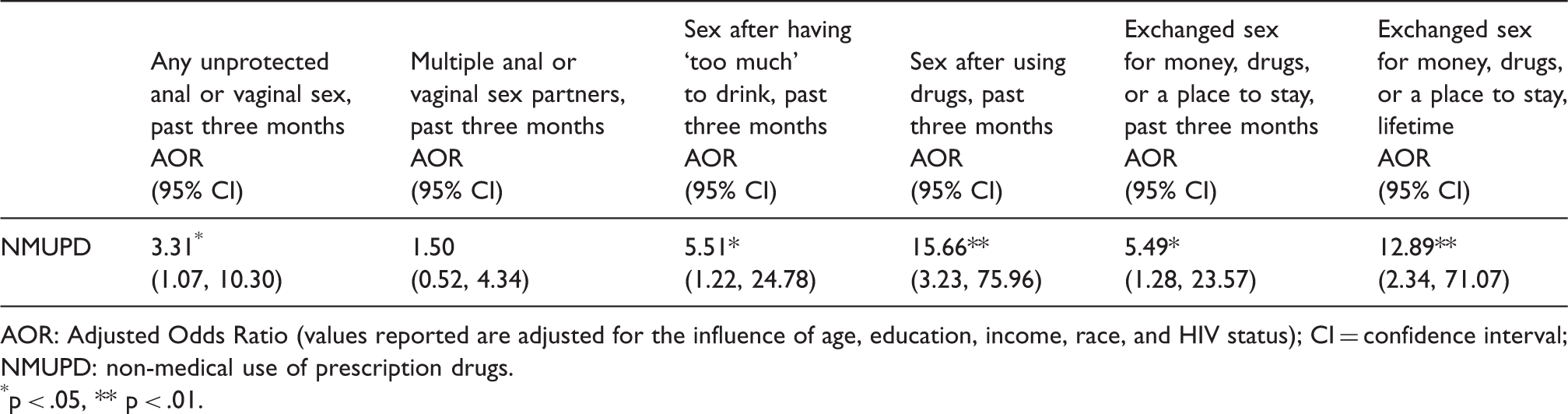
AOR: Adjusted Odds Ratio (values reported are adjusted for the influence of age, education, income, race, and HIV status); CI = confidence interval; NMUPD: non-medical use of prescription drugs.
p < .05, ** p < .01.
Resiliency factors
Non-medical use of prescription drugs and resiliency factors in a sample of transgender women in Richmond, VA and Washington, DC, USA.
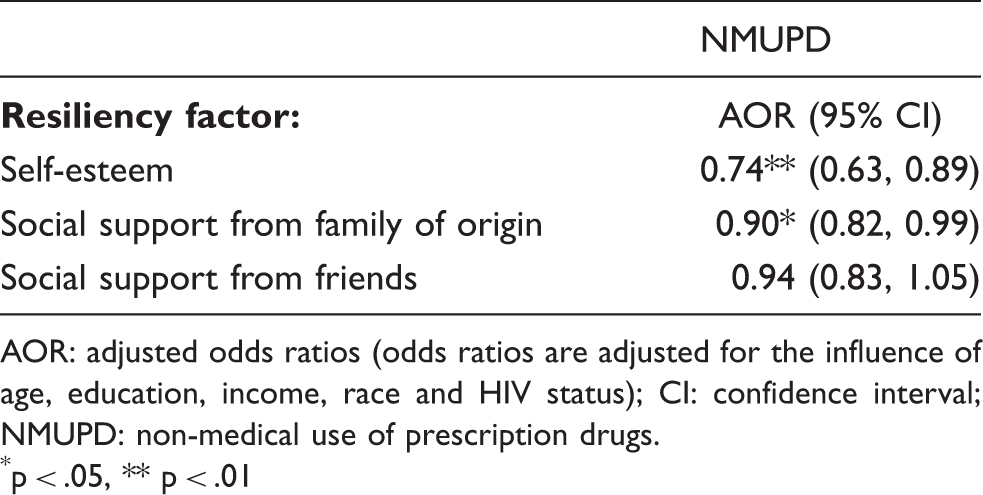
AOR: adjusted odds ratios (odds ratios are adjusted for the influence of age, education, income, race and HIV status); CI: confidence interval; NMUPD: non-medical use of prescription drugs.
p < .05, ** p < .01
Discussion
In this study, nearly one in four TGW reported lifetime NMUPD. These findings are consistent with increasing NMUPD prevalence in other groups in North America. As with other studies, NMUPD was associated with the use of illicit drugs.17,19 It may be more appropriate to consider NMUPD in the context of a polysubstance use pattern. Using prescription medications with illicit drugs can have adverse effects, including death. 13 TGW may be especially vulnerable to deleterious effects of the combined use of illicit drugs, prescription drugs used non-medically, as well as prescription drugs that are prescribed by a physician (e.g. hormone therapy, antiretrovirals).
NMUPD was also associated with both sexual and injection-related HIV transmission risk, including CSW, a crucial risk factor for HIV acquisition in TGW. 26 In prior work, TGW engaged in CSW reported the use of illicit substances to cope with the stress of that activity. 27 Previous research has documented stress-reduction motivations for NMUPD, and NMUPD appears higher in individuals who have experienced sexual trauma. 28 Use of these medications among TGW may reflect an attempt to cope with the stress of CSW. For some of these medications (e.g. anxiolytics), reducing stress-related symptoms is consistent with how they might be prescribed. TGW frequently report poor access to culturally sensitive medical care. 29 We specifically assessed recreational use; however, it may be that these medications were being used without a physician’s prescription because that is the only option available to them. Having high self-esteem and high social support from family were protective factors for NMUPD, perhaps by buffering individuals from the effects of stigma and other stressors. 30
Lifetime reports of injecting drugs (10%), silicone (17%) and hormones (27%) were also high. Risks associated with injecting illicit drugs are well established. TGW face additional risks associated with injecting silicone, which is seen as a rapid method of feminising body parts. 31 Consequences of silicone injection can include acute infection and pulmonary dysfunction leading to death. 32 Injecting silicone and drugs was associated with NMUPD. To our knowledge, this is the first study that documents associations between NMUPD and injection risk behaviours in TGW.
Limitations and conclusion
These data were collected from a relatively small (N = 104) convenience sample of TGW in the Mid-Atlantic region of the US. The study population was predominantly African-American and had low incomes and high rates of unemployment; generalisation to other regions and populations may not be warranted. The use of a cross-sectional design limits drawing causal conclusions. We assessed the use of broad classes of medication (e.g. analgesics) but did not separately assess the use of specific medications (e.g. Vicodin) and only assessed lifetime NMUPD. Future work should assess the non-medical use of specific medications within each class as well as assessing NMUPD over more recent time frames. In addition, a more detailed assessment of sexual behaviour (e.g. separately assessing insertive/receptive anal sex) is warranted.
Despite these limitations, this study provides additional information about patterns of substance use in TGW and is the first to document associations between NMUPD and HIV risk behaviour in this group. Given that almost 1/3 of the sample reported being HIV positive, the associations between NMUPD and behaviour include increased risk for both the transmission and acquisition of the virus. This study is also one of the first quantitative studies to link NMUPD and injection risk behaviours. HIV-prevention programmes focused on TGW may wish to expand their assessment of substance use to include NMUPD. If validated through additional research, these results may indicate the need for specialised interventions to be made available that incorporate HIV prevention and substance use treatment. Given the high rates of unemployment, low incomes, and engagement in CSW, organisations working with TGW may also wish to include job training as part of a comprehensive risk reduction intervention. Comprehensive HIV-prevention programmes should also focus on HIV testing (8.3% of participants in this high-risk group reported not knowing their HIV status) and linkage to care.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by internal institutional grants to the first and second author.