
Abstract
Summary
Reactive arthritis is an under-studied complication of genital Chlamydia trachomatis infection (chlamydia). We assessed trends and risk factors for reactive arthritis in a large urban sexual health clinic. Using a case-control design, data on reactive arthritis cases and controls at the Sydney Sexual Health Centre over the period 1992–2012 were extracted and multivariate analyses were performed. Trend analyses were performed on reactive arthritis diagnoses. Over the 1992–2012 study period, 85 reactive arthritis cases were diagnosed at Sydney Sexual Health Centre. The rate of reactive arthritis diagnoses decreased over time (23 in 1992–1996 to one in 2007–2011 and none in 2012), while chlamydia diagnoses increased (770 in 1992–1996 to 2257 in 2007–2011). In multivariate analysis, factors independently associated with a reactive arthritis diagnosis were: being male (adjusted odds ratio [aOR] 3.27; 95% confidence interval [CI] 1.04–10.32; p = 0.043) or born overseas (aOR 2.69; 95% CI 1.27–5.70; p = 0.010), while a past sexually transmitted infection other than chlamydia or non-gonococcal urethritis was protective (aOR 0.21; 95% CI 0.10–0.45; p < 0.001). Reactive arthritis was not associated with current or recent chlamydia infection (p = 0.184) but was marginally associated with past non-gonococcal urethritis (p = 0.080). This study found a decline in reactive arthritis diagnoses despite an increase in chlamydia diagnoses.
Keywords
Introduction
Reactive arthritis (ReA) is a potential complication of genital Chlamydia trachomatis infection (chlamydia). 1 Increasing diagnoses over the past 20 years have made chlamydia the most common notifiable infection in Australia, with an age-standardised notification rate of 345.8/100,000 in 2012. 2 While there is some correlation between increased rates of chlamydia testing and increased notifications, there is also evidence of an underlying rise in prevalence. 3 However, chlamydia testing rates remain low, especially in young populations where <10% get tested for chlamydia annually. 3 The populations with the highest prevalence of chlamydia in Australia are people under 25 years of age, Aboriginal and Torres Strait Islander people, and men who have sex with men (MSM). 2
Potential complications of chlamydia include pelvic inflammatory disease (PID), tubal factor infertility, chronic pelvic pain, ectopic pregnancy, epididymo-orchitis, ReA and perihepatitis. 4 Despite an increase in chlamydia notifications, rates of many chlamydia-related complications have been shown to be either stable or decreasing across hospital and primary care settings in Australia and elsewhere. Hospital admission rates for PID in New South Wales (NSW) decreased between 1992 and 2001 4 and PID encounters in general practice fell significantly between 1998 and 2003. 5 A similar decrease in PID consultations in primary care has been observed in the UK. 6 In the US, chlamydia screening has been correlated with a decrease seen in PID; however, the effectiveness of screening remains uncertain. 7 Hospital admissions for epididymo-orchitis have not significantly changed over time in Australia, 5 and stable rates have been reported in primary care in the UK. 8 Hospital admission rates for ectopic pregnancy and female infertility have remained stable or decreased in NSW.9,10
ReA is a possible complication of chlamydia 1 ; however, trends in the rates of ReA have not been studied. A recent review suggests an anecdotal decline in cases seen in the UK; 11 however, no data currently exist to substantiate this. The term ReA traditionally describes a sterile arthritis and mucocutaneous lesions, which occurs as a consequence of prior enteric or genital infection. 12 When ReA is preceded by an enteric infection, the most common causative organisms are of the Shigella, Yersinia, Campylobacter and Salmonella species. ReA attributable to sexually-acquired Shigella sonnei was previously reported from the Sydney Sexual Health Centre (SSHC). 13 C. trachomatis is commonly associated with sexually-acquired ReA, with nucleic acid amplification testing (NAAT) identifying the organism in 35–69% of cases. 14 However, its exact role is contentious. 11 Although Neisseria gonorrhoeae has been linked to up to 16% of cases, and described in concomitant chlamydia and gonorrhoea cases, 15 its role in ReA remains unclear. A minority of ReA cases may be linked to Ureaplasma urealyticum and Chlamydia pneumoniae. 14
The triad of arthritis, urethritis and conjunctivitis is often considered to be the classical presentation of ReA. 16 However, facets of this syndrome may also occur individually or non-concurrently, resulting in under-diagnosis. Patients may also experience a spectrum of clinical manifestations including prostatitis, enthesitis, uveitis, keratoderma blennorrhagicum, circinate balanitis, nail dystrophy, mucosal lesions and more rarely, cardiac or neurological manifestations. 17 Rheumatologists typically regard arthritis as a prerequisite for the diagnosis of ReA. However, in non-rheumatological settings, combinations of other symptoms and signs may be seen as sufficiently specific to make the diagnosis in the absence of arthritis. 18
Estimates of ReA following chlamydial infection range from 1% 16 to up to 15%, 19 but generally are around 5%. 1 In a sexual health clinic in Alabama, 4% of patients with chlamydia reported objective features of ReA; 12 however, no control group was used to determine association of the two conditions. Data from Sweden indicated that rates of ReA were higher than rates of rheumatoid arthritis, 20 suggesting that ReA may represent a significant, yet potentially under recognised, burden on the health care system. However, it has been suggested that Scandinavian countries report higher rates of ReA due to less restrictive diagnostic criteria. 21
Diagnostic criteria from the American College of Rheumatology (1981) and the Third International Workshop on Reactive Arthritis (1995) are: ‘the presence of a peripheral arthritis occurring concurrently with urethritis or cervicitis’ and ‘peripheral arthritis with sacroiliac involvement and preceding gastrointestinal or genital infection’, respectively.22,23 However, reliance on a preceding infection becomes problematic as up to 90% of chlamydia cases may be asymptomatic, 3 leading to under-diagnosis or misdiagnosis of ReA. 1 Furthermore, in some primary care settings such as SSHC, information on previous gastrointestinal infection may not routinely be elicited. Difficulties with these diagnostic criteria have been raised, and there remain many points of contention. 24 As a result of these issues with current diagnostic criteria and the under-diagnosis of ReA, it is difficult to perform accurate epidemiological studies.
The aims of this study were to describe diagnosis rates of ReA over a 20-year period in a large urban sexual health centre and to determine factors associated with the diagnosis of ReA.
Methods
Study design and population
We conducted a retrospective case control study to determine risk factors for ReA in patients seen at SSHC, located in central Sydney, Australia. Trends analyses were also performed. Detailed demographic, behavioural, testing and morbidity data for all patients have been collected since 1991. These variables are checked for accuracy and completeness before being entered into a computerised database.
Data for ReA patients were accessed from January 1992 until December 2012. To be included, cases had to have been seen at least once during the study period at SSHC, with a primary reason for their visit being identified and coded as ReA by the treating physician. Cases were identified by their diagnostic code as entered into the database. Both patients with ReA first diagnosed at SSHC and elsewhere were included in the study. Patient files were then reviewed manually and those with a history of two or more specific symptoms or signs of ReA were included, to allow for inclusion of milder presentations seen in a primary care setting.
Controls were the next patient seen by the same practitioner on the day that the case was first coded as ReA. Where this was not possible (for example, the case was seen during the last appointment of the day, or where an individual appeared twice in the control group), controls were randomly selected as any patient seen on the same day at SSHC. New patients were routinely tested for chlamydia throughout the study period, though this was by enzyme immunoassay of first-void urine in men up to 1996 and cell culture of an endocervical swab in women up to 1995; thereafter, nucleic acid amplification testing (polymerase chain reaction [PCR]) was used.
The variables collected for both cases and controls included age, sex, country of birth, gender of sexual partners in the last 12 months, HIV status and history of sexually transmitted infection (STI). Further data were collected for cases regarding the history and nature of ReA symptoms and signs, including date and place of diagnosis, time between STI and ReA onset, symptom duration, affected joints, human leukocyte antigen (HLA-B27) status, history of enteric infections and other symptoms of ReA. Data on the number of chlamydia diagnoses between 1992 and 2012 were also extracted.
Statistical analyses
Diagnosis rates of ReA and chlamydia were calculated with crude numbers per year and due to the small number of ReA cases, time periods were broken into five-year blocks.
Logistic regression was used to assess the factors associated with the development of ReA. Variables with a p-value < 0.1 in the univariate analysis were included in the multivariate analysis. Backward elimination methods were used. Odds ratios and 95% confidence intervals (CI) were calculated. P-values < 0.05 were considered statistically significant.
Data analysis was conducted using Stata 12 (StataCorp, College Station, TX, USA).
Ethics approval was granted by South Eastern Sydney Local Health District HREC (ref no: 08/223).
Results
A total of 85 ReA cases were identified between 1992 and 2012 (Figure 1); 13 patients were excluded from the diagnosis rate calculation because they were diagnosed before the study period (n = 11) or had unknown dates of diagnosis (n = 2). Many of these patients had been previously diagnosed by rheumatologists or were referred on to rheumatologists. However, these patients were included in all other analyses.
Reactive arthritis cases diagnosed at the Sydney Sexual health Centre, 1992–2011.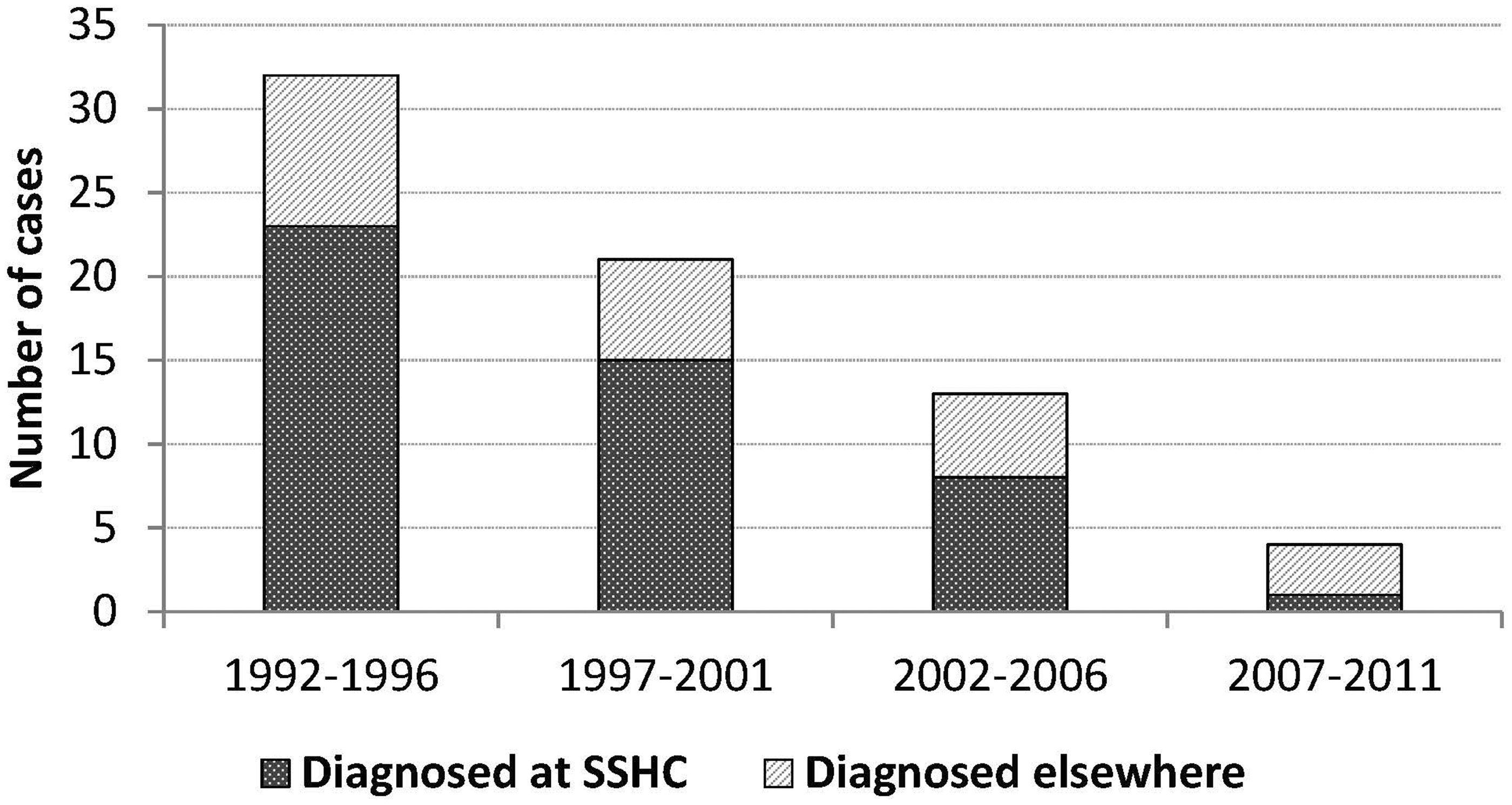
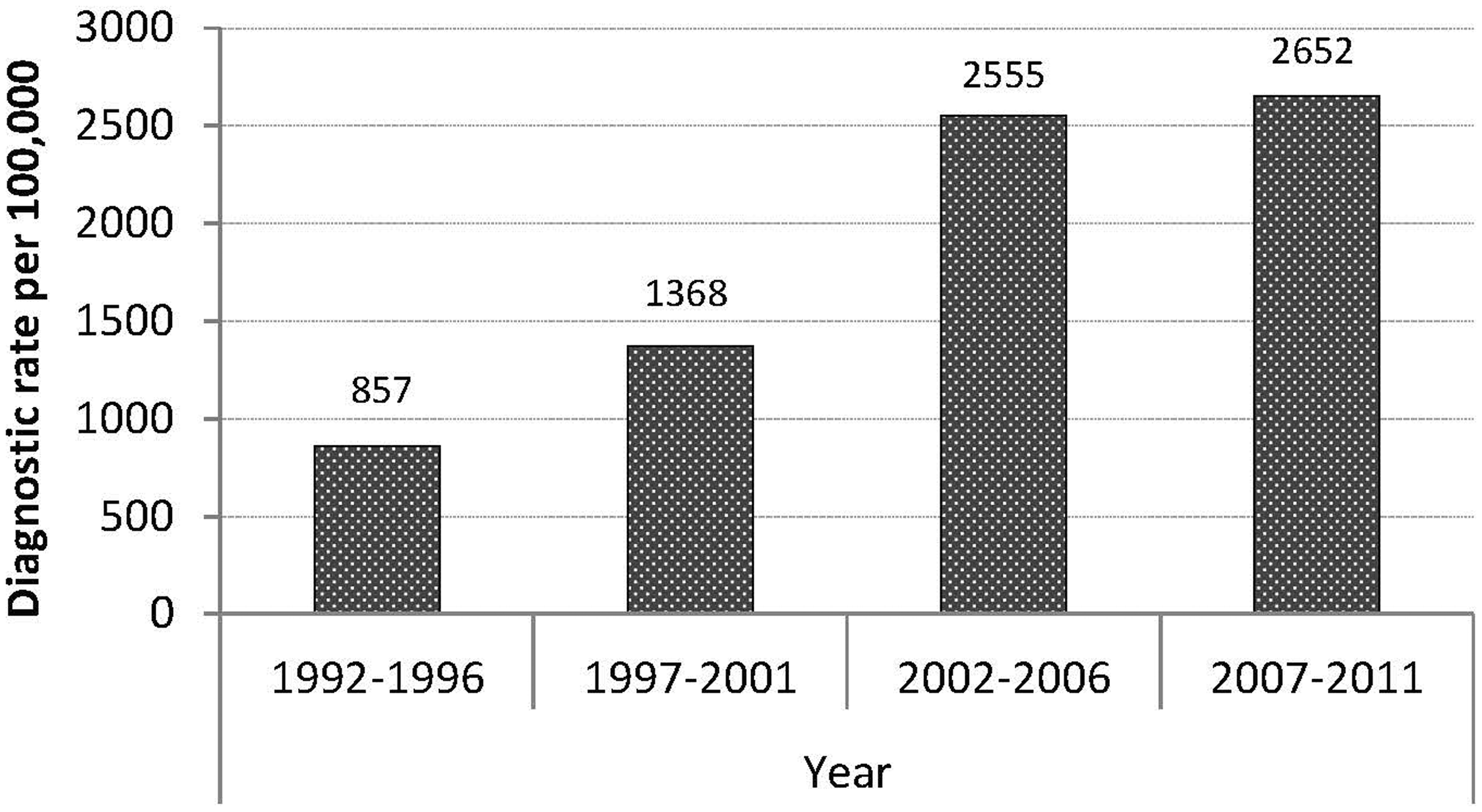
The ReA diagnosis rate at SSHC decreased over time; from a rate of 113 diagnoses per 100,000 patients in 1992–1996 to 13 diagnoses per 100,000 patients in 2007–2011 (Figure 2). By contrast, the diagnostic rate of chlamydia at SSHC rose dramatically over the same time period (Figure 3), mirroring the rising incidence of chlamydia in Australia.
Diagnostic rates of reactive arthritis at the Sydney Sexual Health Centre, 1992–2011. Diagnostic rates of chlamydia at the Sydney sexual Health Centre, 1992–2011.
Characteristics of reactive arthritis cases (n = 85).
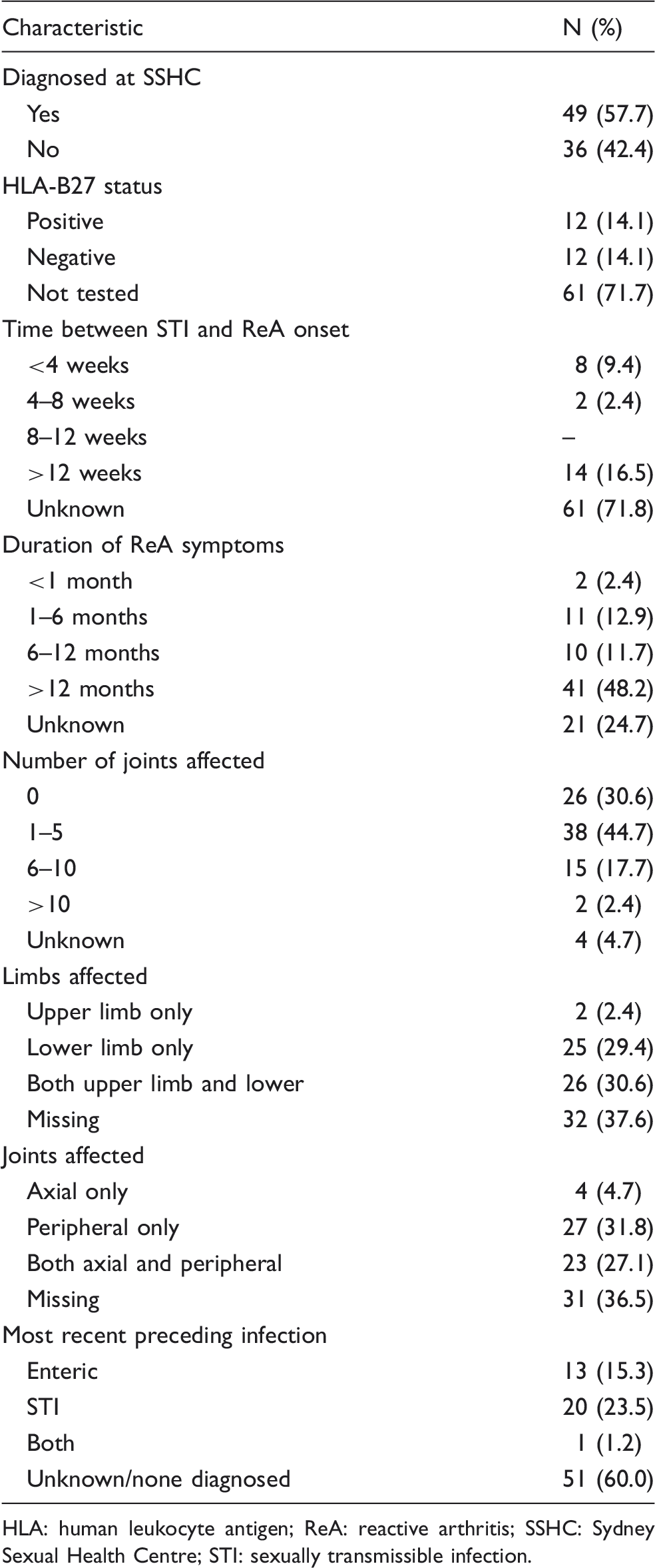
HLA: human leukocyte antigen; ReA: reactive arthritis; SSHC: Sydney Sexual Health Centre; STI: sexually transmissible infection.
The only ReA case diagnosed at SSHC during 2007–2011 was a male with advanced HIV infection who developed severe deforming arthropathy involving >20 joints, nail dystrophy and keratoderma blennorrhagicum following a brisk immune reconstitution after beginning anti-retroviral therapy for HIV infection. He had been treated for chlamydia a few months earlier.
Risk factors for the diagnosis of reactive arthritis.
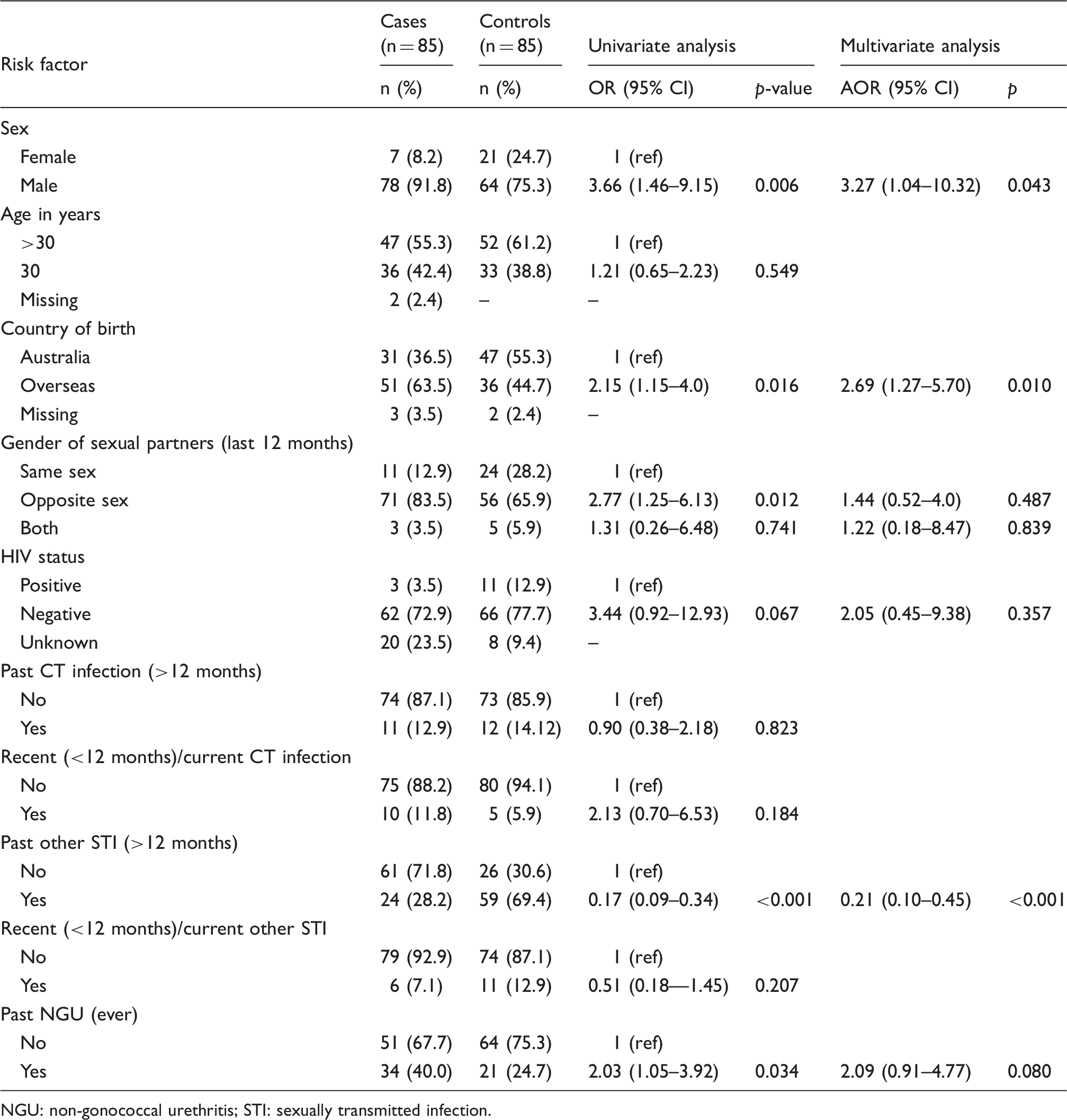
NGU: non-gonococcal urethritis; STI: sexually transmitted infection.
Discussion
In this first case-control study of ReA in a primary care setting in Australia, we found a 10-fold decline in the diagnosis rates of ReA over a 20-year period. Being based in a primary care setting, this study allows exploration of trends and risk factors in milder presentations of ReA, rather than the more severe presentations seen in specialist rheumatology practice. 12 This study contributes to the body of evidence that chlamydial complications are decreasing or remaining stable in the face of increasing chlamydia notifications. This study suggests that those most likely to develop ReA were either male or born overseas or were somehow protected by a past infection with an STI other than chlamydia or NGU.
The reason for this apparent disconnect between chlamydia and its complications is unknown. There are some data which suggest antibiotic use and early treatment of chlamydia may reduce the risk of developing ReA.25,11 However, as <10% of young Australians are tested for chlamydia each year 4 it seems likely that most infections go undiagnosed and untreated. There is still much about the complex pathogenesis of ReA that is poorly understood and requires further research. 11 Any trend that is limited to a single primary care service should always be regarded as preliminary evidence only.
In this study, 50% (12/24) of cases tested were HLA-B27 positive; however, as the total number tested was small, this may not be representative of the total sample. Although a known risk factor in the development of spondyloarthropathies, the role of HLA-B27 in the development of ReA is not well defined. The majority of studies report the prevalence of HLA-B27 in ReA patients as being between 30% and 50%. 1 An ethnic bias is reported in terms of genetic distribution of HLA-B27, with its presence reported in around 6–8% of the Caucasian population and 2% in the African-American population. 16 ReA is more commonly diagnosed among populations with a higher rate of HLA-B27 presence. Within our study population, those with ReA were significantly more likely to be born overseas than those in the control group (OR 2.69; 95% CI 1.27–5.70; p = 0.010). It is possible that this could reflect ethnic differences in HLA-B27 carriage. Alternatively, overseas-born patients may have had less access to alternative health service options such as rheumatologists (difficult and expensive to access), sports physicians (increasing in number during the study period) and general practitioners. Sexual health services in Australia are free at the point of care. Or overseas-born patients may have been at higher risk of exposure to enteric causative agents.
ReA is consistently more commonly diagnosed in men than women, with the male to female ratio typically being reported at around 9:1. 26 Our data also reflect this gender bias, as 91.8% (78/85) of the ReA cases were male. However, common ReA-related signs such as urethritis and circinate mucocutaneous lesions (usually balanitis) are more readily diagnosed in men, leaving all ReA studies open to gender bias. In our clinic population, having partners of the opposite sex only was more common among cases when using univariate analysis; however, this result failed to reach statistical significance in multivariate analysis. As other case-control studies tend to focus on genetic factors influencing disease development, rather than behavioural and demographic data, there is limited literature on this subject. Prior studies of ReA in urban STI clinics in the USA and UK did not report on gender of sexual partners.12,18 While early case reports in the 1980s suggested that ReA occurred more commonly in HIV-positive populations, 27 this study showed no association between HIV and ReA. Several large cohort studies reported no difference in incidence of ReA between HIV-positive and HIV-negative men.28,29 It has been suggested that associations may be due to the sexual behaviour of populations classified as high risk for contracting HIV. 29 However, it has been suggested that immune reconstitution following anti-retroviral therapy initiation may cause a sudden and severe clinical presentation of ReA, 30 which did occur in one case in our study. Interestingly, a history of past STI other than chlamydia and NGU was protective for ReA (aOR, 0.21; 95% CI = 0.10–0.45; p < 0.001). It is possible this may relate to the genetic pre-disposition to develop ReA, as we may expect disease expression to occur with the first few episodes of STI (as a surrogate measure of risk of chlamydia). That is, people with past STI may have passed their time of greatest risk.
This study suggests considerable chronic morbidity due to ReA even in a primary care setting. Almost half (48.2%) of the cases experienced one or more symptoms of ReA lasting more than 12 months, and 10 patients (11.7%) experienced symptoms lasting between six and 12 months. This estimate is slightly higher than previous reports, which suggested between 30 and 50% of cases have symptoms lasting more than six months. 1
Of interest, 30.6% of patients reported no arthritic symptoms, reflecting that not all patients diagnosed with ReA present with the classical clinical ‘triad’, as reported by others in sexual health service settings. 18 Moreover, ReA diagnoses based on both mucocutaneous lesions and arthritis dissipated during the study period. That said, the absence of rigorously applied diagnostic criteria in the context of a regular turnover of doctors is a limitation of this study. Many of those reporting arthritic symptoms (44.7% of patients) experienced arthritis in fewer than five joints. This probably reflects the less severe nature of the disease in those who present in primary care. A relatively large number of patients (18.8%) presenting to the sexual health service reported a recent history of gut infection.
The strength of our study was the long time period of analysis; however, the small sample size and retrospective study design are limitations. Retrospective bias due to missing data, inconsistencies in the recording of patient details and information collected may affect results. Case ascertainment can also be problematic in retrospective analyses. As the records were located using a diagnostic code in this study, it is possible that cases may have been missed due to incorrect coding by the treating clinician. Selecting controls from the same database at the same centre ensured that both the cases and controls were drawn from the same population. Another limitation of our study was that urine PCR testing for chlamydia was not available for men at SSHC until 1997. Thus, chlamydia diagnoses may have been missed due to the use of less sensitive tests such as enzyme-linked immunosorbent assay or culture. As a large proportion of ReA cases were seen before the introduction of PCR at SSHC, many subjects may have had their chlamydia infections missed. As there was a non-significant association between ReA and recent/current chlamydia (Table 2), a more sensitive test early in the study period may have altered the outcome of the analysis. The use of less sensitive tests may also partially explain the relatively small number of ReA patients reporting a past, recent or current infection with chlamydia. The introduction of PCR tests does not entirely explain the increase in chlamydia diagnosis: the change in test method in the mid-1990s resulted in a modest increase in diagnostic yield, 31 but this increase is ongoing. It is, however, important to note that this study did not assess trends in the enteric infections which are also known causative agents of ReA.
Conclusion
This study shows a decline in diagnoses of ReA over a 20-year period in a primary care setting despite increasing chlamydia diagnoses. This mirrors decreases in other chlamydia-related complications such as PID, epididymitis and ectopic pregnancy in both primary and hospital care over the same time frame. This suggests that the relationships between chlamydia and its sequelae are not well understood, and further research into chronic complications of genital chlamydia infections is warranted.
Footnotes
Acknowledgements
Thanks to Heng Lu for his technical assistance with the SSHC database.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.