
Abstract
This study investigated the epidemiological and clinical characteristics of hepatitis B virus (HBV) in HIV-infected adults at the time of antiretroviral therapy (ART) initiation in Guangdong province, China. A total of 2793 HIV-infected adults were enrolled between January 2004 and September 2011. Demographic data and laboratory parameters were collected, HBV-DNA levels were measured, and HBV genotypes were identified before ART initiation. The prevalence of hepatitis B surface antigen (HBsAg) in HIV-infected patients was 13.2%. A total of 266 HIV/HBV co-infected patients and 1469 HIV mono-infected patients were recruited. The median alanine aminotransferase and aspartate aminotransferase levels of HIV/HBV co-infected patients were higher than HIV mono-infected patients (32 U/L vs. 22 U/L, p < 0.001 and 35 U/L vs. 24 U/L, p < 0.001, respectively), whereas the median CD4 cell count of HIV/HBV co-infected patients was lower than HIV mono-infected patients (59 cells/mm3 vs. 141 cells/mm3, p < 0.001). The level of CD4 cell count was lower in hepatitis B e-antigen (HBeAg)-positive co-infected patients than HBeAg-negative patients (36 cells/mm3 vs. 69 cells/mm3, p = 0.014). A similar result was found in high level of HBV-DNA and low level of HBV-DNA groups (33 cells/mm3 vs. 89 cells/mm3, p < 0.001). HBV genotypes were classified as genotypes B and C. Patients infected with genotypes B and C differed significantly in terms of proportion of those who were HBeAg-positive (40.5% vs. 62.2%, p = 0.014). This study indicates a high prevalence of HBsAg in HIV-infected adults in Guangdong. The level of CD4 cell count in HIV/HBV co-infected patients was much lower than HIV mono-infected patients, especially in patients who were HBeAg-positive and had a high level of HBV-DNA. The predominant HBV genotype in HIV/HBV co-infected patients is genotype B.
Introduction
Co-infection with hepatitis B virus (HBV) and human immunodeficiency virus (HIV) is very common because they share similar transmission routes. 1 In HIV-positive patients, HBV infection is more likely to be chronic.2–4 Compared to patients infected with HBV alone, co-infected patients also have more episodes of HBV reactivation, higher HBV viral loads, lower rates of hepatitis B e-antigen (HBeAg) sero-conversion and faster progression to cirrhosis, hepatocellular carcinoma and end-stage liver disease.1–3,5–9 In addition, HIV/HBV co-infection is associated with significantly increased liver-related mortality, especially after the initiation of antiretroviral therapy (ART), which has led to a decline in death from acquired immunodeficiency syndrome (AIDS)-related diseases.3,10–14 Mortality and morbidity associated with liver disease are major concerns, 5 and screening for hepatitis co-infection in HIV patients is strongly recommended.13,15–19
The prevalence of HBV in people living with HIV varies among populations and especially among geographic regions. 2 In Africa and Asia, where HBV is endemic, the prevalence of co-infection is 20–30%. 20 In Western Europe and the USA, the rate of chronic HBV infection in HIV-positive persons is 6–14%. 21
China has a high prevalence of hepatitis B surface antigen (HBsAg). The prevalence of HBsAg in the general population aged 20–59 years is 8–12%. 22 HIV infection is increasing rapidly in China. There were 436,817 HIV/AIDS patients in China as of 31 December 2013. Some studies have shown that the prevalence of HBsAg in HIV-infected patients ranges from 4.2% to 19.4% in different areas.18,19,23–26 But there is a lack of information on this issue in Guangdong province. The aim of this retrospective study was to investigate the epidemiological and clinical characteristics of HBV in treatment-naive HIV-infected adults in Guangdong province of China.
Materials and methods
Study population and data collection
This retrospective study was conducted in Guangzhou No. 8 People’s Hospital from January 2004 to September 2011. Patients were included if they met the following criteria: (1) HIV-positive confirmed by Western blot; (2) 18 years or older; (3) antiretroviral-naive. Individuals who were less than 18-years-old were excluded from the study. Demographic data and laboratory values were collected from medical records before the initiation of ART. The upper limits of normal (ULN) of both alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels were 40 U/L.
Definition
Patients were classified as having HIV/HBV co-infection if they were HBsAg-positive. High level of HBV-DNA was defined as HBV-DNA is equal or higher than 5 log10 copies/mL. HBV-DNA lower than 5 log10 copies/mL was considered as low level of HBV-DNA.
HBV-DNA quantitation
Plasma HBV viral load was measured using a commercial real-time polymerase chain reaction (PCR) with a lower limit of detection of 500 copies/mL (DaAn Gene Diagnostic Company, Limited of SUN YAT-SEN University, Guangzhou, China), in accordance with the manufacturer’s instructions. Positive samples were subjected to further analysis.
HBV-DNA extraction and nested PCR
Viral DNA was extracted from 200-µL serum samples using a QIAamp DNA Blood Mini Kit (Qiagen, Hilden, Germany) as recommended by the manufacturer. The DNA was eluted in 200 µL of elution buffer and used immediately or stored at −20°C for later use.
A nested PCR was performed to amplify a segment of the HBV S genome with two sets of primers. The first-round primers were 5′-GCC TRT ATT TTC CTG CTG GTG GCT CCA G-3′ (forward) and 5′-TCC AGA CCK GCT GCG AGC AAA AC-3′ (reverse). The second-round primers were 5′-TAT TTT CCT GCT GGT GGC TCC AGT TC-3′ (forward) and 5′-GTT CCG CAG TAT GGA TCG GCA GAG G-3′ (reverse). The PCR conditions were as follows: initial denaturation at 94°C for 3 min, followed by 30 cycles each of denaturation at 94°C for 30 s, annealing at 55°C for 30 s and extension at 72°C for 70 s, with a final extension step at 72°C for 10 min. The PCR products of the second amplification were electrophoresed on 1% agarose gels and examined under UV light and compared to the standard DNA marker. The positive samples were sent for sequencing (Life Technology, Shanghai, China). Negative controls were used in the PCR and electrophoresis steps.
Genotype identification
Nucleotide sequences were compared to previously reported sequences of different HBV genotypes and subgenotypes (A-H) obtained from GenBank (National Center for Biotechnology Information). Phylogenetic evolutionary analyses were conducted using MEGA 4.0. The phylogenetic trees were constructed using the neighbour-joining method and the Kimura 2-parameter algorithm. Bootstrap re-sampling and reconstruction were performed with 1000 replicates to confirm the reliability of the phylogenic trees. HBV genotypes and subgenotypes were determined by phylogenetic analysis.
Statistical analysis
Analysis was performed using SPSS version 16.0. Qualitative data were expressed as numbers and percentages. Quantitative data were expressed as median values and interquartile ranges (IQRs). Categorical variables were compared using the Pearson Chi square test. Comparisons between groups were analysed using the Mann–Whitney U test for quantitative variables. Multivariate logistic regression was performed to analyse the risk factors associated with HBsAg-positive. Odd ratios (ORs) and 95% confidence interval (CI) were calculated. A p value of 0.05 or less was considered statistically significant.
Results
From January 2004 to September 2011, a total of 2793 HIV-infected adults were enrolled. Among these patients, 369 (13.2%) were HBsAg-positive; of these, 103 were also hepatitis C virus (HCV) antibody-positive. No patients were co-infected with hepatitis D virus (HDV) and hepatitis E virus (HEV). Study flow was shown in Figure 1.
Flow chart of study design.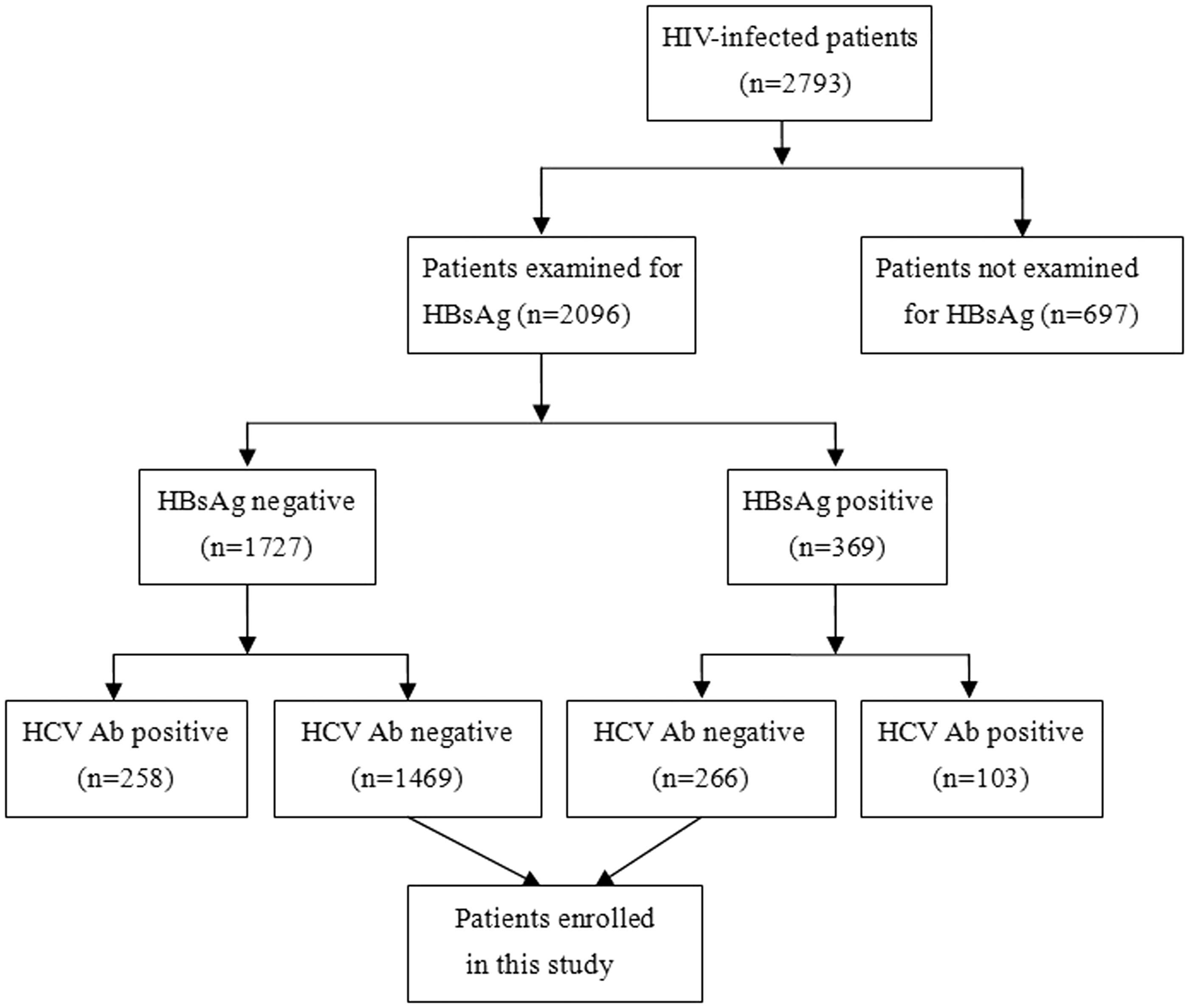
Epidemiological and clinical characteristics of the study patients: Comparison of HIV/HBV co-infected and HIV mono-infected patients
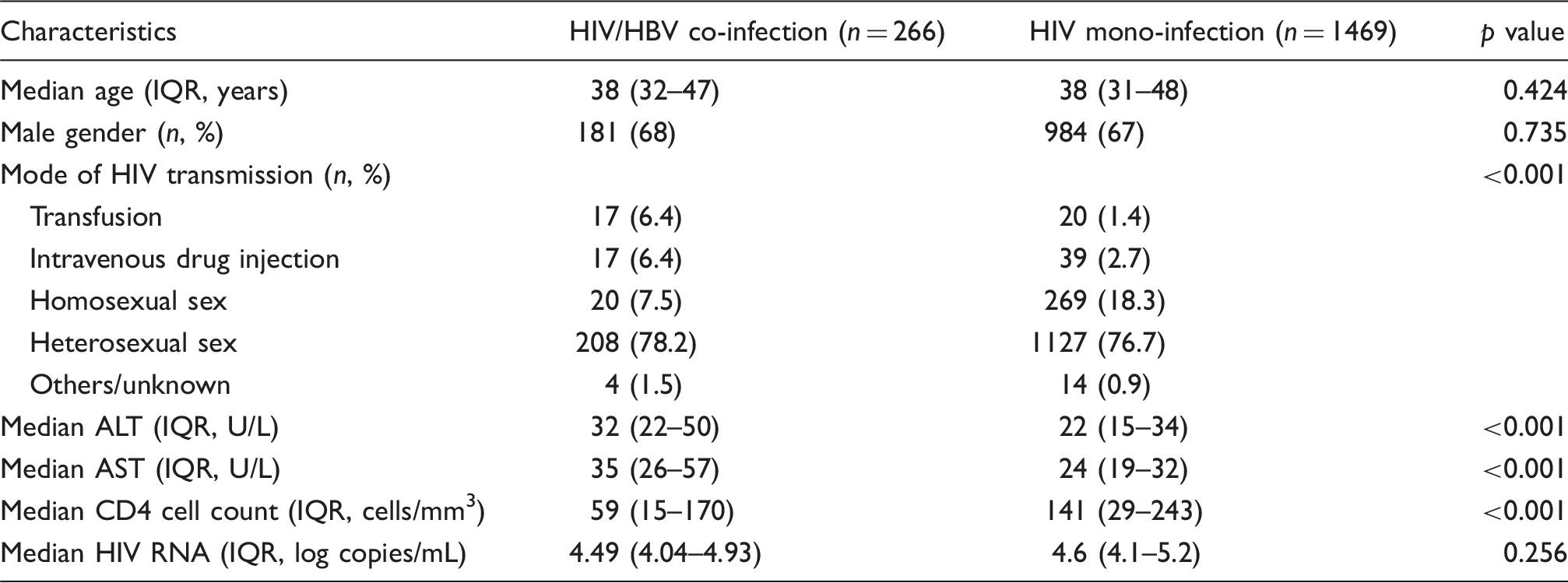
The differences were not statistically significant in terms of age and gender between HIV/HBV co-infected patients and HIV mono-infected patients (p = 0.424 and p = 0.735, respectively). The proportion of homosexual sex in HIV mono-infected patients was higher than in HIV/HBV co-infected patients. Difference was found in mode of HIV transmission in these two groups (p < 0.001).
ALT and AST values were both higher in HIV/HBV co-infected patients (median ALT 32 U/L, median AST 35 U/L) compared to HIV mono-infected patients (median ALT 22 U/L [p < 0.001], median AST 24 U/L [p < 0.001]).
Baseline characteristics of study patients.
Risk factors associated with HBsAg-positive
Multivariate logistic regression was performed in order to analyse the risk factors associated with being HBsAg-positive. Independent variables include age, gender, mode of HIV transmission, baseline CD4 cell count, baseline HIV RNA, baseline ALT and AST and WHO clinical stage. We did a univariate analysis first. The results indicated that risk factors, such as mode of HIV transmission, baseline CD4 cell count, baseline ALT and AST were significantly associated with being HBsAg-positive. Then, we performed multivariate logistic analyses to further clarify the risk factors. It revealed that mode of HIV transmission (OR = 1.220, 95% CI: 1.048–1.421, p = 0.004), baseline CD4 cell count (OR = 1.002, 95% CI: 1.001–1.004, p < 0.001) and baseline AST (OR = 0.987, 95% CI: 0984–0.991, p < 0.001) were the risk factors associated with HBsAg-positivity in HIV-infected patients.
Comparison of different HBV serostatus in co-infected patients at baseline
HBeAg and HBV-DNA status in HIV/HBV co-infected patients were associated with liver status and HIV parameters at initiation of HAART.
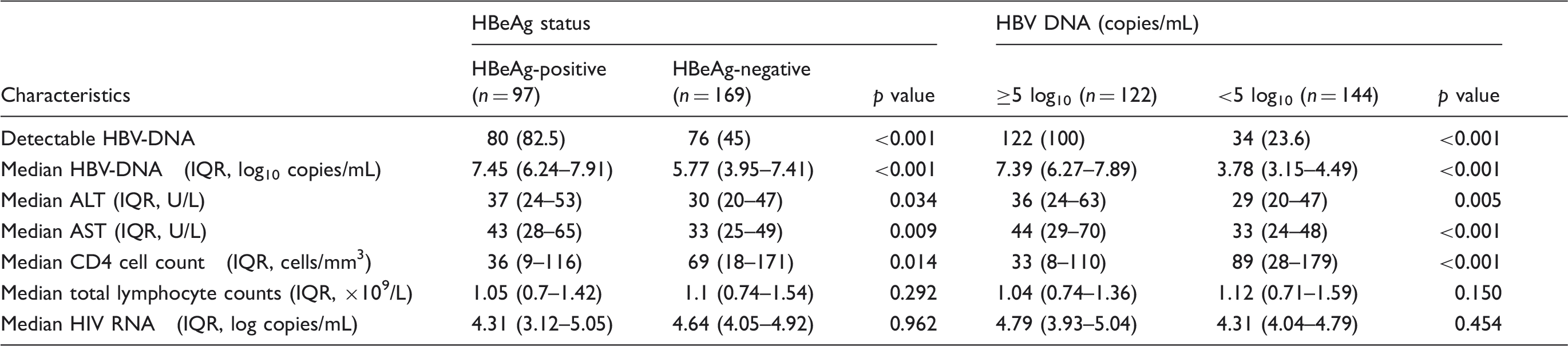
Being HBeAg-positive and having a high level of HBV-DNA were associated with a lower baseline CD4 cell count. HBeAg-positive patients had a baseline CD4 cell count of 36 cells/mm3 (IQR, 9–116 cells/mm3) compared to 69 cells/mm3 (IQR, 18–171 cells/mm3) in those with HBeAg-negative patients (p = 0.014). Those with high a level of HBV-DNA had a CD4 cell count of 33 cells/mm3 (IQR, 8–110 cells/mm3) – lower than those with a low level of HBV-DNA (median 89 cells/mm3 [IQR, 28–179 cells/mm3], p < 0.001), but no difference was found in the median total lymphocyte counts (p = 0.292 and p = 0.150, respectively) and HIV RNA (p = 0.962 and p = 0.454, respectively).
Comparison of genotypes B and C in co-infected patients
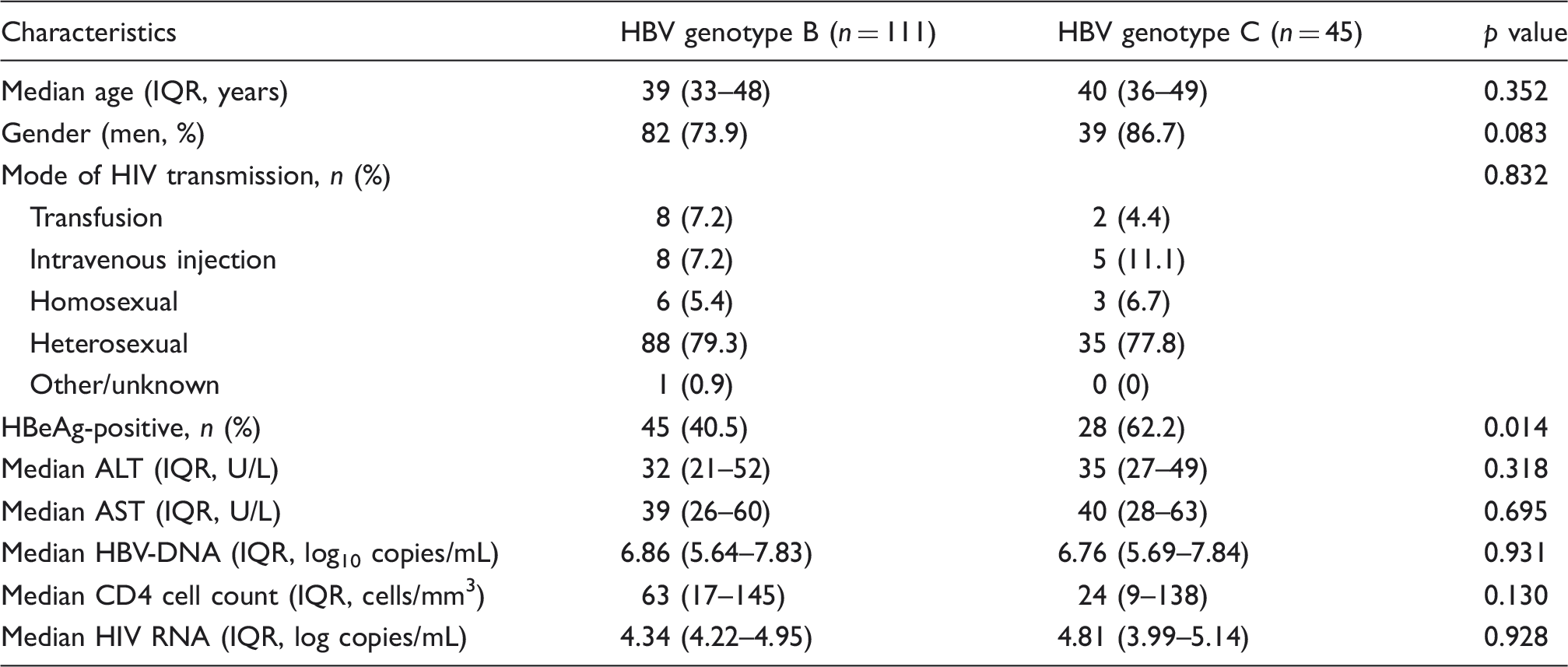
HBV genotypes were determined in 156 HBV-viraemic patients. According to the phylogenetic analysis, 111 and 45 cases were classified as genotypes B and C, respectively. The vast majority of patients were infected with genotype B2 (109, 69.9%), followed by C1 (36, 23.1%), C2 (9, 5.8%) and B1 (2, 1.2%).
Main characteristics of HIV/HBV co-infected patients stratified by HBV genotypes.
Discussion
This is the first time to analyse HIV/HBV co-infected patients characterising both HBV and HIV parameters before ART in Guangdong province. Notable results include the prevalence of HBsAg in HIV-infected adults, an association between HBV co-infection and lower CD4 cell count, especially those who are HBeAg-positive and with a high level of HBV-DNA and HBV genotypes distribution. Such notable findings contribute to our understanding of HIV/HBV co-infected patients in order to focus further therapy.
The prevalence of HBsAg among HIV-infected patients in this study was 13.2%, which is higher than the 10.2% to 12.6% reported by others.18,19,24 However, 13.2% is lower than the 14.6% and 19.4% reported by Wang et al. and Chen et al., respectively.25,26 These differences are mainly due to differences in the prevalence of HBsAg infection in different areas. In some provinces, the prevalence of HBsAg positivity in the general population is much higher; for example, in Fujian, a province in southern China, the prevalence of HBsAg is 23.46%, 27 while the seroprevalence of HBsAg in adults in northeast China is 4.38%. 28 Therefore, in a study population from high HBV-endemic areas, the prevalence of HIV/HBV co-infection will be higher than in a population in low-endemic areas. In our study, about 25% of the 2793 patients were not tested for HBsAg; therefore, we speculated that the prevalence of HBsAg in Guangdong province was higher than 13.2%.
Our study also found that the prevalence of HBsAg is higher in HIV-infected adults than in the general population. In China, the prevalence of HBsAg in the general population aged 1–59 years was 9.8% in 1992. 29 The prevalence of HBsAg decreased dramatically over a 15-year period due to the introduction of HBV-vaccination programs for all neonates in 1992. In 2006, the prevalence of HBsAg in the general population aged 1–59 years was 7.2%; however, in people aged 20–59 years, the prevalence was 8–12%. 22 High prevalence of HBsAg in HIV-infected patients may be associated with mode of HBV transmission. HBV can also be transmitted by parenteral and sexual contact, though not through mother-to-child transmission (MTCT).
In our study, we found that both a high level of HBV-DNA and HBeAg-positivity were associated with a lower baseline CD4 cell count. This result is consistent with previous reports, 30 but contradicts the study reported by Wang et al. 25 Wang et al. reported that HBeAg positivity was associated with low baseline CD4 cell count, but this association was not found in the high level of HBV-DNA group. 25 One possible explanation for the lower baseline CD4 cell counts in HBeAg-positive patients with a high level of HBV-DNA is that HBV replication can increase HIV replication, which decreases the CD4 cell count. Previous studies have demonstrated that HBV X protein can activate HIV RNA transcription.31,32 But HIV-RNA was not associated with a high level of HBV-DNA and HBeAg positivity in this study or in previous reports.25,30 These results indicated that HBV X protein was not the only reason why CD4 cell counts were low. Another reason is that HBV increases T-cell activation, which leads to increased apoptosis of CD4 cell.33,34 Finally, it may be associated with liver disease itself, but both liver biopsy and non-invasive assessment such as fibroscan were not done in this study.
In this study, we found that HBV genotype B was by far (71.2%) the most prevalent in HIV/HBV co-infected patients. Previous studies have shown that the distribution of HBV genotypes is related to geography and ethnicity. HBV genotypes are also associated with disease progression and response to antiviral drugs.35,36 In China, HBV genotypes B and C are predominant.37,38 In a previous study conducted by Zeng et al., the prevalence of genotype B in HBV mono-infected patients in Guangdong province was 53%, higher than that of genotype C (46%), 38 but Nie et al. found that genotype C was responsible for the majority (55.5%) of chronic HBV infection in South China, while the prevalence of genotype B was 21.8%. 39 This study also revealed that the HBeAg-positivity rate was lower in patients with genotype B than in those with genotype C, in agreement with the recent work reported by Zeng et al. 38 The study from Zeng includes 1096 chronic HBV carriers from nine provinces in China. They found that patients with genotype B had a lower prevalence of HBeAg than those with genotype C. 38 But a study in HIV/HBV co-infected patients showed that there was no significant difference between genotype B group and genotype C group in terms of HBeAg positivity. 40
This study had some limitations. First, we collected data from a single hospital in Guangzhou and this may not be representative of all patients in Guangdong province. Nonetheless Guangzhou is the economic and healthcare centre of Guangdong province, 41 and Guangzhou No. 8 People’s Hospital is a public infectious disease hospital and administers nationally-subsidised ART medications in Guangdong province. The hospital also provides treatment for HBV using standard interferon and oral nucleoside analogue drugs. Combined with our large sample size, we think it may still represent the prevalence of HBsAg in Guangdong province. Second, there were some missing data on HBsAg status due to the retrospective nature of the study. This may impact the estimates of prevalence of HBsAg in HIV-infected patients. Third, liver biopsies were not taken to assess the severity of liver fibrosis and inflammation. Therefore, we cannot analyse whether a lower CD4 cell count at baseline was associated with advanced liver disease. Finally the method for HBV genotyping was based on a partial sequence of the S gene; thus, no mixed genotypes could be identified.
In summary, our study indicates a high prevalence of HBsAg in HIV-infected adults in Guangdong province. ALT and AST levels in HIV/HBV co-infected patients were higher than HIV mono-infected patients, suggesting that drug-induced hepatotoxicity should be given greater attention during ART in co-infected patients. The level of CD4 cell count in HIV/HBV co-infected patients was much lower than HIV mono-infected patients, especially in patients who were HBeAg-positive and had a high level of HBV-DNA. The predominant HBV genotype in co-infected patients was genotype B.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: the Key Research Projects of the National 12th Five-Year Plan for the Prevention and Treatment of Major Infectious Diseases (No. 2012ZX10001-003) and Key Subject Programs of the Guangzhou Municipal Health Bureau (No. 2009Zdi-06).