
Abstract
Summary
This cross-sectional survey measured adult experience and perpetration of negative and potentially abusive behaviours with partners and its associations with mental and sexual health problems, drug and alcohol abuse in gay and bisexual men attending a UK sexual health service. Of 532 men, 33.9% (95% CI: 29.4-37.9) experienced and 16.3% (95% CI: 13.0-19.8) reported carrying out negative behaviour. Ever being frightened of a partner (aOR 2.5; 95% CI: 2.0–3.1) and having to ask a partner’s permission (aOR 2.7; 95% CI: 1.6–4.7) were associated with increased odds of being anxious. There were increased odds of cannabis use in the last 12 months amongst men who reported ever being physically hurt (aOR 2.4; 95% CI: 1.7–3.6). Being frightened (aOR 2.2; 95% CI: 1.5–3.2), being physically hurt (aOR 2.3; 95% CI: 1.4–3.8), being forced to have sex (aOR 2.5; 95% CI: 1.3–4.9) and experiencing negative behaviour in the last 12 months (aOR 1.7; 95% CI: 1.2–2.5) were associated with increased odds of using a Class A drugs in the last 12 months. Sexual health practitioners should be trained with regards to the risk indicators associated with domestic violence and abuse, how to ask about domestic violence and abuse and refer to support.
Introduction
The UK definition of domestic violence and abuse refers to ‘any incident or pattern of incidents of controlling, coercive or threatening behaviour, violence or abuse between those aged 16 or over who are or have been intimate partners or family members regardless of gender or sexuality’. 1 In this paper, we use the term domestic violence and abuse (DVA) to denote intimate partner violence or DVA. The terms men who have sex with men (MSM) and gay and bisexual men are reported as they are in other studies that are cited in this paper. According to the literature, MSM are more likely to be victims and/or perpetrators of DVA compared to men who do not have sex with men. 2 A systematic review of mainly US studies reported the lifetime prevalence of any type of DVA amongst MSM to be between 29.7 and 78.0%. 3 This abuse is associated with an increased risk of depressive symptoms, substance abuse, unprotected anal sex and HIV infection. 4
Health care settings are regarded as key entry points in which to address DVA with female patients and interventions implemented in sexual health and perinatal care demonstrate promising findings.5,6 The World Health Organisation 7 recommend that health care professionals should be trained to be aware of the mental and physical heath indicators of DVA, enquire sensitively about DVA and make appropriate referrals. However, little attention has been paid to the role of sexual health services in supporting gay, bisexual and other MSM affected by DVA. Recognising the risk factors associated with DVA in this group is an important first step towards raising awareness of the issue. In a separate publication from our study, we found that the majority of gay and bisexual men support enquiry for DVA by health professionals with two thirds favouring selective enquiry and one third enquiry of all patients. 8 Furthermore, men in the study regarded the sexual health clinic as an appropriate setting in which to develop interventions for men affected by DVA.
Although there is a growing body of evidence on DVA in gay, bisexual and other MSM, estimates of DVA prevalence should not be interpreted in isolation. Additional data are needed to measure the severity and health impact of abuse, as well as whether those involved perceive the behaviours as abusive. 9 Some negative behaviour between partners will fall outside of the definition of DVA, depending on perceptions of the behaviours. We report (1) the occurrence of negative behaviours consistent with DVA (experienced from a partner and carried out towards a partner) in a sexual health service population of gay and bisexual men; (2) the perceived impact of abuse; (3) the association between negative behaviour (experienced and carried out) with mental and sexual health problems and health risk behaviours (current anxiety and depression, sexually transmitted infections, alcohol and illicit drug use in the last 12 months) and (4) documentation of DVA in the medical records.
Methods
Study design
The study is a cross-sectional survey of male patients attending the sexual health clinics of a London teaching hospital. The study received ethics approval from South West Bristol Research Ethics Committee on 11 May 2010 (reference 10/H0106/22).
Participants
Between September 2010 and May 2011, a ‘Health and Relationships’ survey was administered in the waiting rooms of two general sexual health clinics and one specialist sexual health clinic for lesbian, gay, bisexual and transgender (LGBT) patients at a sexual health service in London. The clinics were randomly allocated across the 28-week data collection period. Male patients were invited by the researchers to participate if they were aged 18 or over, attending the clinic alone and could read and write English. Men were given a participant information sheet and consent form with the survey to read through. Men consented to either (i) completing the survey, but not giving permission for their medical records to be accessed or (ii) completing the survey and giving permission for their medical records to be accessed, which required them to provide their full name and date of birth on the consent form. Although private space in the clinic was not available for the participants, the survey was formatted as a small discrete booklet and was referred to as a health survey. Men returned the survey to the researchers who were based in the reception area to assist with completion and deal with any queries arising from participating in the study.
Survey variables
The Health and Relationships survey 10 elicited demographic information and sexual orientation as well as reported diagnoses of sexually transmitted infections (STIs) in the last 12 months. Current anxiety and depression were measured with HADS, the Hospital and Anxiety Scale, 11 using a cut-off score of 8 for the anxiety and depression sub-scales, which is indicative of the presence of a mild mood disorder. We conducted sensitivity analyses with 12+ thresholds for anxiety and depression as well as with the continuous measures of HADS. Alcohol use was measured with the AUDIT-C test 12 ; illicit drug use was assessed using single item yes/no questions on past year use of cannabis and class A drugs (Ecstasy, LSD, cocaine, crack, heroin and injected amphetamines). We computed the AUDIT-C score and classified men who scored more than four points on this scale as men affected by alcohol abuse or dependence. 13
The survey asked whether men had experienced, or carried out, one or more of four negative and potentially abusive behaviours as an adult. Negative behaviours experienced as an adult from a current or former intimate partner included: ever felt frightened of the behaviour of a partner; ever needed to ask a partner’s permission to work, go shopping, visit relatives or visit friends (beyond being considerate to and checking with a partner); ever been slapped, hit, kicked or otherwise physically hurt; and ever forced to have sex or made to engage in any sexual activity against one’s will. This was followed by questions on whether this had occurred in the last 12 months, relationship with the perpetrator, frequency and escalation of abuse, and perceived impact of the behaviours based on the COHSAR (Comparing Heterosexual and Same Sex Abuse in Relationships) survey by Hester et al. 9 Respondents were asked whether they had ever carried out the behaviours towards a current or former partner, whether this occurred in the last 12 months and whether they perceived a negative effect on their partner. Respondents were also asked whether they were in a domestically violent or abusive relationship currently and/or in the past. Whilst most studies tend to report the negative behaviours measured as DVA, the reality is complex. Individuals may report experiencing or carrying out behaviours, but not consider them harmful nor perceive them as abusive or only define particular behaviours as abuse.9,14 In order to differentiate between behaviours that our respondents said they had experienced and/or carried out, and self-perceived DVA, in the ‘Results’ section, we use the term ‘negative behaviour’ to denote the former and DVA for the latter. The survey contained a removable sheet with details of local support services and national help lines for survivors and perpetrators, and it encouraged respondents to talk to the researchers if they needed support. 15
Medical records
Although there was no clinical policy in the sexual health service for screening men for DVA, we wanted to explore the extent to which the issue was being detected by sexual health practitioners in this high risk population. Between December 2011 and July 2012, two clinic health advisors reviewed the sexual health medical records of patients who consented. In order for a patient to be coded as positive for DVA, there needed to be specific documentation that the patient was experiencing some form of emotional, physical or sexual violence or abuse from a current or former partner. The researcher (AMB) trained the health advisors in the different manifestations of DVA and was available to discuss any ambiguous documentation.
Data analysis
Analyses were conducted in Stata version 12.0. 16 For the main analysis, participants with missing data on abuse variables were excluded from estimations involving those variables. We performed separate logistic regressions for anxiety, depression, self-reported past year STI diagnosis, past year cannabis and Class A drug use, and alcohol-use variables on exposure to each negative behaviour experienced and carried out. The reference group for each negative behaviour experienced from a partner is not having experienced that particular behaviour from a partner. The reference group for each behaviour carried out towards a partner is not having carried out that particular behaviour towards a partner. We controlled for socio-demographic variables (age, income, maximum level of education, ethnicity) and sampling design (i.e. clinic attended). The models were based on previous evidence. 17
Men’s responses to whether they were currently or previously ‘in a relationship that could be described as domestically violent or abusive’ were compared with their responses to negative behaviours experienced and carried out.
Our main results are from a complete case analysis. We report how these results are compared to the analysis we conducted on 100 complete datasets generated with the missing data imputation by chained equation (mice) routine on the assumption that the data were missing at random. 18
Results
Socio-demographic characteristics
Clinic records show that 2657 men attended the two general sexual health clinics and the LGBT sexual health clinic on at least one occasion during the randomised weeks of the study period. Of these, 1132 (42.4%) men completed a survey, of whom five were excluded as their sexual orientation was not reported. This should not be treated as a response rate as it not known how many surveys were disseminated and returned. It was not possible to approach all potentially eligible men. Some were called in to their appointment straight away and the clinics were busy, making it difficult to keep accurate records on the number of men entering the clinic and the number of men who were approached and agreed or disagreed to participate. This was further complicated by the fact that some men accessed the clinics more than once during the randomised weeks of the study period, which could have resulted in the researchers double counting.
Of 1127 men who reported sexual orientation, 471 (41.8%; 95% CI: 38.1–46.4%) self-identified as gay, 61 (5.4%; 95% CI: 4.1–6.8%) as bisexual and 595 (52.8%; 95% CI: 48.6–56.3%) as heterosexual. Of the 532 gay or bisexual men, 154 (28.9%) were recruited from the LGBT sexual health clinic, and the remainder from two general sexual health walk-in clinics. Analyses relating to negative behaviours experienced are based on 519 gay or bisexual men who answered all four ‘experiencing’ behaviour questions. Analyses relating to negative behaviours carried out are based on 510 gay and bisexual men who answered all four questions on ‘carrying out’ behaviours. Men who reported negative behaviours experienced and those who reported negative behaviours carried out are not mutually exclusive groups, unless otherwise stated. The proportion of missing data ranged between 3 and 7% across negative behaviours and mental health variables.
Socio-demographic characteristics of gay and bisexual men.

Even with bootstrapping, confidence intervals were not obtainable for this column due to the small numbers and (in most cases) extreme proportions.
General Certificate of Secondary Education (GSCE) and Ordinary Level (O Level) are academic qualifications of UK examination boards conferred on students.
National Vocational Qualification (NVQ) is a work-based award in England, Wales and Northern Ireland achieved through assessment and training.
Advanced Level (General Certificate of Secondary Education A Level) is an academic qualification of UK examination boards conferred on students.
Reported negative behaviours in gay and bisexual men: as an adult and last 12 months.
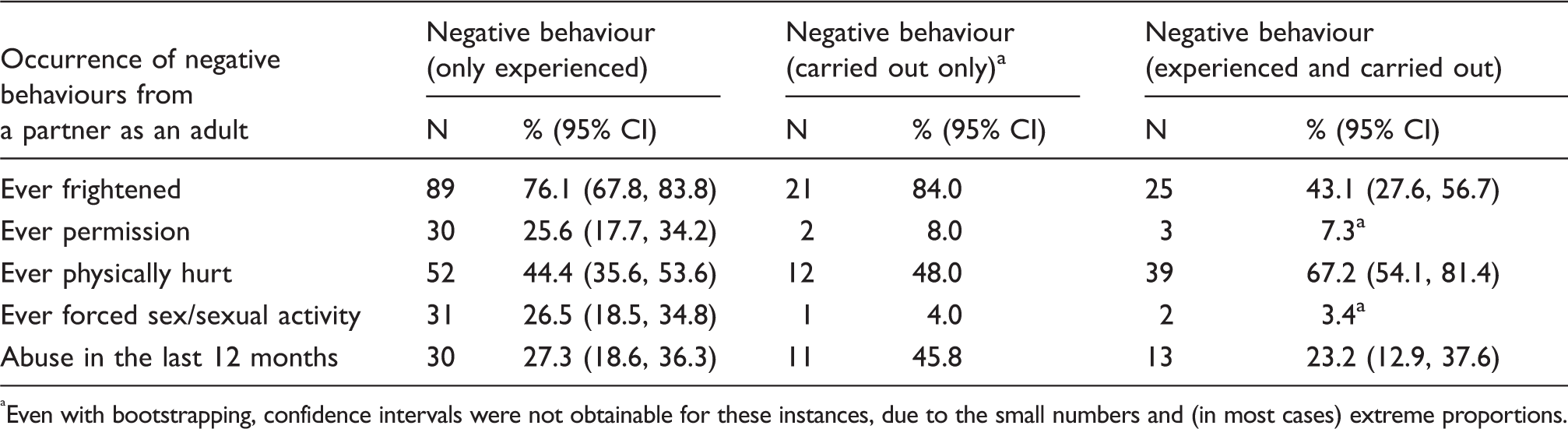
Even with bootstrapping, confidence intervals were not obtainable for these instances, due to the small numbers and (in most cases) extreme proportions.
Negative behaviour experienced and/or carried out
Prevalence and frequency of negative behaviours experienced from a partner
Frequency and escalation of negative behaviour experienced from a partner.

Prevalence of negative behaviours carried out towards a partner
Of 510 who answered, 83 reported carrying out a negative behaviour towards a partner (16.3%; 95% CI: 13.0–19.8%), with physical abuse (n = 54, 10.6%; 95% CI: 7.9–13.8%) and frightening behaviours (n = 55, 10.7%; 95% CI: 8.0–13.7%) most frequently cited.
Reported negative behaviours compared with perceptions of being in a DVA relationship
Of 168 men who reported at least one negative behaviour from a partner, 107 (63.7%; 95% CI: 56.0–70.9%) said that they had never been in a domestically violent or abusive (DVA) relationship. Similarly, 57 of 82 (69.5%; 95% CI: 58.8–79.7%) who reported carrying out at least one negative behaviour towards a partner stated that they had not been in a DVA relationship.
Perceived impact of negative behaviours experienced from a partner
Of 165 who responded, 16 (9.7%; 95% CI: 4.8–14.6%) reported sustaining injuries requiring medical treatment as a result of experiencing negative behaviour. In terms of perceived effects, of the 162 men who responded to all questions on effect, 106 reported some effect of any kind (65.4% 95% CI: 56.7–72.4%). Specifically, amongst the 106 men, 81 (76.4%; 95% CI: 67.1–84.1%) said that it made them feel anxious or depressed, 37 (34.9%; 95% CI: 26.0–45.1%) said that it affected their work or studies, 27 (25.5%; 95% CI: 17.0–34.2%) said that it made them drink more alcohol or take more drugs and 21/105 (20.0%; 95% CI: 12.6–29.1%) said that it damaged their physical health.
Perceived impact of negative behaviours carried out towards a partner
Out of 74 gay and bisexual men who reported carrying out at least one negative behaviour towards a partner, 37 (50.0%; 95% CI: 38.1–62.3%) felt that it had a negative effect on their partner.
Associations between negative behaviour experienced from a partner and health problems
Associations with health problems for gay and bisexual men experiencing negative behaviours from a partner.
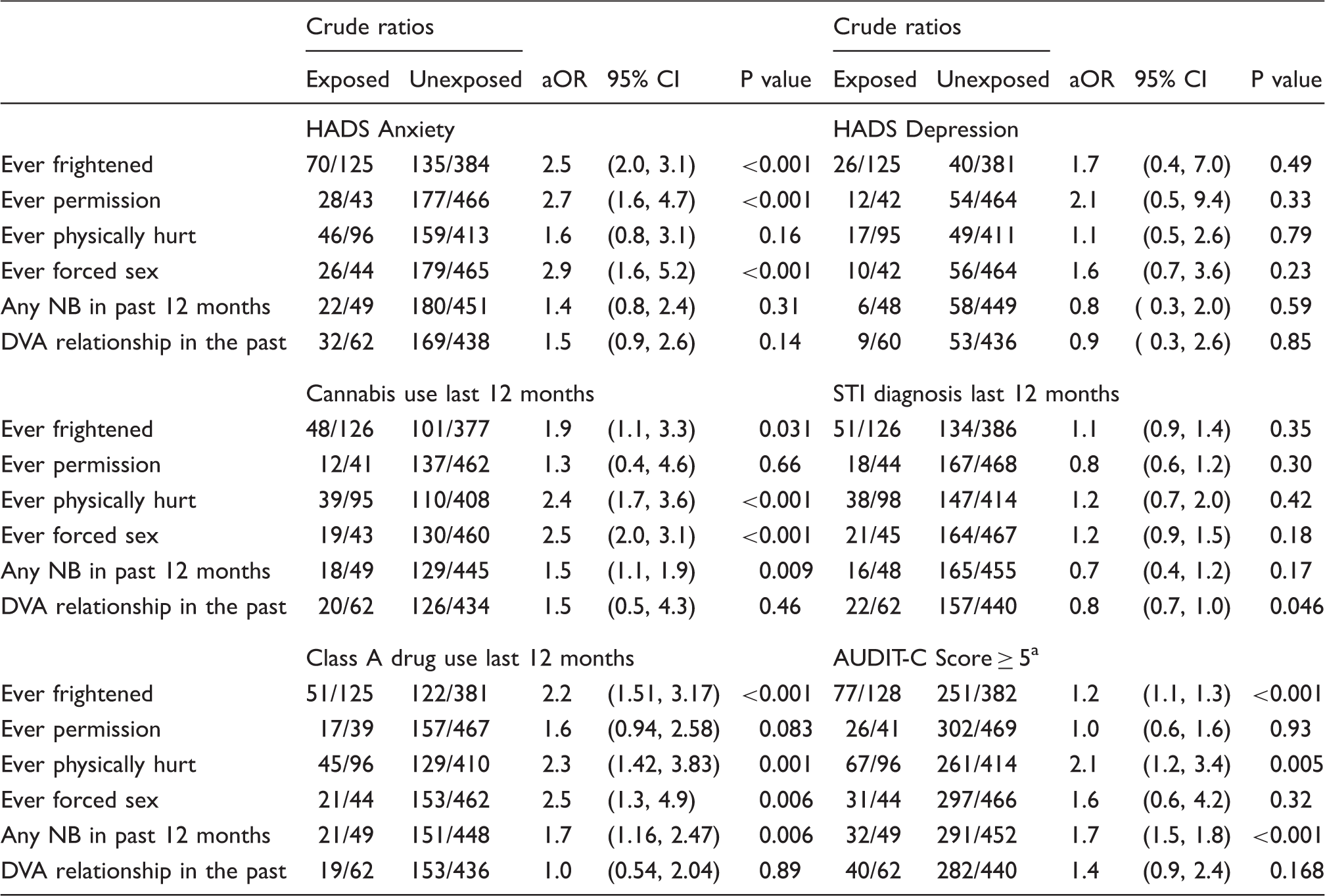
The reference group for each negative behaviour experienced, is not having experienced that particular negative behaviour.
We do not report on the association with currently in a domestically violent or abusive relationships because only six men reported being in one.
NB: negative behaviour; DVA: domestically violent or abusive.
A score of 5 or more on AUDIT-C is indicative of alcohol dependence or abuse.
Associations between negative behaviour towards a partner and health problems
Associations with health problems for gay and bisexual men who carried out a negative behaviour toward a partner.

The reference group for each negative behaviour carried out is not having carried out that particular negative behaviour.
We do not report on the association with currently in a domestically violent or abusive relationship because only six men reported being in one.
NB: negative behaviour; DVA: domestically violent or abusive.
A score of 5 or more on AUDIT-C is indicative of alcohol dependence or abuse.
Imputing missing data using the mice technique yielded estimates of associations that were on average 30% larger for men who experienced negative behaviour and 40% larger for men who carried out negative behaviour, compared with the complete case analysis. This suggests that biases resulting from non-completion of specific items in the questionnaire might have led to under-estimates of the associations reported in this paper.
Audit of medical records
Of the 532 gay and bisexual men, 238 (44.7%) consented to having their medical records reviewed, of which 211 (88.7%) were located. No evidence of DVA was found in any of the records.
Discussion
This is the first study to measure the occurrence and impact of DVA in gay and bisexual men attending a UK sexual health service. It elicits detailed information on frequency, severity, injuries, perceived health impacts and associations with objective measures of health, and health risk behaviours as well as respondents’ perceptions of being in an abusive relationship. Medical records from a sub-sample of men were reviewed for documentation of DVA by sexual health practitioners.
However, the study has a number of limitations. It is not possible to determine the temporal direction of the associations between health problems and negative behaviours due to the cross-sectional design. Less than half of the men who attended the sexual health service during the study period completed the survey, which may have created bias. Some were unable to finish the survey before being called for their visit. Similar challenges of implementing clinic-based surveys on DVA with men have been reported in general practice surgeries in the UK. 19 Issues such as the physical layout of the sexual health clinics and the researcher’s ability to see and approach all men entering the clinic was, at times, problematic. Some men were called in to see a practitioner before the researcher had an opportunity to approach them. If men needed to be seen by different practitioners in different areas of the clinic during their visit, it became difficult to keep track of where patients were located. Therefore, data are likely to be missing at random, supporting our choice of imputation process. The survey asked about sexual orientation, but not sexual behaviour and excludes men who engage in same-sex sexual activity, but do not identify as gay or bisexual. Welles et al. 2 found that men who experience conflict about having sex with men were less likely to identify themselves as gay or bisexual, but more likely to perpetrate DVA. Furthermore, the survey did not include a measure of internalised homophobia, which has been found to be associated with DVA perpetration among MSM. 20 The income categories were not exhaustive. However, it is reasonable to contend that this had no appreciable effect on the results since the current income brackets only exclude £1000 between each bracket and £5000 in total on the scale. It is therefore unlikely that the measure failed to capture a large number of respondents. Moreover, if respondents failed to respond because their income was not included, this event would be distributed across all brackets, and not affect one disproportionally.
The reported occurrence of negative and potentially abusive behaviours from a partner amongst gay and bisexual men (one in three) is consistent with other studies conducted in clinical and community settings.2,21,22 It is also higher than reported negative and potentially abusive behaviour found in heterosexual men attending general practice clinics in the UK, from another study within the PROVIDE programme, which used the same survey. 23 In our study, 11% of men reported both experiencing and carrying out negative behaviour. It is not known whether this was bidirectional abuse with the same partner, or if men had shifted from victimisation to perpetration in different relationships. 24 Questions to determine negative behaviour experienced and carried out within different relationships could have been included in the survey, but it was important to consider the respondent burden.
Our analysis found higher odds of poor mental health symptoms in men who experience or carry out abuse, although strong evidence for these effects is only apparent for a few behaviours. The imputed analysis suggests that the association between abuse and poor mental health may be an underestimate. Negative behaviours experienced and carried out were associated with illicit drug use and binge drinking, a finding which has been reported in a number of US studies of gay and bisexual men exposed to partner abuse.22,25,26 In terms of carrying out negative behaviour, only physically hurting a partner was associated with increased odds of using class A drugs.
The association between DVA and poor mental health and substance abuse in MSM populations has been highlighted in a systematic review by Buller et al. 4 Our measures of recent anxiety and depression (HADS) did not show an association across all negative behaviours experienced or carried out. However, HADS asks about symptoms in the past week and fails to capture past depression or anxiety. Attempting to measure whether depression or anxiety occurred concurrently with the abuse would have proved challenging due to recall bias. It is also possible that the abuse did not have a lasting effect.
Our study found lower odds of having a STI in the last 12 months amongst men who reported carrying out a negative behaviour in the last 12 months and those who reported being in an abusive relationship in the past. Whilst this finding is difficult to explain, our survey did not include a measure of sexual risk behaviour. Community surveys from North America demonstrate that gay and bisexual men affected by DVA are more likely to engage in sexual risk behaviours such as unprotected anal sex, which can result in STI transmission.22,27,28 Our survey was conducted in a sexual health service where men attend for prevention as well as treatment, and they may have had better sexual health compared to studies of MSM in the community. It is also possible that experiences of negative behaviour occurred in relationships that had ended, thereby reducing men’s risk of contracting an STI in the last 12 months.
Two-thirds of men who reported experiencing or carrying out at least one type of negative behaviour consistent with abuse did not consider themselves to have been in a DVA relationship. This confirms that broad generic questions on abuse result in under-reporting compared to questions about specific behaviours. Gay and bisexual men find it difficult to make sense of their abuse experiences because historically discourses on DVA have constructed the issue as being about men’s violence against women. 9 In a survey of same sex DVA by Hester et al., 9 respondents were most likely to define their experiences as DVA if they had experienced physical or sexual abuse or multiple forms of abuse, compared to those who experienced emotional abuse only. Therefore, interventions involving enquiry for DVA may be more likely to elicit disclosure when questions are asked about specific acts of abuse, frequency, severity, escalation and impact.
The audit of the medical records found no documentation of DVA. This is likely to reflect the absence of a policy of asking male patients about abuse at the time, a consequent low disclosure rate in the clinics, men’s lack of recognition of their experiences as abuse and possibly a failure to record disclosures that are made. However, without official documentation, men may be deprived of their right to protect themselves from the abuser if pursuing legal remedies or seeking accommodation. Furthermore, without a system for recording DVA, there is no method of communicating the information to other health professionals involved in the patient’s care.
The findings of this study are significant in the context of the Public Health England 29 action plan 2015–2016 where DVA is highlighted as a major social determinant of the health inequalities affecting gay, bisexual and other MSM. PHE plans to improve the evidence base regarding same sex partner violence and its impacts in order to inform clinical practice and service provision.
There have been no intervention studies within sexual health services for gay and bisexual men affected by DVA, yet studies of women show that they are opportune settings for interventions involving enquiry for DVA and referral to support services.5,30,31 The National Institute for Health and Care Excellence Domestic Violence Guidelines 32 cite sexual health services as a setting where clinicians should ask service users about DVA as part of routine good clinical practice ‘even where there are no indicators of such violence and abuse’. Further research is necessary as different intervention approaches may be needed for gay, bisexual and other men who have sex with men. Sexual health services can play an important role in supporting gay, bisexual and other MSM who experience or perpetrate DVA. Training and awareness-raising should include information on the prevalence of DVA, associated health problems, risk indicators, how to make sensitive enquiries about DVA and respond to disclosures of abuse. Health practitioners also need to be aware of the growing number of organisations that are dedicated to offering practical and emotional support to lesbian, gay, bisexual and transgender communities exposed to domestic violence.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper presents independent research commissioned and funded by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0108-10084). The views expressed in this publication are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.