
Abstract
Peripheral neuropathy is one of the most common neurological complications of HIV infection with a 30–60% lifetime prevalence. Newer HIV drugs cause less peripheral neuropathy, but patients are now living long enough to develop concomitant diabetes-related, vascular-related, and chemotherapy-related neuropathy so it continues as a major debilitating issue. Recent national CDC guidelines have stressed the importance of non-opioid therapies, especially in this population that may have had drug abuse problems. We treated a 52-year-old man who had severe disabling classic peripheral neuropathy since 1998 with Scrambler Therapy (Calmare), an FDA-cleared peripheral non-invasive neuromodulation device. His pain rapidly improved, as did his motor and sensory function, with just four 45-min treatments, and he was able to come off opioids for the first time in years. When his pain returned six months later, only two treatments were needed to resolve it. This represents the first published use of this novel, inexpensive, and non-invasive pain modality in HIV peripheral neuropathy, and should engender further trials.
Introduction
Peripheral neuropathy (PN) is one of the most common neurological complications of HIV infection with a 30–60% lifetime prevalence.1–4 Drug treatment helps only about one-third. 5 New CDC guidelines recommend against long-term opioid treatment for chronic pain and call for new, safe approaches to pain management. 6 Scrambler therapy is an FDA-cleared treatment for neuropathic pain supported by multiple trials. 7 Scrambler therapy reduced chemotherapy-induced neuropathic pain, numbness, and tingling by 50%8,9 and reduced opioid use. 10 We report here the treatment of an HIV-PN patient for the first time.
A 52-year-old man was diagnosed with HIV in 1998 when he developed bilateral paresthesias before starting ART. His neurologic symptoms and examination were stable from 2001 to 2015 with numbness and shooting pains on the soles and paresthesias to above the ankle. Exam showed absent ankle reflexes and vibratory sensibility at the toes and loss of pinprick and light touch to just above the ankles bilaterally. His HIV load had been undetectable for at least five years on elvitegravir–cobicistat–emtricitabine–tenofovir (Stribild®) 150–150–200–300 mg. Previous treatment trials of gabapentin up to 3200 mg a day, pregabalin, duloxetine, venlafaxine, capsaicin, and lidocaine patches were unsuccessful. Since 2012, he had been prescribed extended release morphine (Kadian®, Avinza®) 30 mg and oxycodone/acetaminophen (Percocet®) 10 mg/650 mg daily with some relief.
At the time of Scrambler therapy treatment, he rated his numbness and pain at 10/10 at its worst, 5/10 at its best, and 8/10 average. He was treated with pairs of electrodes from behind the malleoli to behind the contra-lateral fifth and first toes, as shown in Figure 1, daily for 45 min. His pain rating was reduced after four treatments to 1–2 on his right side and 4 on his left side. He was able to flex his toes and perform the yoga crane pose for the first time since 1998. He stopped his morphine and oxycodone after these treatments, and was able to walk for miles.
Placement of Scrambler Therapy electrodes to treat HIV–PN on the soles.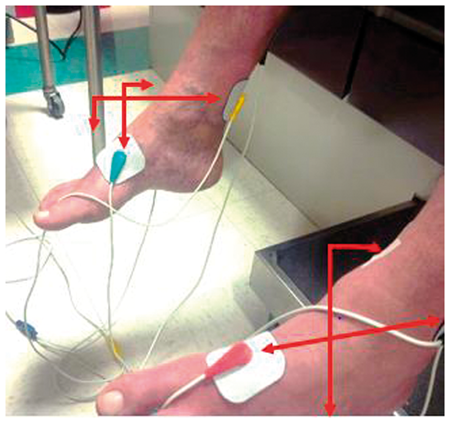
Six months later, his pain returned over several weeks limited to his toes (8/10 on the left; 6/10 on the right). After two treatments, his pain reduced to 1/10. Four months later, his pain again began to return and he again underwent successful treatment with just one session, in Figure 2.
Pain scores over time; treatments were given on days 1–4, 121–122, and 244.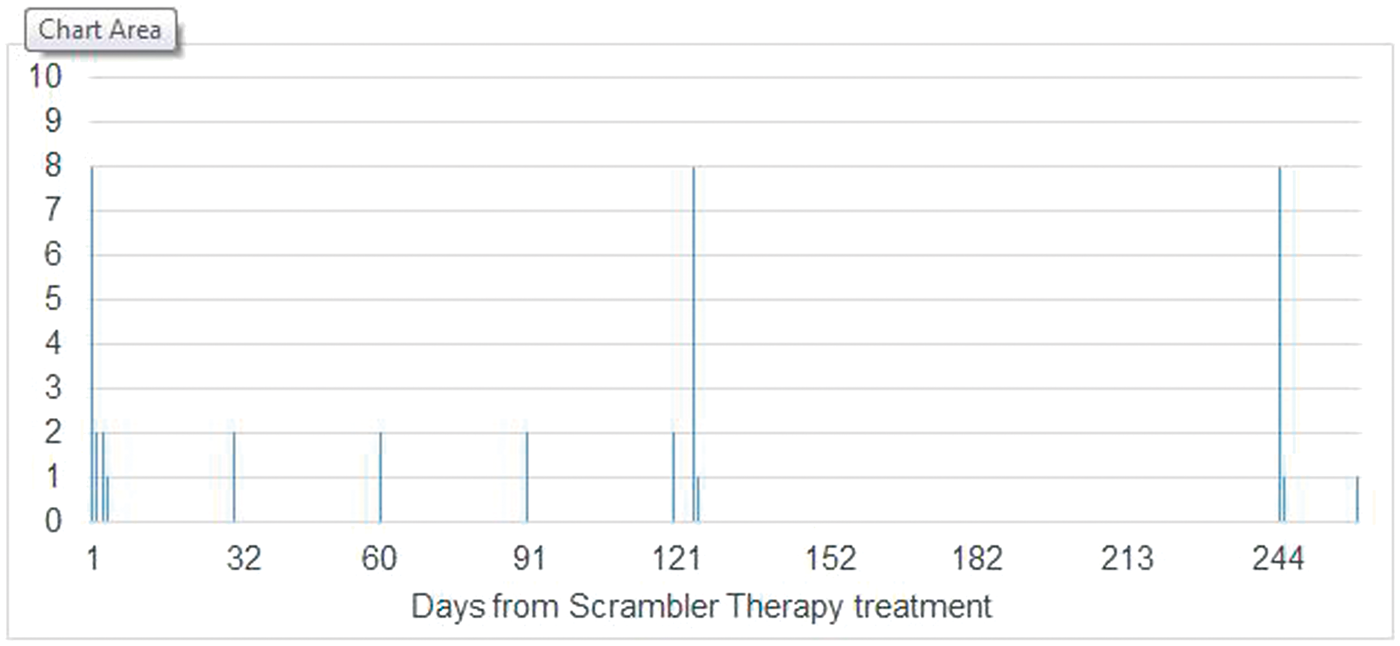
His response was dramatic, sustained, repeatable, and improved his function. This is the first reported use of this technology to treat HIV-related pain. It illustrates that HIV-PN may be amenable to electrostimulation, that treatments can be repeated, and that many patients will not need 10 full treatments; indeed, the manual says to treat only until the pain is gone and stop at that point. Importantly, in the context of new recommendations regarding long-term opioid treatment, he was able to completely discontinue morphine and oxycodone. While his response may be attributable to some other factor, the pain relief than enabled him to stop opioids demonstrates the need for rigorous trials of Scrambler Therapy for HIV-PN.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.