
Abstract
An inner Sydney sexual health service introduced the option to gay and bisexual men of receiving a negative HIV result by SMS to mobile phone one business day after venipuncture (rapid SMS). Men could also choose one of the other options: a point-of-care-test (POCT), by phone, or in-person (clinicians could also require in-person). We followed-up patients choosing the rapid SMS method to ascertain their satisfaction. During 12 months, 473 men had 591 HIV tests. Of these tests, 5.4% were POCTs, 9.1% were in-person, 24% were by phone, and 62% were rapid SMS. HIV POCTs declined from being 22% of result methods in the pre-study period to 5.4% during the rapid SMS intervention period (odds ratio 0.20, 95% CI 0.13–0.32, P < 0.0001). Phone/in-person results declined from 78% to 33% (odds ratio 0.14, 95% CI 0.10–0.20, P < 0.0001). SMS was sent by the next business day in 95% of cases; 96% of men were satisfied; and 95% would choose this method for their next test. Of 77 men who previously had an HIV POCT, 56 (73%) elected a rapid SMS result rather than having another POCT. The higher accuracy of conventional serology was commonly expressed as the reason for choosing rapid SMS for results.
Keywords
Introduction
In many countries, including Australia, there have been recent increases in HIV incidence, predominantly in gay, bisexual and other men who have sex with men (GBM). 1 More frequent testing of GBM, and reaching those who have been reluctant to test, are proposed in order to detect infections at an earlier stage, 2 because earlier treatment benefits the individual and reduces ongoing transmission.3,4 Surveys show that GBM want the testing process to be more convenient, and deliver the result more quickly.5,6 Less than a decade ago, it was common policy for patients to return in-person to receive HIV test results. 7 Provision of negative HIV test results by telephone is now commonplace. 8 While this is more convenient, and has led to increased testing and more patients actually getting their results, 9 the time between test and result is still typically five to seven days. 10
HIV testing by point-of-care test (hereafter called ‘HIV POCT’) provides a result at the clinic visit and may encourage more testing of those at higher risk. A large multi-centre study in Sydney has shown HIV POCT to be popular among GBM,10,11 with an increase in testing frequency; 12 however, a randomised controlled trial in Melbourne did not show sustained increase in testing. 6 Also, HIV POCTs when used as standalone screening tests, have lower sensitivity in detecting recently acquired infection, compared with gold-standard fourth-generation enzyme-linked immunosorbent assays (ELISAs) performed on serum.11,13
The popularity of text messaging (short message service [SMS]) has been seen as it is used by the health sector to convey short communication to patients, especially reminders for appointments. In Sydney, a survey at a large sexual health service indicated that delivery of test results by SMS would be as acceptable as receiving results by telephone or in-person. 14
The immunopathology laboratory for our clinical service routinely conducts conventional fourth-generation HIV serology testing twice daily (Monday–Friday) and can deliver negative results by the following day. In this study, we aimed to (i) deliver conventional HIV serology negative test results by SMS to GBM by one business day after venipuncture (hereafter called ‘rapid SMS’ HIV results), (ii) determine the uptake and acceptability among GBM of receiving results by this method, and (iii) explore reasons for the choice of this test result method.
Methods
From October 2011, Northern Sydney Sexual Health Service began performing HIV POCTs for GBM as part of a multi-centre study in Sydney. 11 From December 2012, we also offered the option of receiving HIV results (if negative) by rapid SMS to the patient’s mobile phone one business day after venipuncture. We conducted this study of delivering HIV results by rapid SMS during the 12-month period of December 2012 to November 2013. Clinicians determined if GBM needed to return in-person for a result, according to a previously published guide. 15 Otherwise, after discussing the options with their clinician, GBM were able to choose between having an HIV POCT, receiving HIV results (if negative) by rapid SMS, or receiving their HIV result by phone five to seven days after venipuncture, or returning in-person. Importantly, all the HIV POCTs conducted at our service (and elsewhere in Sydney) were part of a formal study whereby they were evaluated and confirmed by conventional fourth-generation serology. 11 Those having an HIV POCT were not eligible to receive their serology result by rapid SMS. They were able to receive this result by phone five to seven days after their clinic visit. We designed a script sheet for clinicians to facilitate and standardise explanation of these options with patients. Information given to patients about accuracy of HIV POCTs was similar to previously reported. 10 Briefly, we explained that an HIV POCT may miss HIV infection that was recently acquired and also could have a false-positive reaction. For any patient whose HIV serology result was reactive, the result was not sent by SMS but was managed according to the clinic’s usual policy. Briefly, this is to expedite a Western Blot test, and to contact the patient by telephone to inform and counsel them of an initially reactive sample that needs further testing.
The HIV POCT used during December 2012 to July 2013 was the Determine HIV Combo (Alere, Chiba, Japan) fingerprick rapid test, then beginning August 2013, the Trinity Biotech Uni-Gold HIV test (Trinity Biotech Plc, Bray, Co., Wicklow, Ireland). The conventional screening HIV test performed in the laboratory was the fourth-generation HIV screening immunoassay (Architect HIV Ag/Ab Combo, Abbott Diagnostics, Wiesbaden, Germany).
The files of patients electing to receive an HIV result by rapid SMS were assigned to the triage/results nurse, who would obtain the results from the pathology intranet service the following business day. The nurse would then send an SMS via the clinic’s database software to the patient. For privacy reasons, the text in the SMS was ‘Hi. Your blood test result is negative’.
We conducted a brief semi-structured telephone evaluation of patients who received an HIV result by rapid SMS. We asked specific questions about (i) satisfaction with the delivery of their HIV test result by rapid SMS, (ii) preferred method of delivery for future HIV results, and (iii) if there were concerns about the privacy of the SMS method. Opinions were also sought about the result delivery method, including comparisons with other methods and reasons for their choice. Some patients had more than one HIV test during the 12-month period. They were surveyed only once, which could have occurred after more than one experience of receiving their test result by SMS. We also surveyed clinical staff to ascertain which of the HIV test result methods they prefer to use in the clinic.
Data were entered into Microsoft Excel. We analysed data in SAS statistical software package, version 9.3 (SAS Institute Inc., Cary, NC, USA) and in Epi Info 7.1.5.2 (Centers for Disease Control and Prevention, Atlanta, USA). Proportions were calculated with exact binomial 95% confidence intervals (CI). The dependent variables (result methods) were investigated for significant changes after the intervention of providing results by rapid SMS, using the Chi square test and logistic regression. The Human Research Ethics Committee of Northern Sydney Local Health District approved this project for research.
Results
From December 2012 to November 2013, 591 HIV tests were performed in 473 GBM. Of these tests, 32 (5.4%) were POCTs, 54 (9.1%) were received in-person, 139 (23.5%) were received by phone, and for 366 (61.9 %) tests, 261 GBM elected to have the result sent by rapid SMS. Of these rapid SMS results, one test was indeterminate (this patient was phoned by clinical staff). Two anxious patients phoned the day after venipuncture before their SMS could be sent. Of the remaining 363, one specimen was incorrectly labelled, seven patient files were temporarily misplaced, and these patients phoned for their result. In 10 cases, the SMS was sent one day late, and in two cases, it was sent two days late. Thus, for 343 of 363 cases (94.5%, 95% CI 92.1–96.8), the results were successfully sent via SMS by the next business day. Results were delivered electronically to the clinic by the immunopathology service by the next business day for all cases.
Only one new HIV infection was diagnosed during the study period; his clinician determined his high risk and therefore recommended that he needed to return in-person for his result, according to our guideline. 15
Figure 1 illustrates the uptake of the rapid SMS method over time compared with the other methods of receiving HIV test results. Results by rapid SMS quickly became the preferred delivery method, and averaged 62% of all results during the study period. HIV POCTs declined from being 22.4% of result methods in the pre-study period to 5.4% during the rapid SMS intervention period (odds ratio 0.20, 95% CI 0.13–0.32, P < 0.0001). Similarly, phone/in-person results declined from 77.6% to 32.7% (odds ratio 0.14, 95% CI 0.10–0.20, P < 0.0001).
Uptake of receiving HIV results by rapid SMS.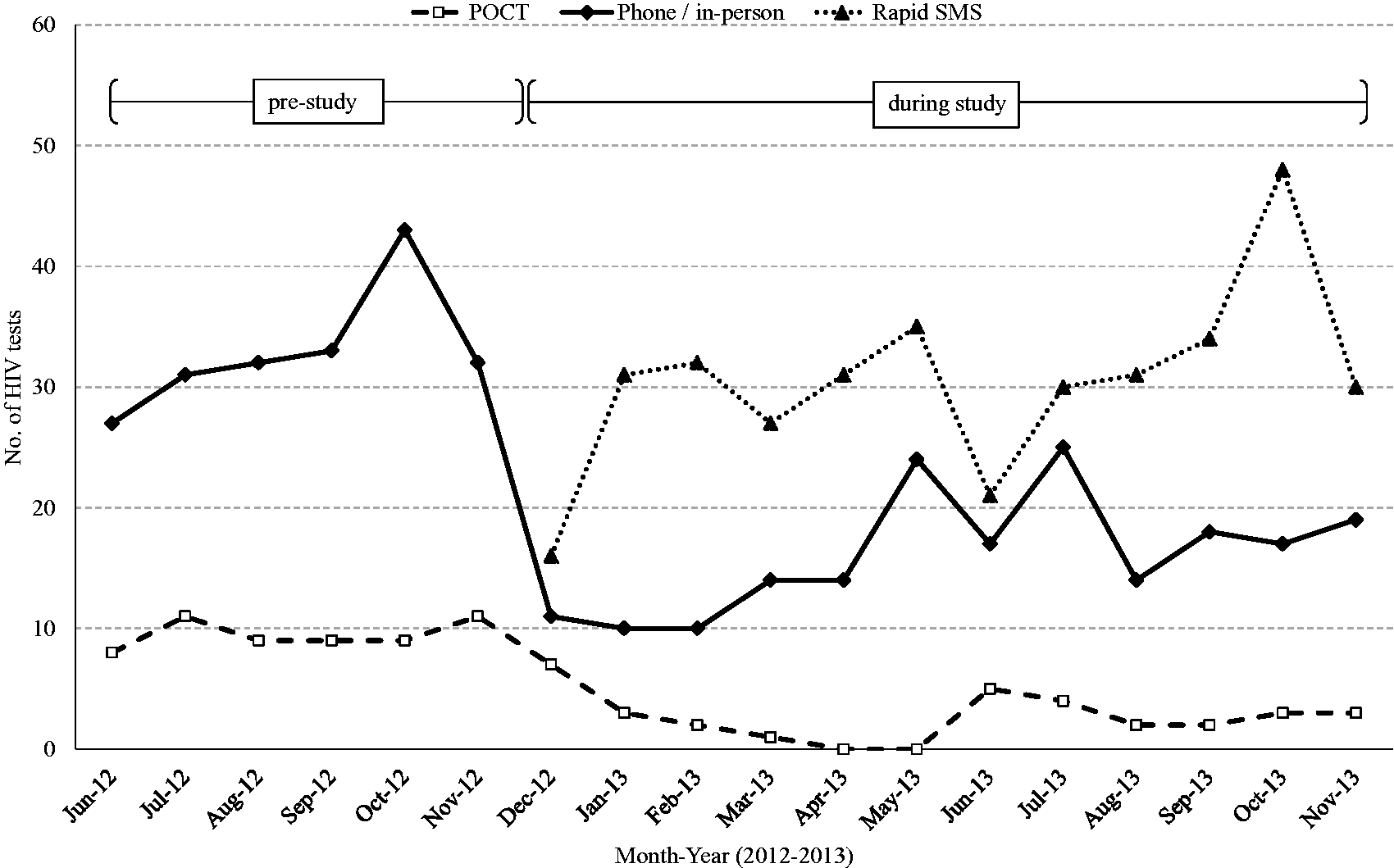
We were unable to contact 43 patients for their opinions of receiving HIV results by rapid SMS. We excluded the two patients who phoned the day after testing and the patient with an indeterminate result whom we phoned. This left 215 patients for evaluation. Of these, 207 (96.3%, 95% CI 93.7–98.8) were satisfied with the rapid SMS delivery; 205 (95.3%, 95% CI 92.5–98.2) would choose this method for the next test, and seven (3.3%, 95% CI 0.9–5.6) were concerned about SMS privacy (yet all seven were satisfied and elected the rapid SMS method for their next test). Many patients provided reasons for their choice. For 92 (42.8%) patients, the accuracy of the test was the most important factor in their choice of future test; they used phrases such as ‘most accurate test’, ‘wanted the most accurate test available’, and ‘the greater accuracy of serology’. After discussing the current policy of only using POCTs with back-up serology, the importance of accuracy as a factor in choice of future test was relevant for 79/215 (36.7%).
Of the 261 patients in the study, there were 77 who had previously had an HIV POCT. Of these, 56 (72.7%, 95% CI 62.8–82.7) elected a result by rapid SMS rather than a repeat HIV POCT (Figure 2). Of those contactable, 25 of 49 (51%) mentioned the greater accuracy of the conventional serology test as influential in the preference for HIV results by rapid SMS. Again, after discussing the current policy of only using POCTs with back-up serology, the importance of accuracy as a factor in choice of future test was relevant for 18/49 (36.7%).
Preferences of 77 GBM who previously had an HIV POCT at clinic.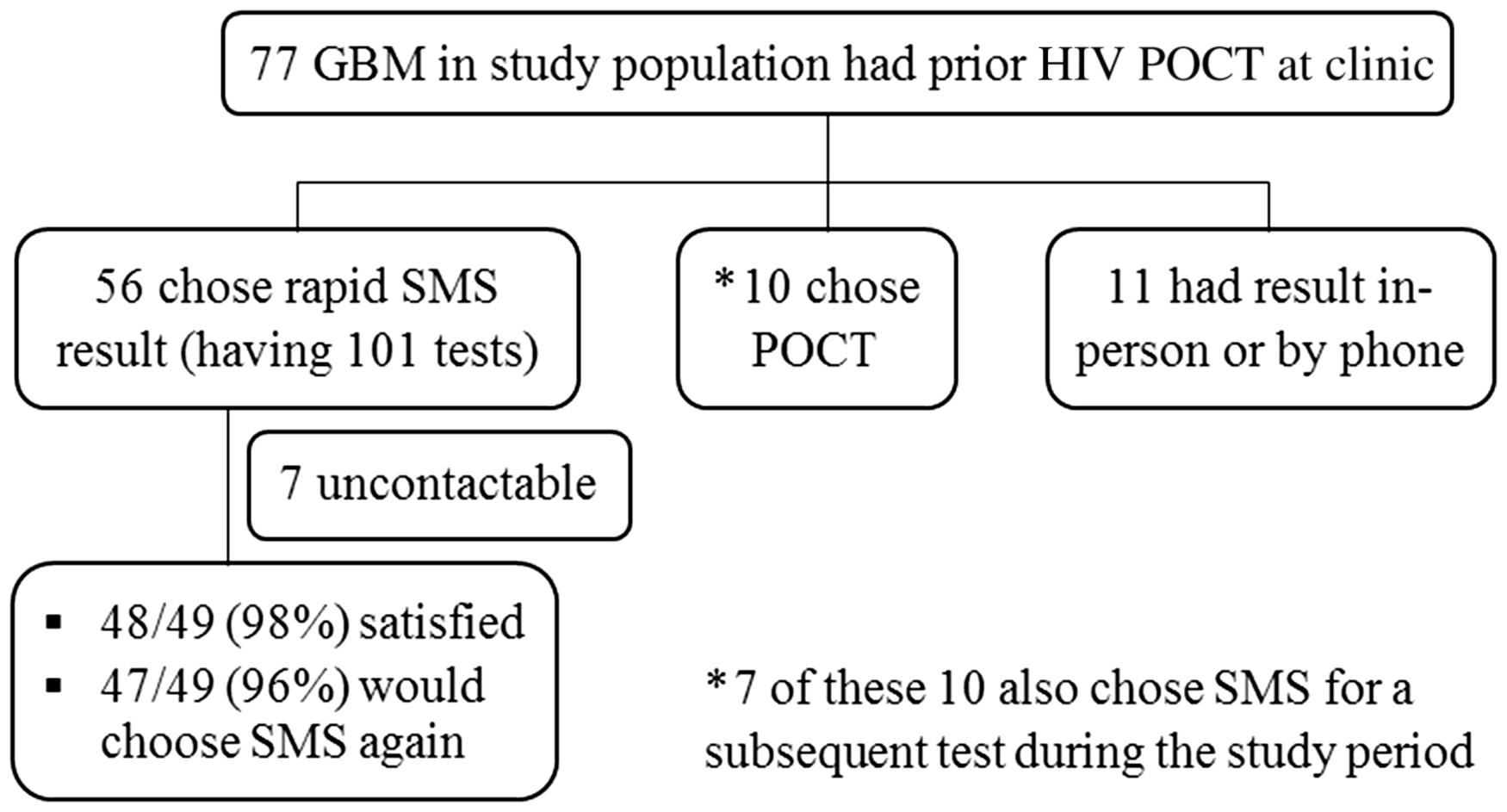
All clinical staff completed a survey to ascertain their preference of test result method to use in the clinic, and 16/18 (89%) preferred to use the rapid SMS method. The most common reasons provided for this choice were the greater accuracy, simplicity, patient preference, and least clinical time expended on managing results.
Discussion
In our clinic, we introduced the new procedure of sending HIV results by SMS to GBM patients on the next business day after venipuncture. This quickly became the preferred method of receiving HIV test results, with the great majority of men satisfied with this method, and reporting that this would be their preferred method for future testing. There was a corresponding reduction in the numbers of men receiving results by phone/in-person, or electing to have a POCT fingerprick test for HIV.
In previous studies, GBM have not had a choice between two methods of HIV test result delivered rapidly: typically HIV POCTs have been compared with serology results delivered one week after venipuncture, either by returning for results 6 or phoning for results, 10 and many men report that it is the long wait that causes them anxiety.6,10 We were able to reduce this wait to one day, with the process absorbed into the tasks performed by a triage/results nurse.
Together with the greater accuracy of HIV serology and (although not formally measured) an almost certainly shorter clinical visit compared with performing HIV POCTs, we postulate that this is the major reason for the preferences expressed by the men in our study. When we asked patients to provide reasons for choosing the rapid SMS method, and their preference for a future test, the lower accuracy (especially lower sensitivity) for HIV POCTs was commonly reported. This concern is well known.16,17 Many patients displayed astute discrimination in their survey feedback. The lower accuracy of HIV POCTs was of less importance when the patient knew there was back-up serology. It is therefore even more interesting that the majority of men still chose the rapid SMS result method. This preference persisted for those men who had direct previous experience of HIV POCTs. The rapid SMS result process did not involve the need to read study information or provide written informed consent (as was the case for HIV POCTs). Patients having an HIV POCT may react negatively to a longer clinic visit and documentation. 10 Also, we surmise that some patients may have experimented with their choices of receiving their HIV results. For example, while ten patients elected to have a POCT, seven of these subsequently chose a rapid SMS result.
Our study did not survey patients selecting the option of phoning the clinic for their HIV results, and this is a limitation. Anecdotal feedback from staff suggests that many patients want to receive all their sexually transmitted infection test results at the one time, want to speak to a clinician, or are concerned about privacy. Other patients during our study returned in-person to obtain their HIV test results. This was almost always due to clinical reasons; many patients required prompt follow-up of a clinical condition, or were quite anxious, required a language interpreter, or were at high risk of HIV infection (with an HIV-infected sexual partner).
The uptake and preference for obtaining results by the new method was immediate. This could be caused by bias among clinicians in how they explained the choices of receiving test results. Our clinical staff may have influenced the choice by patients, as the survey of staff revealed an overwhelming preference for the rapid SMS method due to its greater accuracy, simpler process and belief that it takes up less clinical consultation time. However, the effect seen was so immediate that it is unlikely even staff could have experienced the differences so quickly to have influenced patients. More importantly, it was the chosen method in the study period by most of those who had previous experience of an HIV POCT (56/77, 72.7%).
Our clinic has continued to provide HIV results to GBM by the rapid SMS method, which is now embedded into our clinical practice, and continues to be the most preferred method of receiving HIV test results. We continue to ask those at very high risk of testing positive, or who have psychological risks for poor adjustment to a positive result, to return in-person for results. 15 In the immediate 12 months after the study period (December 2013 to November 2014), HIV POCTs were 4.2%, phone/in-person were 32%, and rapid SMS were 64% of all HIV results in GBM. Our clinic ceased performing HIV POCTs in November 2014 as the persistently low number of tests being conducted did not meet operational standards. 18 For the next ten months for which data are available (December 2014–September 2015), phone/in-person were 30%, and rapid SMS were 70%, of all HIV results in GBM.
We should have done better in avoiding some errors. There were some cases where we failed to deliver the SMS result by the next business day. If promising to deliver a result to a patient within a specified time, a clinic needs attention to detail to avoid misplaced files, and regularly updating patients’ mobile phone numbers (plus a process to avoid transcription errors). Ability to deliver SMS should be integrated into the electronic medical record software. We experienced some initial problems in all these areas, which we suspect affected the confidence of some staff in the rapid SMS method, and could have resulted in more results by phone than otherwise might have occurred. Finally, the support of a laboratory that does frequent HIV testing and can reliably deliver results within the specified time is an important requirement.
HIV POCTs have good accuracy in detecting chronic HIV infection, but their sensitivity can be as low as 57% in detection of acute HIV infection compared with fourth-generation immunoassay.11,13 This becomes important for clinical services such as sexual health clinics, which are targeting and prioritising GBM with high-risk behaviour for frequent HIV testing, with the aim of diagnosing HIV as early as possible.19,20 In a recent study of HIV POCTs among sexual health services in NSW, 39% of all newly detected infections were classified as acute. 13 We agree that HIV POCTs should not be used as standalone screening tests when patients might have acute or recent HIV infection.11,13,21 Also, such high-risk men require frequent testing for syphilis, 22 best performed on serum.
We believe that inevitable improvements in technology will enable gold-standard tests to be performed more rapidly in the laboratory, even in the clinic or more remote locations, and delivered rapidly to clinical services, such that results will be available on the same day as testing. Examples of this have already occurred.23,24 In the meantime, we have shown that HIV tests, using the best available fourth-generation ELISAs, can be performed by a large laboratory, delivered to the clinic and then by text message to mobile phone by the next business day. Such a mechanism is popular with patients. For clinics serviced by laboratories with capacity to provide results within 24 h, this procedure may appeal as an alternative to performing HIV POCTs.
Footnotes
Acknowledgements
The authors thank the following: Bridget Dickson, Caradata for help with extraction of data from the electronic medical record Specialised Health Information Program (SHIP); Dr Rachel O’Connell, NHMRC Clinical Trials Centre, University of Sydney for assistance in statistical analyses; Catherine Needham for help in maintaining an Excel database; clinical staff at Northern Sydney Sexual Health Service and laboratory staff at ImmunoRheumatology Laboratory, Pathology North Sydney.
Contributors
SCD conceived and designed the study, was PI, educated staff, conducted telephone surveys, analysed the results, and wrote the paper; AK was study investigator, helped with study design and education of staff, and contributed to the paper; HEL was study investigator, conducted telephone surveys, and contributed to the paper; RBF was study investigator, managed laboratory testing and processing, and contributed to the paper; SLF was study investigator, supervised and managed laboratory testing and processing, and contributed to the paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.