
Abstract
Leukemia cutis is seen in around 20% of acute monocytic leukemia. They usually present as papules or nodules or infiltrated plaques but ulceration is uncommon. A 28-year-old female presented with multiple painless indurated genital ulcers of three weeks’ duration with low-grade fever, gum hyperplasia, and generalized lymphadenopathy. Tissue smear from the edge of the ulcer showed atypical monocytes suggestive of leukemic infiltrate which was further confirmed by peripheral smear and bone marrow aspirate. Herein, we report a case of acute monocytic leukemia (AML) with leukemia cutis presenting initially with genital ulcers simulating chancre.
Case report
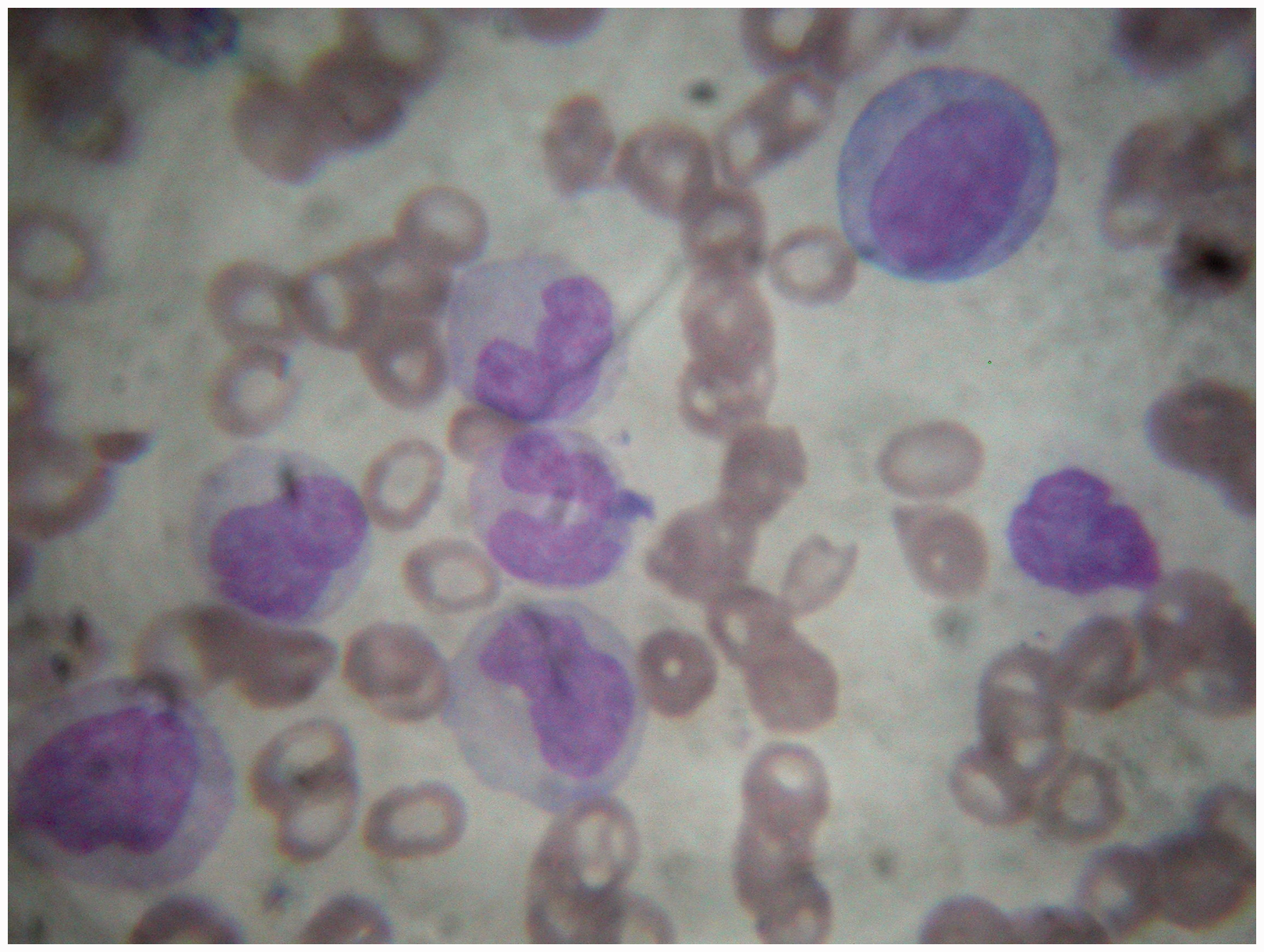
A 28-year-old married female presented to our STI clinic with two painless genital ulcers of three weeks’ duration. She also had occasional low-grade fever for one month. There was no history of oral ulcers, skin rash, joint pains, cough, or weight loss. She was not on any medications. Both she and her husband denied of any extramarital sexual contact. On general examination, there was pallor and generalized lymphadenopathy involving the cervical, epitrochlear, axillary, and inguinal nodes. Lymph nodes size varied from 0.5 cm to 2 cm and were discrete, firm, mobile, and nontender in nature. Examination of oral mucosa showed marked gingival hypertrophy (Figure 1). Examination of the genitalia revealed two ulcers, one on the right labia minora and another on the posterior fourchette. Both ulcers were of approximate size 2 × 1.5 cm oval in shape with clean floor, indurated base, nontender, and not fixed to underlying structures. Whitish mucoid vaginal discharge was present (Figure 2). Per vaginal and per rectal examination was within normal limits. Systemic examination was unremarkable. Dark ground microscopy for treponemes, Gram staining, and Tzanck smear from the genital ulcers were tested negative. Gram stain, KOH mount, and normal saline mount of vaginal discharge were also tested negative. A differential diagnosis of syphilitic chancre and leukemia cutis was made. Tissue smear from the edge of the ulcer showed atypical mononuclear cells (Figure 3). A complete blood count revealed anemia (Hb – 9.3 g%), leukocytosis (TLC – 56 × 109/L) with a differential count of P 40%, L 21%, E 4%, M 35%, and thrombocytopenia (45 × 109/L). Peripheral smear showed atypical monocytes suggestive of acute monocytic leukemia (AML) M5 type (Figure 4). Ultrasound of the whole abdomen showed mild hepatomegaly. HIV testing, VDRL, and TPHA were negative in both the patient and her partner. Patient was referred to Regional Cancer Centre for further evaluation and management, where bone marrow aspiration confirmed the diagnosis of acute monocytic leukemia (AML – M5).
Oral mucosa showing marked gingival hypertrophy. Genitalia showing two painless indurated ulcers, one on the right labia minora and another on the posterior fourchette with whitish mucoid vaginal discharge. Tissue smear from the edge of the ulcer showed atypical mononuclear cells. Peripheral smear showed atypical monocytes suggestive of acute monocytic leukemia (M5).


Discussion
Leukemia cutis is seen in around 20% of AML. 1 Cutaneous manifestations of leukemia can present as either specific or nonspecific skin lesions. Specific skin lesions are usually seen as erythematous papules, macules, nodules, tumors, or ulcerating plaques caused by the infiltration of leukemic cells. They are also referred to as leukemia cutis. Histopathology reveals distinctive features of leukemia cutis. Nonspecific skin lesions present as petechiae, purpura, ecchymosis, or infection. In addition to these, they may also present as erythema nodosum, various acute neutrophilic dermatoses like Sweet syndrome, pyoderma gangrenosum, subcorneal pustular dermatoses, erythema elevatum diutinum, leukocytoclastic vasculitis, and prurigo. Oral complications are mostly seen in acute leukemia than chronic leukemia. Gum hypertrophy seen in the absence of medication does serve as an important clinical clue for AML. Genital ulceration due to leukemic infiltrate is an uncommon primary feature in AML patients.2–6 Two cases each of scrotal and vaginal ulcers have been reported due to AML in literature.2–4,6 Apart from leukemic infiltrates, previous case reports describe vaginal ulcers following chemotherapy, 7 mimicking Behcet’s disease, 4 and due to infection. 5 Pathogenesis of ulceration in AML is either due to infiltration of leukemic cells or diminished local resistance to bacterial, viral and fungal infections, or hemorrhagic diathesis. Cutaneous disorders serve as a mirror of systemic involvement. The common causes of genital ulcers considered in young women are sexually transmitted infections. Leukemia cutis, though, a rare manifestation also needs to be added to the differential diagnosis of genital ulcers. Early diagnosis, treatment, and management are essential in such patients as it carries a poor prognosis. Simple diagnostic tests like peripheral smear and tissue smear aided in early diagnosis of this patient.
Footnotes
Acknowledgement
We would like to thank our laboratory technician Mrs. Subi C T, Department of Dermatology and Venereology, Government Medical College, Thrissur for her valuable help.
Authors’ contributions
We affirm that each contributor has participated sufficiently in the work to justify authorship. The manuscript has been read and approved by all the authors. The requirements for authorship as stated earlier in this document have been met. Each author believes that the manuscript represents honest work.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.