
Abstract
Background
In Kenya, HIV incidence and prevalence have declined. HIV rates are lower in rural areas than in urban areas. However, HIV infection is reported higher in men in rural areas (4.5%) compared to those in urban areas (3.7%).
Objectives
This study examined HIV knowledge, feelings, and interactions towards HIV-infected from 302 participants in rural Central Kenya.
Methods
Chi square tests and multivariable logistic regression analyzed variables of interest.
Results
Most participants exhibited positive feelings in their interaction with people living with HIV and AIDS (PLWHA). Association between HIV knowledge and socio-demographic characteristics revealed that the proportion of participants with a correct response differed by gender, age, level of education, and marital status (p < 0.05). Compared to those with inadequate knowledge of HIV/AIDS, participants with adequate HIV/AIDS knowledge were nearly three times as likely to disagree that PLWHA should be legally separated from others to protect public health (adjusted odds ratio: aOR (95% CI) (2.76 (1.12, 6.80).
Conclusions
HIV stigma continues to impact HIV prevention strategies particularly in rural Central Kenya. Culturally, appropriate interventions addressing HIV knowledge among those with lower levels of education, single, older, and male are warranted. Review of HIV policies separating high-risk populations from the general population is needed to reduce stigma.
Introduction
Globally, HIV/AIDS continues to be a leading cause of morbidity and mortality with almost 35 million people living with HIV. 1 Nevertheless, there has been progress in curbing the epidemic such that HIV incidence rates and AIDS-related mortality have progressively declined. Additionally, almost 12.9 million people globally are receiving antiretroviral medication, which is an improvement in HIV treatment. 1 In Kenya, HIV prevalence has declined from 14% in 1990 to 5.9% in 2015,2–4 while in 2011 there was a 40% decline in HIV incidence rates. 3 Nevertheless, HIV prevalence is still high among men and women in the 25–44 years age group and young women (4.5%) and men (1.5%) in the 15–24 age group as of 2012. 4 This signifies a need for continued upscale of HIV prevention, particularly targeting disproportionately affected age groups and women.
Relevant to this paper, HIV cases in rural areas are reported to be lower than in urban areas. However, HIV infection is reported higher in men in rural areas (4.5%) compared to those in urban areas (3.7%). 5 While documented evidence alludes to HIV rates being lower in rural areas compared to urban areas, as aforementioned, there is still a need to examine the existing rates in rural areas to enhance primary prevention strategies in order to minimize HIV incidence rates and reduce the burden of healthcare costs associated with HIV and AIDS treatment. Furthermore, given that the primary mode of HIV transmission in Kenya is heterosexual contact, 5 a concerted effort is warranted focusing on men in order to ensure HIV prevention among both sexes and not just women. Particularly, a closer assessment of levels of HIV knowledge and HIV stigma is necessary because it may have potential influence on HIV prevention.
Having accurate HIV knowledge is considered central to HIV prevention 6 to enhance consistent condom use, adherence to prescribed HIV medication, HIV testing and disclosure of serostatus to sexual partners. 7 Such knowledge can also improve perception towards HIV and interactions with people living with HIV and AIDS (PLWHA). 8 However, inaccurate HIV transmission knowledge can increase negative perceptions and attitudes resulting in stigmatization against those who are infected.9,10 Such stigmatization can negatively impact access to social support, which is a reported buffer against stigma, because people are afraid of disclosing their HIV status to others.11,12 Ultimately, HIV stigma can negatively impact success of HIV prevention strategies such as: HIV testing, HIV disclosure, medication adherence, and consistent condom use because of fear of rejection, ostracizing, domestic violence, and lack of privacy and confidentiality.13–18
Nevertheless, some studies have reported that having HIV knowledge does not definitively lead to perception of HIV risk, change in risky behavior, and/or uptake of HIV prevention strategies.19–24 For example, Orisakwe et al. 20 examined the relationship between HIV knowledge, willingness to be tested and HIV attitudes and perception at a clinical setting in South Africa. Authors found that even though participants scored high on the HIV knowledge survey, those scores did not translate to an increase in the number of participants who were willing to be tested for HIV. 20 In essence, there may be a gap between knowledge and behavior. Such participants are knowledgeable and willing to be tested but the action of testing maybe hindered by fear of finding out their status because of the perceived negative reaction from other people towards them if they are seropositive.
HIV stigma in Kenya has progressively decreased given the accelerated efforts to address HIV/AIDS in the past decade via social marketing messages and advocacy via the development of a 2008 HIV stigma strategic plan launched with the collaborative assistance of healthcare workers and religious leaders. 25 Additionally, a national AIDS strategic plan had already been instituted in 2006 to reduce AIDS-related mortality and increase universal access to HIV-related care. 25 Such efforts, albeit happened when HIV/AIDS was at an all-time high in Kenya, they have facilitated a concerted effort across the country to address HIV transmission. 25
However, there was some concern that stigma was prevailing at high levels in rural settings in Kenya. 25 Given that stigma is driven by societal norms that purport that HIV-positive individuals should be treated differently for going against certain norms, HIV-positive individuals can internalize such stigma and suffer from psychosocial issues such as alcoholism, depression, unemployment, and much more.16,26–28 To that end, to further minimize stigma and increase uptake of HIV prevention strategies in rural Kenya, it is paramount to incorporate culture and tradition 29 which may enhance comprehending stigma in those contexts with nuance. 30
The purpose of this paper is to examine factors that can influence feelings towards and interactions with those who are HIV-infected in a rural setting in Central Kenya. Even though HIV-related stigma in Kenya has reduced, more needs to be done to address negative perceptions and attitudes towards those who are HIV-positive in order to mitigate the negative impact of stigma on the success of HIV prevention strategies. Such a study has not been conducted in that region previously. Thus, reported findings are essential in that region to inform future large scale studies and/or interventions.
Methods
Study population
Eligible participants (n=302) from a rural community in Central Kenya, were recruited for the exploratory pilot study in 2013. Eligibility requirements were based on the following: male or female, 18 years and above and ability to understand English or Kikuyu. Approval was sought from the Ohio University’s Institutional Review Board and the African Medical Research Foundation’s (AMREF) Ethics and Scientific Review Committee in Kenya. The sample size for the study was calculated using Lwanga and Lemeshow 31 formula for sample size determination in health studies: n = (z2 pq)/d2 where n = sample size; z = the standard normal deviation which corresponds to the 95% confidence level (1.96); p = estimated prevalence of accepting attitudes toward those living with HIV/AIDS in rural Central Kenya (27%), derived from a nationally representative study in Kenya that utilized four items to assess attitude toward those living with HIV/AIDS; 32 q = 1 – p=(1 − 0.27 = 0.73); d = desired absolute precision (0.05). Using this formula, a minimum sample size of 302 participants was calculated.
Data collection
Data was collected in six randomly selected sub-locations in the priority region in Central Kenya. Sample allocation in each sub-locations was proportionate to the number of residents in each sub-locations. There was a reported increase in HIV prevalence in the county housing the priority region, from 3.6%to 4.4%in 2012.3,25 The increase presented concerns about primary prevention strategies, which prompted AMREF, who works collaboratively with the Constituency AIDS Control Council in that region, to reach out to the Ohio University researchers to collaborate on an exploratory study. No other study had examined the variables of interest prior to conducting the study nor has there been any other subsequent studies to date.
In each of the selected sub-locations, a central location (e.g. a market, an intersection, church, mosque or any other common benchmark) was identified and a random direction picked by spinning a pen. The number of houses between center and periphery in that direction were counted (and we had n = number of households). Finally, using a random number table, a random number between number 1 (one) and n (i.e. the number of houses counted) was selected. Eligible residents from the selected household were administered the questionnaire. If the household selected did not fulfill the selection criteria, the nearest next house was selected, and so forth.
In the households where an eligible person(s) was identified, the researcher and field assistants screened such individuals in a private room in the home or outside. The informed consent process was explained and a signature obtained before survey administration was conducted in private. This process was then repeated across all eligible persons within the household to avoid selection bias. Questionnaires were developed and administered in English and Kikuyu. The questionnaire was checked for face validity by AMREF’s staff and field assistants in that region and changes made prior to receiving IRB approval. Whereas English is a national language in Kenya, Kikuyu is the predominant local language in that region. The researcher was available at all times to assist participants experiencing challenges in comprehending and responding to the survey items. Participants were compensated with a KSH200.00 ($2.00) phone card.
Three field assistants in the research team were hired to assist as needed with the study. They all had higher level education and had previously worked on HIV/AIDS research and had received the appropriate research training. With regard to research training, the lead investigator met with the research assistants every day the week before data collection. They received training on reading questions to low level of education participants in their language of choice, explaining the nature of the study in the informed consent process, cultural sensitivity, administering phone cards to participants, responding to questions posed by participants and reporting any issue to the lead investigator. All three field assistants had previously worked with AMREF and the local Constituency AIDS Control Council in the priority region.
Measurements
HIV attitudes and perceptions
Items related to attitudes and perceptions towards PLWHA were selected from a previously validated instrument by Herek et al. 33 Respondents indicated their level of agreement with these statements on a four-point scale (1 = strongly disagree 2 = disagree 3 = agree 4 = strongly agree). A new variable was derived by recoding the four-point scale into a dichotomous variable (0 = disagree and 1 =agree) to calculate the proportion of participants agreeing or disagreeing with each item. In our study, this questionnaire had an acceptable internal consistency (Cronbach’s α = 0.71)
HIV knowledge
Characteristics of study sample (N = 302).

Indicates variables with missing values.
Association between HIV/AIDS knowledge and socio-demographic factors.

HS: high school.
p < 0.05; **p < 0.01;***p < 0.001 (x2 test).
Statistical analysis
Frequencies and proportions were used to describe the data. Chi square tests were used to examine the associations between socio-demographic characteristics and items related to attitudes and perceptions towards PLWHA as well as HIV/AIDS knowledge. Multivariable-adjusted logistic regression was used to obtain adjusted odds ratios and 95% CI for the association between attitudes and perceptions towards PLWHA and HIV/AIDS knowledge scores. A p-value of 0.05 was considered statistically significant. All analyses were conducted using SPSS version 22.0 (IBM Corp, Armonk, NY, USA).
Results
Characteristics of the study population (n = 302) are shown in Table 1. In terms of age distribution, slightly higher proportion of participants was in 31–39 years (26.5%) followed by 25–30 (23.8%), 50 and above (20.9%), 40–49(18.5%) and 18–24 (10.3%). Half of the study population was female. The majority of the sample was married, but unmarried (27.8%) and divorced or widowed participants (7.9%) were represented as well. Nearly three quarters of study participants raise children. Greater proportion of participants had less than high-school education (45.0%) followed by those having high-school level education (40.4%) and greater than high school (14.6%). Nearly 66% of the study participants were unemployed at the time of the survey.
Association between attitudes and interactions with PLWHA and socio-demographic characteristics.
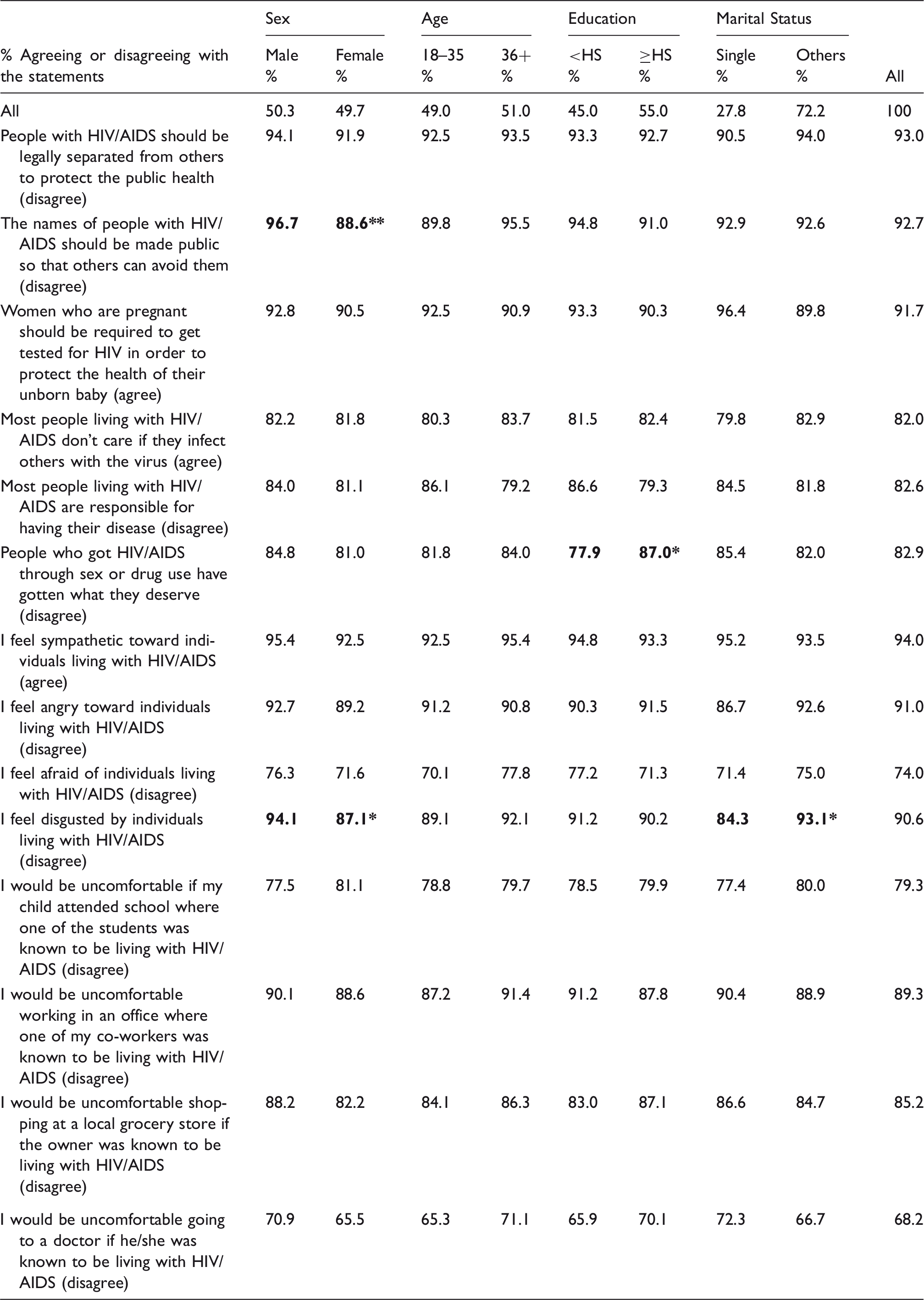
HS: high school.
p < 0.05; **p < 0.01; ***p < 0.001 (x2 test).
Table 3 summarizes the association between HIV knowledge and socio-demographic characteristics. The proportion of participants with a correct response to the statement that teenagers and young adults are at high risk of being infected with HIV differed by age (p < 0.001) and by level of education (p < 0.01). Similarly, the percentage of participants who correctly responded to the question that HIV/AIDS can be transmitted through mosquito bites differed by level of education (p < 0.05). Compared to females, slightly higher proportion of males correctly responded to the statement that a person can get HIV even if he/she has only one unprotected sexual encounter with an HIV-infected person (p < 0.05). Compared to older participants, higher proportion of participants in the 18–35 age category correctly responded to the statement that in general it takes three to six months for a person with HIV to develop AIDS (p < 0.01). The percentage of participants who correctly responded to the statement that a person with HIV can look and feel healthy differed by level of education (p < 0.05). Compared to unmarried participants, greater proportion of currently or previously married participants correctly responded to the statement that a pregnant woman with HIV can pass the virus to her baby (p < 0.05). The percentage of participants who correctly responded to the statement that any time blood is drawn it is tested for HIV differed by gender (p < 0.05).
Associations between attitudes and interactions with PLWHA and HIV-related knowledge scores.
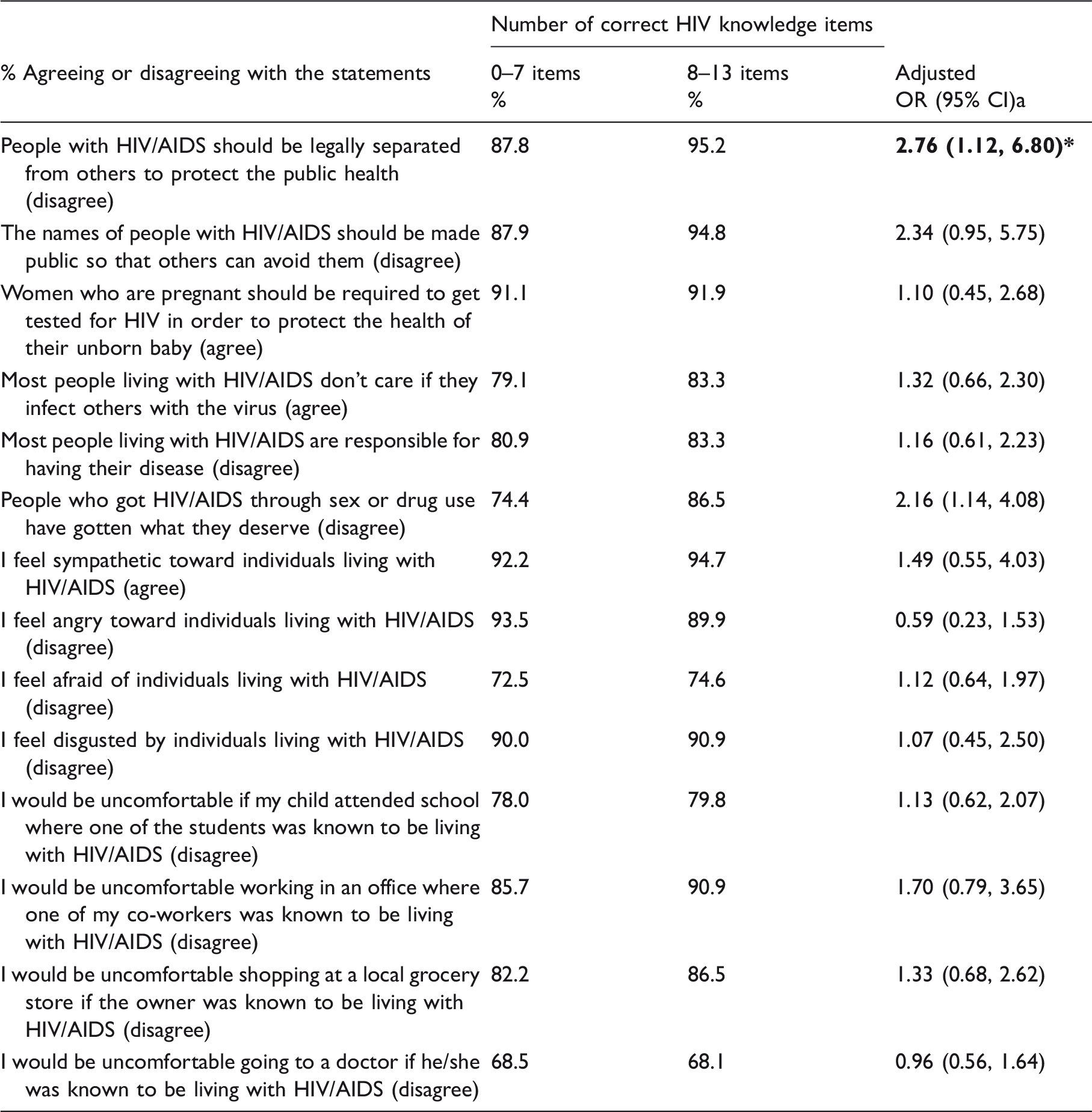
Adjusted for sex, age, education and maital status.
p < 0.05
Discussion
The purpose of the current paper was to examine the factors that can influence knowledge, perception, and attitudes towards those who are HIV-infected in a rural Central Kenya. In general, findings reveal that the majority of the sample group had positive perceptions and attitudes towards PLWHA. This may be attributed to the accelerated efforts to address HIV/AIDS in the past and the existence of an HIV stigma strategic plan. 25 Of significant interest is the finding on the association between items related to HIV knowledge scores, attitudes and perceptions towards PLWHA, that revealed that participants who scored high on the HIV knowledge assessment disagreed with separating PLWHA from the general population to protect public health. This finding is consistent with other studies that have shown that increased stigma and discrimination are associated with low levels of HIV transmission knowledge.10,39
The relationship between HIV knowledge and socio-demographic factors revealed that knowledge was significantly associated with the age, gender, level of education, and marital status. A high level of HIV knowledge as evidenced by correct response to HIV knowledge items was among those whose level of education was higher than high school and belonged to the 18–35 age group. This may indicate that those who are young and those who have a higher education may have more awareness of HIV transmission and prevention via mass media and other interventions targeting young adults. Other studies found similar findings with regard to the association between HIV knowledge and age and level of education.24,40
The association between attitudes, perceptions, and socio-demographic factors revealed that most of the participants were accepting of the HIV-infected and disagreed with statements related to: making public names of HIV-positive, disgusted by PLWHA and PLWHA have gotten what they deserve if they got infected via sex or drugs. Given the reports that HIV stigma is prevalent in rural areas, 25 these findings indicate that stigma maybe decreasing in some rural settings. A greater proportion of participants’ attitudes and perceptions towards PLWHA were associated with gender, level of education, and marital status. With regard to level of education, Hamra et al. 41 found that stigma was more common among those with lower level of education in an urban setting in Kenya. In this paper, compared to those with level of education lower than high school, a greater proportion of those with higher than high-school level of education disagreed that PLWHA got what they deserved.
Overall, these findings are critical to the continued success of HIV stigma prevention strategies. Particularly, given the influence of HIV knowledge, feelings, attitudes towards and interactions with PLWHA, advocating for an amendment to current HIV-related policies that identify and ultimately separate high-risk populations from the general population is paramount. Policies that focus on identifying PLWHA as a vulnerable group that is separate from the general population can contribute to social exclusion.10,42 Ultimately, such exclusion can enhance stigma and discrimination against PLWHA and hamper the success of HIV prevention strategies.
Instead, HIV prevention programs and HIV-related policies should focus on (1) emphasizing that HIV-positive individuals are useful members of the community suffering from a chronic disease 10 and (2) everyone in the general population is at risk of HIV transmission, in order to enhance uptake of HIV prevention across the board and minimize stigma and discrimination. 10 Such efforts can be strengthened with the assistance of community leaders (e.g. politicians, religious leaders, village chiefs, district commissioners/officers) who can facilitate community mobilization through events such as HIV testing (whereby community leaders get tested too), fundraising for local HIV programs and other HIV awareness campaigns that are culturally appropriate.29,30
Limitations
Findings from the study rely on self-reported information regarding attitudes, perceptions and HIV knowledge, which could be biased towards socially acceptable responses. Also, those households that were not visited may be subject to selection bias. In addition, participants from the chosen household who were at work or in school were not interviewed. Thus, findings from this study may not be generalizable to all rural areas in Kenya given the differences in socio-demographic and cultural factors. The study is also exploratory and cross-sectional which limits ability to ascertain causality among chosen variables. However, the associations between the variables provide insight for a follow-up long-term study and intervention.
Conclusion
Overall, findings reveal that the majority of the sample group had positive perceptions and attitudes towards PLWHA. Such findings greatly support the ongoing efforts to address HIV stigma and discrimination against those who are HIV-positive in Kenya. In spite of the progress, there is a need to have targeted programs in that region that focus on increasing HIV knowledge among those with lower levels of education, are single, older, and male in a culturally relevant manner. One strategy to reach out to those groups is to perhaps integrate interventions within existing programs such as primary care or maternal and child health or home-based voluntary and counseling programs.
While HIV knowledge does not always signify a change in targeted behavior, there is evidence to show that having accurate HIV knowledge is related to enhancing the success of HIV prevention strategies such as consistent condom use, adhering to prescribed HIV medication, HIV testing and disclosure of serostatus to sexual partners while improving perceptions and attitudes towards PLWHA. Future studies can conduct a longitudinal study that follows the priority group over time to measure changes in perceptions and attitudes towards PLWHA.
Finally, a review of HIV policies that separate high-risk populations from the general population is paramount across the board in order to minimize stigma and discrimination. As aforementioned, it is important to emphasize that PLWHA are useful members of a given society and that everyone in the society is collectively at risk of acquiring HIV infection.
Footnotes
Acknowledgements
We would like to extend thanks to study participants, co-authors, research assistants, Othaya District Commissioner and Officer, Othaya chiefs and AMREF-Kenya. Contents of the paper are solely the responsibility of the authors and do not necessarily represent any official view. Special thanks are extended to Jocelyn Nyambura, Eliud Gichuki and JaneWachira.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was sponsored by funding provided from the College of Health Sciences and Professions, Ohio University, Athens, OH, USA.