
Abstract
The incidence of disseminated Mycobacterium avium complex (MAC) infection in HIV patients has fallen markedly since the introduction of effective antiretroviral therapy (ART). However, current guidelines still recommend primary prophylaxis. We conducted a retrospective cohort study in a university-affiliated hospital from January 1998 to January 2014. During that period, HIV patients who had at least one CD4 cell count below 50 cells/mm3 and had been treated with ART were enrolled. We compared incidence of disseminated MAC infection in the 12 months after the first CD4 cell count below 50 cells/mm3 between prophylaxis and nonprophylaxis groups. A total of 157 patients were enrolled and the total observation period was 144 patient-years (PY). Thirty-three patients (21%) received primary MAC prophylaxis. The initial CD4 cell count of the prophylaxis group was lower than that of the nonprophylaxis group (P = 0.024), but the proportion of patients who reached a CD4 cell count >100 cells/mm3 (P = 0.234) and were virologically suppressed (P = 0.513) 12 months after ART commencement was not different in the prophylaxis and nonprophylaxis groups. The incidence of MAC did not differ significantly between the groups (3.4/100 PY versus 0.8/100 PY, P = 0.368). Routine MAC prophylaxis may be not required in the era of effective ART.
Introduction
Disseminated Mycobacterium avium complex (MAC) infections were one of the most common opportunistic infections in patients with acquired immunodeficiency syndrome (AIDS) before effective antiretroviral therapy (ART) became available. 1 Before effective ART, 21% of patients with AIDS developed disseminated MAC infection within a year of diagnosis and 43% within two years.2,3 This infection is itself an independent risk factor for mortality.4,5
Several randomized studies have shown that prophylaxis with macrolides (clarithromycin or azithromycin) or rifabutin decreases the incidence of disseminated MAC infection, one of the studies also demonstrating a reduction in deaths.6–9 Based on those studies, current guidelines recommend prophylaxis for disseminated MAC infection in human immunodeficiency virus (HIV) patients whose CD4 cell count is below 50 cells/mm3.10,11 After the advent of effective ART, opportunistic infections, including disseminated MAC, fell remarkably, and several studies demonstrated that it is safe to discontinue primary prophylaxis against MAC if an increased CD4 cell count is sustained.12,13 As a result of these studies, the guidelines recommend stopping primary prophylaxis at a CD4 cell count >50–100 cells/mm3 for over three months.10,11 According to these recommendations, every HIV patient who starts ART at a CD4 cell count <50 cells/mm3 should receive MAC prophylaxis for at least three months.
However, the studies that initiated primary prophylaxis against MAC were conducted prior to the era of effective ART, which has itself reduced the incidence of MAC massively, 14 and it is uncertain whether the prophylaxis would decrease the incidence of disseminated MAC infection in patients receiving ART.15–17 One study conducted after the introduction of effective ART reported that azithromycin still decreased MAC infections, 16 and at that time the virologic suppression rate was at most 20–30%. However, in a recent study prophylaxis made no difference in patients who received ART and were virologically suppressed even though their CD4 cell count had fallen to <50 cells/mm3. 15
We compared the incidence of disseminated MAC infection with and without the use of MAC prophylaxis in HIV patients receiving ART to evaluate the effectiveness of primary prophylaxis against MAC in an era of effective ART.
Methods
This is a retrospective cohort study in a single center. We reviewed all HIV patients aged over 18 years who visited the HIV clinic at Seoul National University Hospital (a university-affiliated tertiary hospital, Seoul, Korea) between January 1998 and January 2014. Patients were included who had had at least one CD4 cell count <50 cells/mm3 and had initiated ART, resumed it if they had been receiving it, or continued on it. ART was defined as triple antiretroviral drug therapy including one protease inhibitor or nonnucleoside reverse transcriptase inhibitor or integrase inhibitor. We excluded patients who took any antimycobacterial agent other than isoniazid prophylaxis for tuberculosis. We examined patients’ demographic characteristics, CD4 cell count, HIV RNA load, previous history of ART, nontuberculous mycobacterial infection including MAC infection, other opportunistic infection at the time when their CD4 cell count was <50 cells/mm3, and MAC prophylaxis status after CD4 cell count was <50 cells/mm3. We investigated the development of disseminated MAC infection until 12 months from the time of their first CD4 cell count <50 cells/mm3. We collected the CD4 cell counts, which were usually checked every three months with HIV RNA viral load over the 12-month period (if a count was not available after a three-month interval, we used the CD4 cell count nearest in time) and compared the changes of CD4 cell count in the MAC prophylaxis and nonprophylaxis groups over the 12 months. Disseminated MAC infection was defined as a positive culture of MAC from blood or bone marrow. If there was generalized lymph node enlargement with suggestive symptoms and signs of disseminated MAC infection, recovery of MAC from a lymph node was also defined as disseminated MAC infection. Observation was ended at last visit, death, diagnosis of disseminated MAC infection, or nontuberculous mycobacterial infection other than MAC, or 12 months after the first CD4 cell count <50 cells/mm3, whichever occurred first. We calculated the incidence of disseminated MAC infection per 100 patient-years (PY) and compared the values in patients with and without prophylaxis. Continuous variables are reported as mean (standard deviation) or median (interquartile range [IQR]) and categorical variables as number (percentage). Between-group differences were assessed using the t-test, Wilcoxon rank sum test, Chi square test, or Fisher’s exact test. CD4 cell count changes over the 12 months were compared by repeated measures ANOVA. We used SPSS for Windows (version 19.0 software package; SPSS Inc., Chicago, IL, USA). The study was approved by our hospital’s Institutional Review Board (H-1411-027-623).
Results
Characteristics of study population
Over the study period 1373 HIV patients visited our clinic and were assessed for eligibility; there were 196 patients with at least one CD4 cell count <50 cells/mm3 and who received ART. Excluding 39 patients who took antimycobacterial agents due to tuberculosis during the 12 months of observation, 157 were included in the final analysis. Three patients died within the 12-month period, 16 were lost to follow-up, and 138 patients were observed for 12 months. The total observation time was 144 PY. Most of the patients were men (96%) and the median age was 38 years (IQR, 19–66). Median CD4 cell count was 20 cells/mm3 (IQR, 11–49 cells/mm3). Forty-five percent of the patients presented with opportunistic infections at the time when their CD4 cell count was <50 cells/mm3. At that time 114 (73%) patients had received ART in the past, 30 (19%) had not, and 13 (8%) were receiving ART currently. Patients who were not receiving ART started or restarted on ART within a median duration of eight days (IQR, 3–22). Among the patients with ongoing ART, nine continued on it and four changed to other regimens. Two patients were diagnosed with disseminated MAC infection over the 12-month observation, an overall incidence of 1.4/100 PY.
Comparison of patients with prophylaxis and without prophylaxis
Comparison of baseline characteristics of patients with and without MAC prophylaxis.

ART: antiretroviral therapy; IQR: interquartile range; MAC: Mycobacterium avium complex.
Data are no. (%).
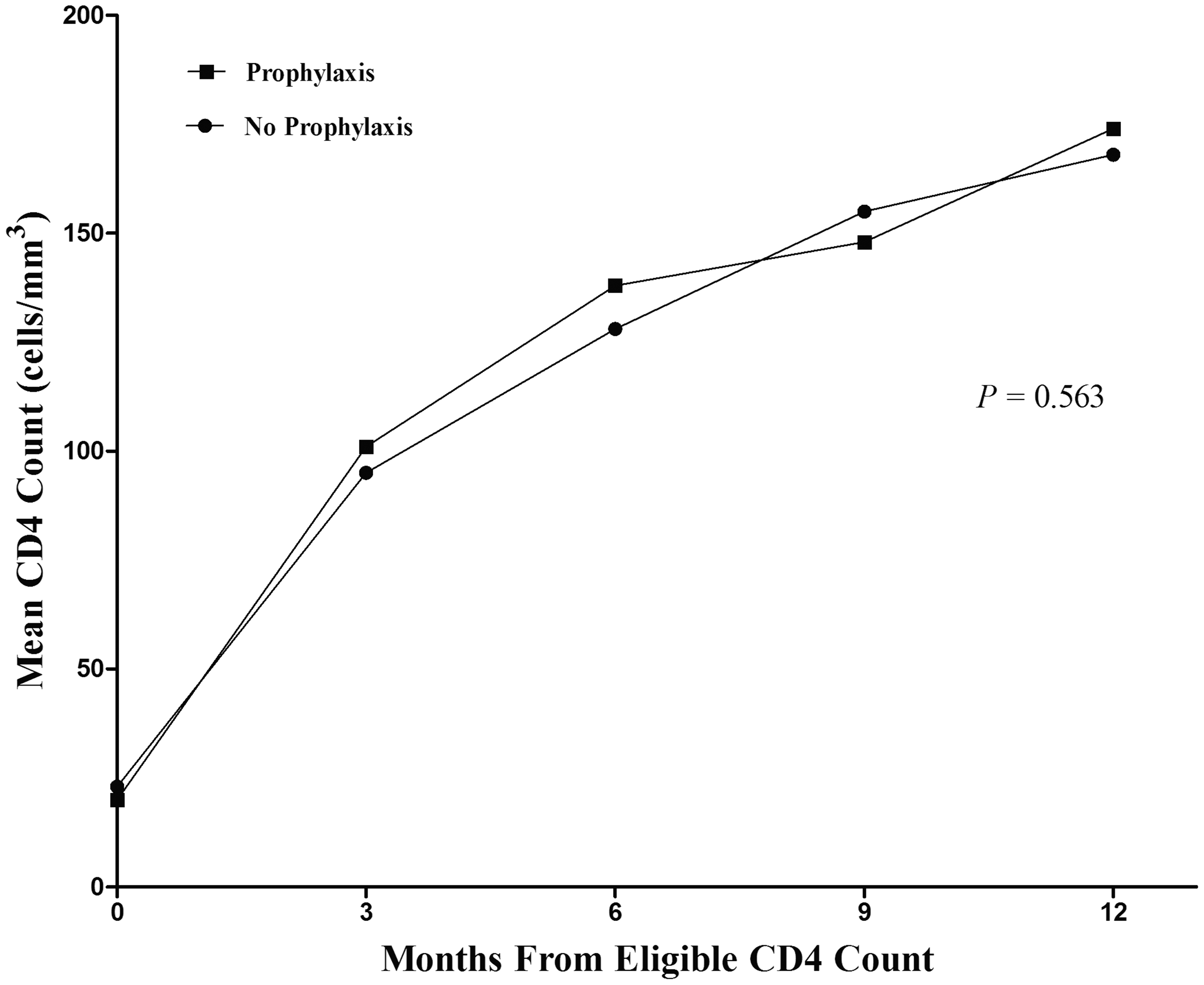
Average CD4 cell count at baseline and during follow-up in patients with prophylaxis and without prophylaxis.
Outcome of disseminated MAC infection with prophylaxis.
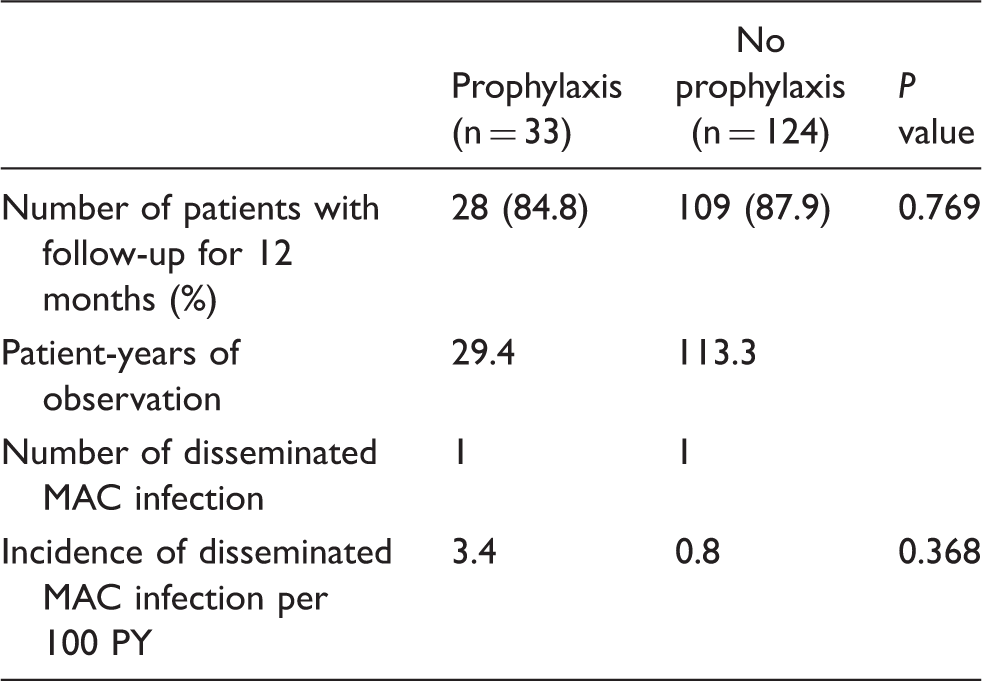
MAC: Mycobacterium avium complex; PY: patient-years.
MAC prophylaxis
Thirty-three patients (22%) had been prescribed MAC prophylaxis for a median duration of 64 days (IQR, 30–307). Median day from eligible date to start prophylaxis was 15 (IQR, 5–24). Twenty-nine patients were prescribed clarithromycin, and the remaining four were prescribed azithromycin. Twenty-four percent (8/33) suffered side effects due to the prophylactic medication; six had gastrointestinal trouble, and among them two ceased the drug. One patient complained of a change of taste and went on medication, one experienced bone marrow suppression and had to stop the medication. The median CD4 cell count at the time of prophylaxis discontinuation was 110 cells/mm3 (IQR, 48–150) and only one patient achieved a stable CD4 cell count (>100 cells/mm3 for three months) among the prophylaxis group at the time of prophylaxis discontinuation.
Cases of disseminated MAC infection
Case 1
A 26-year-old man visited the outpatient clinic with fever and epigastric pain for five days. He was diagnosed with HIV infection two years previously but did not visit hospital after that. Four weeks ago, he had started ART and azithromycin prophylaxis against MAC when his CD4 cell count was 4 cells/mm3 and HIV RNA viral load was 3.61 × 103 copies/mL. His abdominal computed tomography (CT) scan showed hepatosplenomegaly and multiple enlarged intra-abdominal lymph nodes and chest CT showed multiple enlarged bilateral cervical lymph nodes. An aspirated specimen from the left supraclavicular lymph node grew nontuberculous mycobacteria and was identified as Mycobacterium intracellulare by molecular techniques. His CD4 cell count was 136 cells/mm3 five weeks after ART. Around that time he began azithromycin and ethambutol for treatment of disseminated MAC infection.
Case 2
A 29-year-old man visited the outpatient clinic with aggravating abdominal pain for one day. He was diagnosed with HIV and had initiated ART three weeks prior in our institution. His CD4 cell count was 20 cells/mm3 and HIV RNA viral load was 8.12 × 103 copies/mL. He recalled that he had abdominal pain at this time, but thought it was not serious enough to inform the doctors. His CD4 cell count was 16 cells/mm3 three weeks after ART. He had diffuse abdominal tenderness and rebound tenderness on physical examination and fever developed one day after admission. His abdominal CT revealed hepatosplenomegaly and multiple enlarged intra-abdominal lymph nodes. He underwent bone marrow and intra-abdominal lymph node aspiration and both grew nontuberculous mycobacteria identified as Mycobacterium avium by molecular testing. Two weeks after admission he started clarithromycin, ethambutol, and ciprofloxacin for the treatment of disseminated MAC infection.
Discussion
We found that there was no difference in the incidence of disseminated MAC infection between the prophylaxis and nonprophylaxis groups of HIV patients with CD4 cell counts <50 cells/mm3 receiving effective ART. The overall incidence of disseminated MAC infection was 1.4/100 PY in our study population. The incidence and prevalence rates of MAC infections vary with time, location, and disease definition. In the past, most studies of opportunistic infections in HIV patients were performed in developed countries, but many clinical trials are now being conducted in developing countries. In East Asia there have been a few studies of opportunistic infections in HIV patients.17,18 Among more than a thousand HIV patients in a tertiary hospital in China the prevalence of MAC infection was reported to be 11%. 18 In our previous study of all opportunistic infections in HIV patients, the prevalence of atypical mycobacterial infection in HIV patients was 3%. 19 However, it is hard to compare rates in different countries because the units are not standardized and, as mentioned above, disease definitions are not the same. A study of a similar population (patients with CD4 cell counts <50 cells/mm3 and on ART) in the USA reported an incidence of all MAC infections (disseminated and localized) of 0.6/100 person-months, which is considerably higher than in the present study. Another cohort study including six European countries and the USA found a lower incidence than ours, of 5.8/1000 PY. 20
Early discontinuation (before reaching a certain CD4 level for a certain length of time) of prophylaxis against opportunistic infections has been mostly studied in Pneumocystis jirovecii pneumonia and a systematic review has concluded that early discontinuation is safe in virologically suppressed HIV patients. 21 Although there have been few studies of withholding primary MAC prophylaxis some experts have suggested that routine MAC prophylaxis is not necessary based on the evidence that disseminated MAC infection has decreased markedly in the era of effective ART, and no MAC infections have developed in virologically suppressed patients despite their lower CD4 cell counts (<50 cells/mm3).15,22 Compliance with the recommendation for MAC prophylaxis seems to be low in clinical practice despite the recommendation. Primary prophylaxis against MAC has never been strictly followed in Switzerland, and only 20–40% of eligible patients have received MAC prophylaxis in Germany and the USA.22–25 In the present study, only a fifth (33/157) of the patients received prophylaxis, and of these only one fulfilled the criterion recommended for discontinuation. We do not know the reason for the lack of compliance with the recommendation, but it could be the very low incidence of the disease in the era of effective ART. In addition, gastrointestinal side effects of high-dose macrolides may interfere with the patient’s adherence to ART, and maintaining viral suppression and imposing a high pill burden have negative effects on ART adherence. Weekly azithromycin seems to be costly without apparent benefit, considering the very low incidence of disseminated MAC infections particularly in the era of effective ART.
A recent study in the USA examined the incidence of MAC infection among patients with CD4 cell counts of <50 cells/mm3 receiving combination ART and did not find a difference in the incidence of MAC between the prophylaxis and the nonprophylaxis groups. 15 However, the authors did not show that the two groups had a comparable risk of developing MAC infection as they mentioned they did not have information on patient adherence to ART. In other words, physicians may have decided to provide prophylaxis against disseminated MAC infection not only based on CD4 cell counts but also on other considerations such as compliance, family support, and previous medical history, which could have affected responses to ART. This practice could have led to selection bias in evaluating the effectiveness of prophylaxis accurately. In the present study, the initial CD4 cell count was lower in the prophylaxis group, which means that more of those patients could be at risk of developing disseminated MAC infections than those in the nonprophylaxis group. However, subsequent changes in CD4 cell count and the proportions of patients reaching CD4 cell count >50 cells/mm3 in the 12-month observation period did not differ between the two groups, which suggests that they had similar responses to ART and comparable risks of developing disseminated MAC infection.
Before the introduction of effective ART, MAC infections were generally disseminated and accompanied by systemic symptoms and signs, such as fever, weight loss, night sweats, and severe anemia, sometimes with focal signs or symptoms depending on the organs involved.26,27 After ART, localized presentation became more prevalent,16,28,29 possibly because new forms of MAC-infected patients whose immune systems could not fully recover but were able to prevent the infection from disseminating. Alternatively, asymptomatic (subclinical) MAC infections present before the initiation of effective ART may have presented as lymphadenitis as the immune system reconstituted; this process is referred to as unmasking of immune reconstitution inflammatory syndrome (IRIS). In our study, both of the patients who developed disseminated MAC infection had symptoms within four weeks of the start of ART. They may have acquired de novo infections, but they may have harbored subclinical infections that became evident once their immune function was restored after effective ART. The incidence of MAC infections has been shown to increase for up to three months after the start of ART, and this has been attributed to unmasking of IRIS.20,30 Whether MAC infection in the early period after ART is prevented by MAC prophylaxis has not been studied, but azithromycin prophylaxis has been shown to decrease localized MAC lymphadenitis which is a possible presentation of IRIS. 16
Our study has several limitations. This study was conducted in a single center and our findings cannot be generalized. It may have underestimated the incidence of disseminated MAC infections because it was a retrospective study and blood culture was not performed routinely in patients with fever and/or CD4 cell count <50 cells/mm3. We could not prove the ineffectiveness of the prophylaxis with high statistical power because the population of HIV patients with CD4 cell count <50 cells/mm3 was small, and disseminated MAC infection developed very rarely. However, a larger randomized controlled trial to confirm our results may be difficult to carry out because the incidence of disseminated MAC infection is very low in the era of effective ART.
In summary, we found no difference in disseminated MAC infection as a result of MAC prophylaxis in HIV patients receiving ART. While this study has statistical limitations, our finding provides experiential support for the view that MAC prophylaxis is not be needed in such patients.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.