
Abstract
Immunoglobulin G4 (IgG4)-related disease (IgG4-RD) is an immune-mediated condition characterized by infiltration of the involved organs by IgG4-bearing plasma cells. The prevalence of autoimmune diseases, associated with or occurring in patients with human immunodeficiency virus (HIV) infection, has been increasing. We describe a 58-year-old man with an undiagnosed HIV infection, which presented as chronic cervical lymphadenopathy with an elevated serum IgG4 and a very high IgE. Histologically, lymph nodes showed expanded sinusoids and burnt-out germinal centers with increased plasmacytic infiltration and collagen fiber deposition. The absolute number of IgG4+ plasma cells and the IgG4+/IgG+ plasma cell ratio was increased. The lymph nodes were enlarged and clinically the patient improved after steroid treatment. Nine months later, he was diagnosed with acquired immune deficiency syndrome, following presentation with a cavitary left lung lesion. Immunohistochemical studies on the previously resected lymph node revealed complete absence of CD4+ T-lymphocytes and increased CD8+ T-lymphocytes. The pathologic findings met the criteria of both HIV infection and IgG4-related lymphadenopathy. Our case demonstrates that further investigations for underlying HIV infection in a case of IgG4-RD are critical, especially when extremely elevated IgE is concomitantly present.
Case report
A 58-year-old Taiwanese man presented in January 2014 with a six-month history of posterior neck lumps. On physical examination, multiple tender and mobile lymph nodes were palpable bilaterally on the neck. Computed tomography (CT) of the neck revealed bilateral enlarged lymph nodes in the submandibular and upper neck regions (Figure 1(a)). Routine laboratory investigations were within normal limits, except for anemia (haemoglobin concentration: 11.6 g/dL), thrombocytopenia (platelet count: 133,000/µL) and eosinophilia (14.3%). Excisional lymph node biopsy showed interfollicular lymphoplasmacytic infiltrate and storiform fibrosis (Figure 2(a) and (b)). The percentage of immunoglobulin (Ig) G4+/IgG+ plasma cells was more than 40%, with an absolute number of IgG4+ plasma cells of up to 160 per high-powered field (Figure 2(c) and (d)). Serum IgG level was 3390 mg/dL (reference range: 700–1600 mg/dL), IgG4 1160 mg/dL (reference range: 3–201 mg/dL), and IgE 70,800 IU/mL (reference range: <100 IU/mL). He denied allergic disorders. Thus, IgG4-related lymphadenopathy was considered as the most likely diagnosis. He was started on treatment with prednisolone 20 mg/day, and gradually tapered over time, following which IgG4 and IgE levels declined moderately (down to 461 mg/dL and 22,700 IU/mL, respectively). At nine months after the diagnosis of IgG4-RD, he was admitted due to a cavitary left lung lesion. Serological test for HIV was positive. HIV viral load was 77,838 copies/mL, and CD4 cell count was 38 cells/mm3. We reexamined his previous lymphadenectomy specimens and found a complete absence of CD4+ T-lymphocytes but increased CD8+ T-lymphocytes (Figure 2(e) and (f)). Histopathological specimens were negative for human herpes virus 8 immunohistochemical staining. A diagnosis of coexistent IgG4-related disease (IgG4-RD) and HIV lymphadenitis was made. After three months of an antiretroviral therapy (ART) regimen without steroids, the follow-up IgG4 level increased to 1080 mg/dL, but no clinically palpable lymphadenopathy was found. Five months later, cervical lymphadenopathy with rising IgG4 levels recurred and steroids were prescribed again. The cervical lymphadenopathy gradually declined. Two years after the initial CT, a follow-up CT scan showed marked regression of cervical lymphadenopathy (Figure 1(b)). At the present time, the patient is continuing on prednisolone 10 mg/day for the control of IgG4-RD.
(a) Computed tomography of head and neck performed in 2014, demonstrating multiple borderline-enlarged lymph nodes in the bilateral submandibular and upper neck region (level I and level II). (b) Computed tomography performed in 2016, revealing marked regression of enlarged lymph nodes. Pathological features of lymph node biopsy. (a, b) The interfollicular areas showing lymphoplasmacytic infiltration and storiform fibrosis (H&E, ×40 (a) and ×400 (b)). (c) Immunostaining for IgG showing increased IgG+ plasma cells (400 ×). (d) Immunostaining for IgG4 revealing a moderate number of IgG4+ plasma cells are present. The IgG4+/IgG+ ratio was more than 40%. The number of IgG4+ plasma cells is 120–160 per high-power field (400×). (e) Immunostaining for CD4+ T-lymphocytes showing marked depletion of CD4+ T-cells (400×). (f) Immunostaining for CD8+ T-lymphocytes demonstrating increase in CD8+ T-cells. Significant reversion of CD4/CD8 cell count ratio was observed (400×).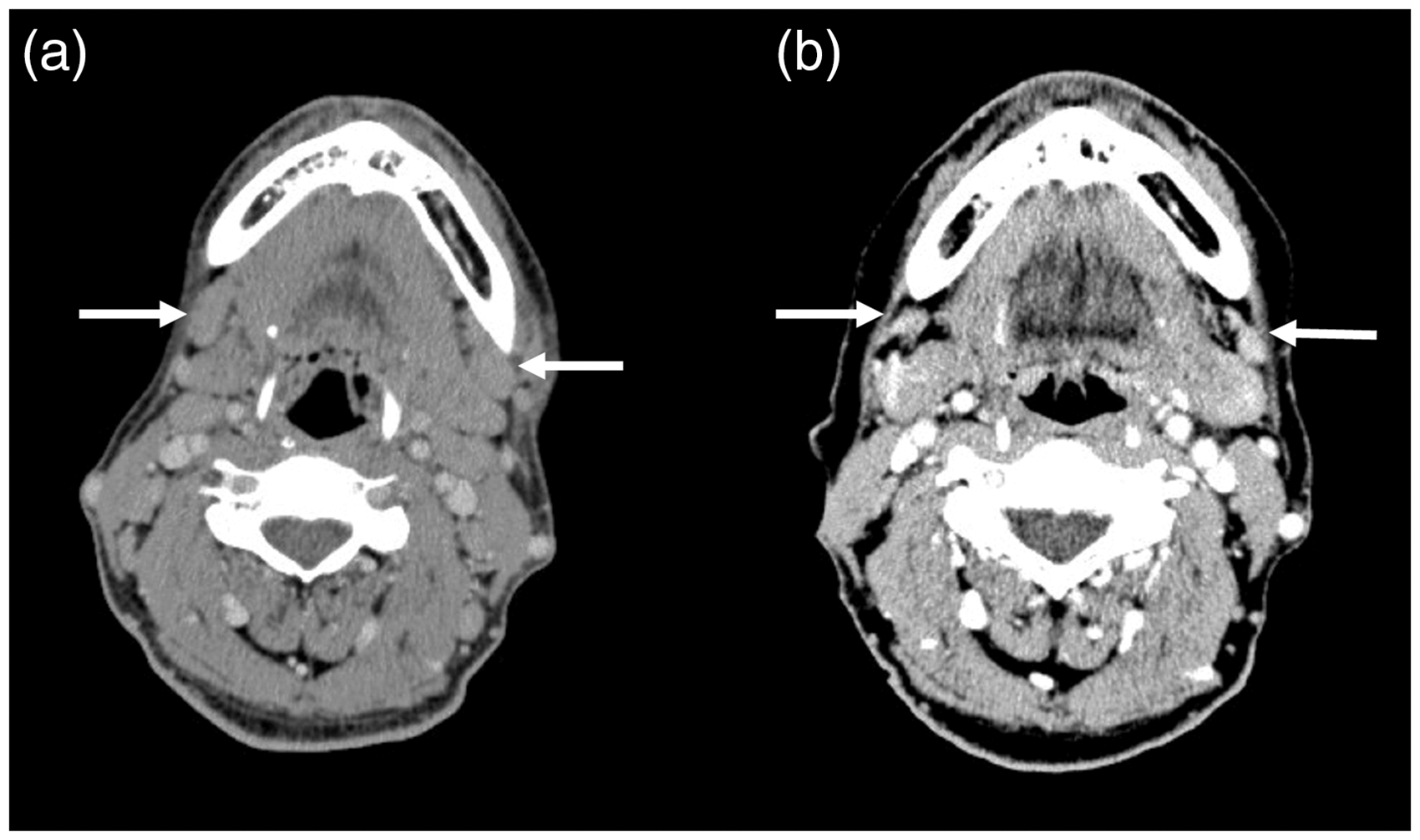

Discussion
IgG4-RD is an immune-mediated condition characterized by tissue infiltration of lymphocyte and IgG4-positive plasma cells, storiform fibrosis, often elevated serum levels of IgG4, and a prompt response usually to oral steroids.1–3 The head and neck region is the second most common site for the development of IgG4-RD. 4 Lymphadenopathy is observed in up to 80% of IgG4-RD and may recur or progress to involve multiple organ systems. 2
Peripheral lymphadenopathy is a common clinical finding among HIV-infected individuals and may occur at any stage of HIV infection. 5 The differential diagnosis of peripheral lymphadenopathy in the HIV-infected population typically falls into one of three major categories: infection, malignancy, or reactive change. 6 To the best of our knowledge, this is the first case of an undiagnosed HIV-infected patient presenting with palpable cervical lymphadenopathy due to with IgG4-RD. The patient met the 2011 comprehensive diagnostic criteria for IgG4-RD based on the organs affected, involved tissues enriched with IgG4-positive plasma cells, and high serum IgG4 concentration. 7
Although the pathogenesis of IgG4-RD remains poorly understood, several studies have suggested a causative immune-mediated role for type 2 helper T (Th2) cells. 2 About 30–50% of IgG4-RD patients have a history of allergy; eosinophilia and/or elevated serum IgE levels are observed. 8 High serum IgE concentrations, sometimes higher than 10 times the upper limit of normal, are also common. 1 However, in our non-atopic patient with IgG4-RD, a very high IgE concentration (more than 700 fold) was unusual. Extremely elevated IgE levels greater than 5000 IU/mL have been reported in association with a variety of causes, including atopic dermatitis, HIV infection, hyper-IgE syndrome, lymphoreticular malignancy, and IgE myeloma. 9 Based on our case, underlying HIV infection should be kept in mind when a patient with IgG4-RD shows marked elevation of serum IgE.
Immunohistologic alterations of lymph nodes in HIV infection represent a dynamic process characterized by initial follicular hyperplasia that ultimately progresses to a burnt-out lymphocyte depletion endpoint. 10 Marked reduction in CD4+ T-lymphocytes and a significant increase in CD8+ T-lymphocytes within germinal centers are highly suggestive of HIV infection. 10 Altered CD4+/CD8+ cell count ratio has been observed in a variety of non-HIV situations, including cytomegalovirus infection, following transplantation, during acute illness, and due to malnutrition. 11 Our patient had no clinical manifestations of these diseases. Thus, his enlarged lymph node could have been associated with HIV infection at that point. In the present case, lymph node enlargement with an elevated IgG4 level recurred five months after initiating ART, but resolved after resuming steroids. The evolution of lymphadenopathy with a striking clinical response to steroid therapy led to the diagnosis of IgG4-RD coexistent with HIV infection.
In conclusion, we report an unusual case of IgG4-related cervical lymphadenopathy as the initial manifestation of HIV infection. This case highlights the importance of differentiating IgG4-related lymphadenopathy from HIV lymphadenitis and its clinical relevance and treatment implications, when they co-exist. HIV infection should always be considered in cases of IgG4-RD, especially when extremely elevated IgE is concomitantly present.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Informed consent to publish this report was obtained from the patient. This study was approved by the local Institutional Review Board of Chang Gung Memorial Hospital (IRB No: 201600830A3).