
Abstract
Ukraine has the second largest HIV epidemic in Eastern Europe/Central Asia. This study characterizes the demographics of HIV-infected women in the Lviv region of western Ukraine, patterns in their clinical presentation, and factors associated with delays in seeking care. A retrospective chart review was conducted of 622 HIV-infected women who registered for HIV treatment at the Lviv AIDS Center between 2008 and 2013. A total of 81.6% of women were infected through heterosexual transmission and the remaining 18.4% through intravenous drug use. Slightly less than half (45.4%) was between 26 and 35 years old. Slightly more than half (56.7%) listed their residence in a city, 22.6% in villages. One-third (30.0%) of all women presented with AIDS, and 37.7% presented with symptomatic conditions. Women diagnosed with HIV during antenatal care experienced a median delay of 34 days between diagnosis and registration, compared to 87.5 days for nonpregnant women tested in the context of intravenous drug use. Overall, HIV-infected women in western Ukraine experience time delays in care, and often present with advanced HIV disease and secondary complications. Linkage to care in a timely manner is a high priority and substantial challenge for women, particularly for intravenous drug users who may face stigma and other additional barriers.
Keywords
Introduction
Eastern Europe/Central Asia is facing one of the fastest growing HIV epidemics in the world. 1 Ukraine has the second highest incidence of HIV compared to other nations in this region, with an estimated 36.9 newly-diagnosed HIV infections per 100,000 population per year. 1 The defining characteristics of Ukraine’s HIV epidemic are also changing. In its early stages, the Ukrainian epidemic was concentrated among injecting drug users (IDUs) and disproportionately affected men. 2 In 2008, heterosexual sex overtook drug use as the predominant mode of transmission and continues to be the main driver of the epidemic, accounting for an estimated 72.5% of new infections in 2015. 1 As a result, women have become an important, growing subset of people living with HIV in Ukraine. Among women over 25 years old, the number of reported infections due to heterosexual transmission more than doubled from 1814 in 2005 to 5057 in 2012. 2 In 2015 as many as 43% of all new infections were identified in women. 1 Ukraine also has the highest prevalence of HIV-positive pregnant women in Europe. 3 However, newly-diagnosed HIV infections in pregnant women have been declining, from 0.55% of all pregnant women tested for HIV in 2009 to 0.33% in 2015. 1
With Ukraine’s centralized health care system, patients may be tested for HIV at various service entry points, including maternal care services, tuberculosis (TB)/sexually transmitted infection (STI)/drug rehabilitation clinics, prison services, primary health care clinics, voluntary counseling and testing sites, or community outreach points. 4 HIV-positive individuals are then referred to a network of state-supported clinics that specialize in HIV care (called ‘AIDS centers’). Such AIDS centers are the only providers of HIV-related care in Ukraine. In order to access this treatment, patients must register at one of these centers. Registration requires additional confirmatory testing of HIV, which is conducted via Western blot offsite at a regional laboratory. Thus, a patient’s date of registration with the AIDS center is also the date of their initiation into HIV-related care following their diagnosis.
According to national protocols, initiation of antiretroviral therapy (ART) among non-pregnant women was recommended at a CD4 cell count of below 200 cells/mm3 during 2008–2009. 3 This was revised in 2010 to a threshold of <350 cells/mm3 or those with TB coinfection, and again in 2015 to include women with a CD4 cell count of <500 cells/mm3, those with coinfection of TB or hepatitis, or those believed to be at high risk of transmitting HIV to others. 5 ART has been recommended for all pregnant women, regardless of clinical indicators, throughout this time.
When ART supplies are limited (‘stock outs’), individuals with lower CD4 cell counts are prioritized for treatment. Due to the frequent separation of testing and treatment sites, the need to register for HIV care, and the lack of ability to receive treatment anonymously, patient care is often fragmented, patient data are often missing, and loss to follow-up is common.2,6,7 Approximately half of people living with HIV known to the Ukrainian health system are enrolled in care and treatment.4,7
Women disproportionately experience numerous risks for HIV infection and barriers to HIV testing and care. Women infected through heterosexual transmission may be vulnerable to domestic and social pressures, and not able to prevent HIV infection from their partners. 8 Furthermore, with a majority of people infected with HIV in Ukraine estimated to be undiagnosed, 9 women may be less able to prevent infection if they are unaware that their partners are infected. Women who inject drugs are at higher risk of HIV infection than their male counterparts, as they are more likely to be ‘second on the needle’, exchange sex for drugs, or be subject to gender-based violence.10,11 HIV-related stigma, economic barriers, and geographical and bureaucratic constraints also contribute to delays in diagnosis and treatment. 12 However, the unique demographics of and risk factors faced by the HIV-infected women in Ukraine remain poorly understood. In addition, Ukraine’s HIV epidemic tends to be concentrated in the eastern and southern regions of the country, 2 which has resulted in a dearth of research on HIV in Ukraine’s western regions.
The purpose of this study is to characterize the population of HIV-seropositive women who have registered for care in the regional AIDS center in Lviv Oblast in western Ukraine, to describe patterns in their clinical presentation, and to identify factors that influence delays between diagnosis and registration into care. Such detailed knowledge about the female face of Ukraine’s HIV epidemic will inform interventions to improve testing, prevention of future transmission, and linkage to care.
Methods
A retrospective chart review was conducted of all 622 HIV-seropositive women aged 18 years and older who registered at the Lviv AIDS Center, a governmental HIV/AIDS care center serving the Lviv oblast of Ukraine, between December 2008 and December 2013. Individual variables recorded from medical charts were age, city of residence, date of first blood draw for HIV testing, date of confirmation of first blood draw (when available), date of registration, transmission type, reason for testing, presence of AIDS (defined in Ukrainian clinical protocol by the Centers for Disease Control and Prevention 1993 revised classification system for HIV), 13 and presence of a broad range of symptomatic conditions (including HIV-related opportunistic infections such as TB, as well as HIV-unrelated symptoms such as STIs) at initial presentation.
Of note, ‘transmission type’ was determined by the registering health care provider based on a patient’s known risk factors and on the provider’s clinical judgment. ‘Reason for testing’ was provided by the patients themselves. Most women had a date on record for their ‘first blood draw’ or their ‘confirmation of first blood draw,’ but rarely both. The first blood draw (part of the initial HIV testing) and the confirmatory HIV testing are generally conducted at different locations. Delays in care were calculated as the time from either first blood draw or confirmation of first blood draw to the date of registration. These data were stratified by transmission type as well as reason for testing. Statistical differences were assessed using Chi square analyses and Kruskal–Wallis testing to compare patterns between tested variables. Data were analyzed with Stata v.11.2.
Informed consent was waived due to the retrospective nature of the study; however, names were not recorded and the database was stored securely for the duration of the study. This protocol was reviewed by the Institutional Review Board at Brown University.
Results
Demographics and HIV risk profile of women infected sexually versus through injection drug use (n = 615).
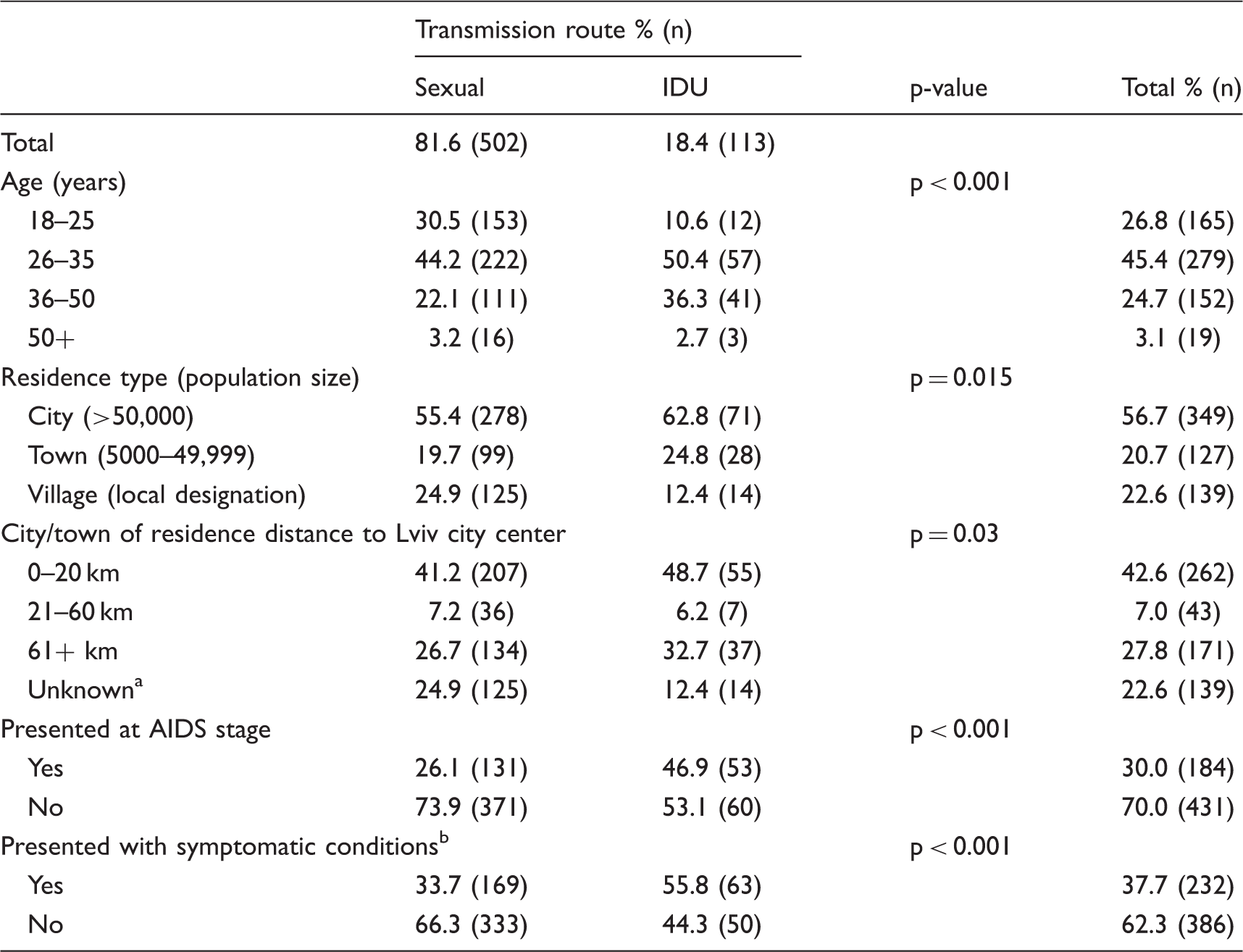
IDU: injecting drug user.
‘Unknown’ includes women living in villages whose geographic location was undocumented.
Includes HIV-related opportunistic infections such as tuberculosis, as well as HIV-unrelated symptoms such as sexually transmitted infections.
Women often presented to the HIV clinic for care with advanced HIV disease. One-third (30.0%; 184/615) of all women presented with AIDS as defined by the Ukrainian protocol. Of all women, 37.7% (232/615) presented with symptomatic conditions (which include opportunistic infection, STIs, or other AIDS-related conditions, that may or may not have met clinical criteria for AIDS). Although only 18% of women testing positive for HIV were infected through IDU, these women were overrepresented among those who presented with AIDS (46.9%; 53/113), compared to 26.1% (131/502) of those with AIDS who presented with heterosexual transmission. Among women whose stated reason for their original HIV blood test was IDU, 46.2% (24/52) presented for treatment with AIDS, and over half (55.8%; 29/52) presented with other symptomatic conditions. Among women tested during pregnancy, 8.8% (25/284; p < 0.001) presented with AIDS, and 16.6% (47/284; p < 0.001) had infectious symptoms.
Reasons for being tested for HIV and the median delay, in days, from diagnosis to registration at Lviv AIDS Center (n = 549).
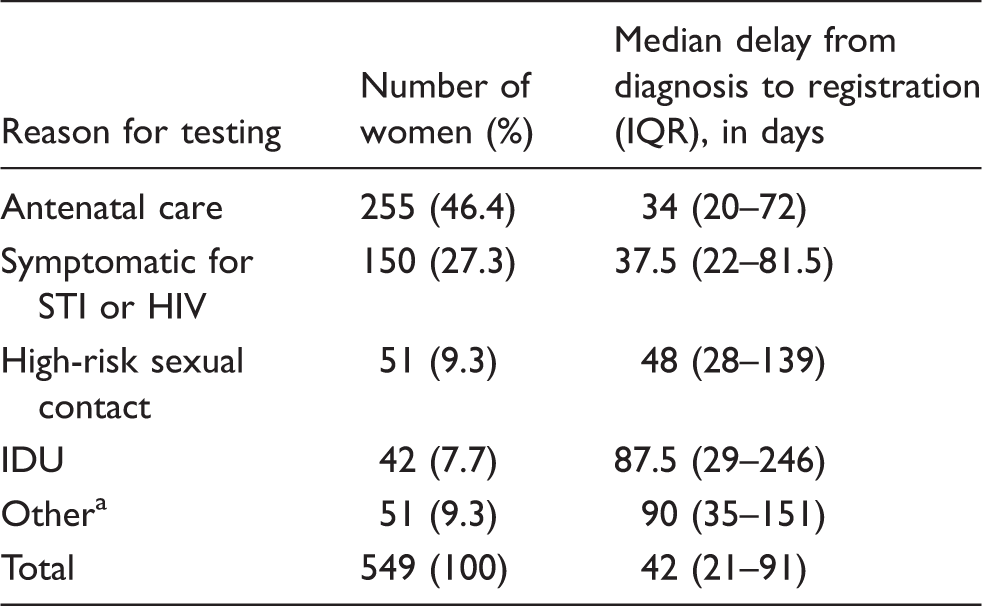
IDU: injecting drug user; IQR: interquartile range; STI: sexually transmitted infection.
Other includes first-time blood donors, prisoners or persons living in detention, tested anonymously, tested by their own will.
The median delay between diagnosis and registration in care across all patients included in this review was 42 days. Kruskal–Wallis tests showed statistically significant differences in times from diagnosis to registration; women tested during antenatal care had the shortest delay (34 days), those tested after high-risk sexual contact (48 days), and those with IDU as their reason for testing having the longest delay (87 days; p < 0.0001). Women who gave IDU as their reason for testing also experienced the greatest variance in the length of delay (IQR 29–246 days; see Table 2), which was significantly greater to those categorized with heterosexual transmission and those with IDU transmission (p = 0.002). Of those women categorized with IDU transmission, 18.5% presented for registration more than 360 days after their initial diagnosis. In contrast, only 7% of women categorized with heterosexual transmission presented with this same delay. While there does appear to be a downward trend in the length of delay between diagnosis and registration between 2011 and 2013, none of the patterns discerned when looking at data year by year were determined to be statistically significant (p = 0.119). There was also no significantly different time delay to seek care for women who presented with symptomatic conditions compared to those without (p = 0.539).
Discussion
This study analyzed the demographics and risk profiles of HIV-infected women who presented to the Lviv AIDS Center for HIV-related care between December 2008 and December 2013. A large majority of women who presented for care were categorized as infected through heterosexual transmission, which mirrors the generalized epidemic across Ukraine. Though the age range of registered women was wide, women with heterosexual transmission tended to be younger than women with IDU transmission. Women frequently presented with infectious symptoms and other signs of advanced HIV disease. Most of these women lived outside of the city of Lviv, where the AIDS center is located.
Our finding that nearly one-third of women diagnosed at this AIDS clinic first presented with AIDS, and that more than one-third presented with other infectious symptomatic conditions, is alarming. Our data indicate substantial delays of entry into care – delays that are notably longer among women with reported histories of IDU. Although western Ukraine carries a smaller HIV burden than many areas to the east and south of the country, 2 true HIV morbidity and mortality may be underestimated in this region as a result of the very late stages of HIV disease with which women are presenting.
Our study also suggests IDU women experience even more substantial delays in care than their non-IDU counterparts. This finding seems to contradict a recent study conducted in the Odessa region of Ukraine, which found that lower educational attainment, not feeling ill, and not having time to go to the AIDS center were significantly associated with delayed enrollment in HIV medical care, but that IDU status was not. 14 In interpreting these results, it is important to consider that the Lviv region of Ukraine has a lower HIV and IDU burden than does the Odessa region. 2 Additionally, IDU women in our study who presented both late to care and late in the course of their disease may have been influenced by factors such as education levels and not feeling ill, separately from their IDU status. The causes for such delays may also be due in part to the clinic’s accessibility; transportation may be a barrier in particular for women living far from the city and AIDS Center.
Fear of losing anonymity when registering with the government-sponsored AIDS Center is also a major barrier.15,16 The Ukraine Stigma Index studies suggest that stigma and discrimination toward people living with HIV has decreased between 2010 and 2014.15,16 However, generalized stigma remains high, and people living with HIV continue to experience discrimination in health care settings such as breaches of confidentiality and the refusal of medical care. Such experiences of discrimination are especially common among IDU patients, who are among the most socially vulnerable. 16 For these populations, the name-based registration system for HIV diagnosis and treatment may serve as a disincentive to seek care. 17
It is of particular note that of the women who gave IDU as their reason for HIV testing, more than one-tenth were designated by the clinician as HIV infected via heterosexual, and not IDU, transmission. This may be due in part to clinician efforts to protect patients from the social stigma associated with being labeled as IDU as well as to protect them from prosecution, as IDU remains criminalized in Ukraine. 18 Future studies should explore this discrepancy further.
Current research in Ukraine gives cause for optimism. Rapid HIV testing for key populations increased from 2009 to 2013 through support of The Global Fund grants. 7 A recent study has demonstrated that HIV-infected IDUs in Ukraine can be successfully linked and retained in HIV care through methadone maintenance treatment centers. 19 Harm reduction programs have successfully piloted outreach efforts by nurses to target IDU patients and offer HIV counseling. 20 Additionally, novel bottom-up approaches that allow service providers to develop HIV prevention programs show promise for generating new strategies for testing and treating women, especially those for whom current outreach efforts have been suboptimal. 21 However, if the World Health Organization’s 90–90–90 treatment goal 22 is to be met in western Ukraine, early detection of HIV must be improved, delays in entry into care must be reduced, and outreach efforts must be implemented and expanded to target at-risk, marginalized women, including IDUs and those living in rural regions.
Future work should explore effective linkage to care and treatment plans that promote patient engagement and adherence to care. As testing and treatment for HIV have often been separated, the targeted integration of these services may minimize delays in seeking care and improve patient retention and follow-up rates.7,14 A recent report from the Ukrainian Ministry of Health recognized that HIV-related medical care should be offered at places convenient for the patient. 5 While regional AIDS centers remain responsible for maintaining and reporting HIV and AIDS-related data, conducting HIV tests, and distributing ART, these centers now work with health care facilities of different specializations, such as TB and STI treatment clinics, to bring these services closer to patients. 1 Nearly all pregnant women in Ukraine receive HIV testing as part of routine antenatal care.1,23 This study found a 34-day median delay between diagnosis and registration into care among pregnant women; nonetheless, within the limited and critical time frame of a pregnancy, even this comparatively small delay may have implications for missed opportunities for preventing mother-to-child transmission, especially among women presenting late to antenatal care. However, in 2007, as many as 99% of Ukrainian women received at least one antenatal care visit. 24 Coverage with ART among women diagnosed with HIV in pregnancy increased from 9% in 1999 to 95% in 2015, 1 exemplifying the success of antenatal care programs. Although it is beyond the scope of this study, future research should investigate the proportion of registered women following up with ART postpartum. Additionally, future research should follow rates of initiation onto and adherence to ART among nonpregnant women, as well as delayed ART initiation and gaps in coverage.
Several limitations should be considered when interpreting these results. First, our study was conducted in the Lviv region of western Ukraine and may not be generalizable to the rest of the country. Our sample only included women who had already been diagnosed and successfully linked to care. These results may not be descriptive of the entire Ukrainian HIV epidemic or of those populations who were lost to follow-up entirely. Barriers such as mandatory inclusion on state registries of known HIV-positive persons may deter some segments of the population from care more than others. Some misclassification of modes of infection and diagnoses on medical records cannot be ruled out.
Conclusions
The HIV epidemic among women in western Ukraine is widely distributed, both geographically and across age groups, and nearly two-thirds of women present for care with AIDS or symptoms of infection. The HIV epidemic among women in western Ukraine should be a high priority for policymakers. Finding sustainable solutions to the challenges of timely diagnosis and linkage to care for women, especially women IDU, is critical for an effective response to the HIV epidemic in this region.
Footnotes
Acknowledgments
We would like to thank Oleksandra Grushynska for her help with translation, Dr Marta Vasylyev and the epidemiology office at the Lviv AIDS Center for their support of this project, and members of the Brown University Ukraine Collaboration.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Summer Assistantship Program at The Warren Alpert Medical School of Brown University.