
Abstract
There is a lack of evidence on the burden of Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG) and Trichomonas vaginalis (TV) among HIV-infected pregnant women in South Africa. We conducted a cross-sectional analysis of HIV-infected pregnant women in two healthcare facilities in a South African township to determine the prevalence of CT, NG and TV. HIV-infected pregnant women were recruited during the first antenatal care visit for their current pregnancy and requested to self-collect vulvovaginal swab specimens. Specimens were tested for CT, NG and TV using the Xpert® assay (Cepheid, Sunnyvale, CA). Of 247 tested for CT, NG and TV, 47.8% tested positive for at least one organism; CT = 36.8%, TV = 23.9%, NG = 6.9%. Forty three (17.4%) had multiple infections, of which 42 included CT as one of the infecting organisms. Of the 118 participants who tested positive for at least one sexually transmitted infection (STI), 23.7% reported STI-like symptoms. Among women who tested positive for CT, 29.7% reported symptoms while 47.1 and 27.1% of those who tested positive for NG and TV, respectively, reported symptoms. The high STI prevalence coupled with the low symptom prevalence among infected individuals justifies the use of diagnostic screening approaches rather than syndromic management of STIs in this setting.
Introduction
Chlamydia trachomatis (CT), Neisseria gonorrhoeae (NG) and Trichomonas vaginalis (TV) are major contributors to the global burden of disease. According to the most recent World Health Organization (WHO) estimates, more than 90 million new cases of these three infections were reported among adults aged between 15 and 49 years in Africa in 2008. 1 TV alone accounted for approximately 59.7 million of those cases, while CT and NG account for 8.3 and 21.1 million cases, respectively.
Numerous studies have shown that these sexually transmitted infections (STIs) significantly increase the risk for HIV transmission and acquisition. CT, NG and TV lead to inflammatory cytokine upregulation with subsequent accumulation of leukocytes – some of which are HIV target cells – in tissues around the genital tract as part of the immune response, which further increases the risk of HIV acquisition.2–4 The inflammatory response may be present even without apparent signs and symptoms. 5 Lesions that result from these STIs facilitate virus shedding, which increases the risk of genital HIV transmission to sexual partners during sexual intercourse.
During pregnancy, untreated STIs may lead to a variety of complications including intrauterine death (spontaneous abortion), preterm delivery, intrauterine growth retardation and low birth weight.6–8 Recently published evidence suggests that these STIs may increase the risk of mother-to-child transmission (MTCT) of HIV.9,10 Analysis of data from a multi-site study demonstrated that the rate of HIV MTCT was higher among infants born to mothers infected with CT (10.7%) or both CT and NG (14.3%) compared to those born to uninfected mothers (8.1%). 9 This finding was in line with a previous study conducted in Tanzania, which found that HIV-infected pregnant women with NG infection had 5.5 times increased risk of intrauterine transmission of HIV. 10
There is a lack of data on the prevalence of CT, NG and TV among pregnant women and their associated risk factors; especially in sub-Saharan Africa, which bears a disproportionate burden of HIV. The lack of epidemiological data impedes efforts to develop guidelines to effectively control these STIs. The few studies that have been published have reported infection rates among pregnant women, which are substantially higher than the general population.9–11
Despite compelling evidence from other regions supporting the establishment of universal diagnostic screening of CT, NG and TV in pregnancy with molecular tests, the majority of countries in Africa and other low-resource settings rely on the WHO-recommended syndromic approach in which treatment of STIs is based on the presence of defined signs and symptoms. 11 Given that most CT, NG and TV infections are asymptomatic, many infected women remain untreated. 12 Consequently, the syndromic approach is ineffective in controlling those infections or reducing associated adverse pregnancy outcomes. 13
We conducted a cross-sectional analysis of HIV-infected pregnant women accessing antenatal care (ANC) services at two primary healthcare (PHC) facilities in a South African township to determine the prevalence of CT, NG and TV. We also sought to determine the prevalence of symptoms among participants in order to inform recommendations relating to diagnosis and management of STIs during pregnancy.
Methods
Study design
This study was a cross-sectional analysis of women recruited as part of a study that sought to determine the acceptability and feasibility of using a point-of-care test for STI screening among HIV-infected pregnant women, conducted from 1 June 2016 to 31 October 2017. The current analysis included data from participants recruited up to 24 March 2017. The South African STI Treatment Guidelines recommend syndromic management of STIs in PHC facilities. 14 In this study, a point-of-care nucleic acid amplification test was incorporated into the basic ANC package offered to women at their first antenatal visit.
Study setting
The study was conducted at two PHC facilities in Tshwane District, South Africa; Tshwane incorporates Pretoria, the administrative capital of South Africa. Tshwane’s estimated general population HIV prevalence is 11.7% (95% CI: 8.1–16.6%). 15 Among pregnant women using ANC services in Tshwane, the estimated HIV prevalence is 23.4% (95% CI: 20.1–27.1%). 16 In 2014, early infant (six weeks) HIV positivity was estimated to be 1.85%. 17
Recruitment and data collection
The eligibility criteria for the main study were used in this analysis and included (1) women attending their first ANC session for their current pregnancy; (2) documented HIV-positive status; (3) gestational age less than 35 weeks; (4) age ≥18 years; (5) currently reside in Tshwane District, with intent to remain in Tshwane following delivery. Women were screened for eligibility by a research assistant. Gestational age was estimated via a gestational wheel using the last known menstruation date, with clinical confirmation via palpation and symphysis measurements by a study nurse. Eligible women providing consent were assigned a unique participant identification number (PIN).
Participants were interviewed by a research assistant using a structured questionnaire, which included socio-demographic characteristics and STI symptom screening questions. After being interviewed, a research nurse provided Basic Antenatal Care services as per South African Maternity Care Guidelines. 18 During this process, the research nurse collected clinical data including obstetric history, co-morbidities and HIV antiretroviral therapy. A physical vaginal examination was performed to assess for STI-defining signs and symptoms. The exterior of the vagina and vulva was inspected for any abnormalities or signs of infection including ulcers, lice, sores, scarring or warts, and for discharge (colour, odour, thickness and purulence). Where necessary, digits or a speculum was used in the vaginal orifice to inspect for any abnormalities, or for cervical position, effacement, thickness or pain.
Specimen collection and testing
Participants self-collected two vulvovaginal swab specimens using Xpert® CT/NG Vaginal/Endocervical Specimen Collection kits (Cepheid, Sunnyvale, CA) as per manufacturer instructions. Specimens were tested immediately and women were given results, and treatment if indicated, prior to leaving the facility. CT and NG were tested using the Xpert® CT/NG assay and TV was tested using the Xpert® TV assay (Cepheid, Sunnyvale, CA). Tests were conducted by clinic research staff. Participants were given targeted treatment on the basis of the Xpert® result if positive or treated syndromically if negative for all three organisms on Xpert®. As per South African STI guidelines Xpert®-positive participants were given partner notification/referral slips; these participants were also given the option to take a partner treatment packet with them for their sexual partner(s) for expedited treatment, which was not part of routine care. Participants were advised to return unused or leftover partner medication when visiting facilities for their STI test of cure.
Data management and analysis
Real-time data collection, using REDCap (Research Electronic Data Capture), was performed on tablet computers. 19 All captured data were stored in a secure, password-protected web-based server. Data quality checks were performed regularly, and inconsistencies were flagged for verification and correction. Barcoded PINs were placed on consent forms, copies of source documents, specimen collection containers and test cartridges to allow for direct linkage of participant data.
Prevalence was defined as the proportion of individuals who tested positive among individuals who were tested. Normality was assessed graphically and by the Shapiro-Wilk test; normally distributed variables were compared using Student's t-test, and non-normally distributed variables were analysed using Mann–Whitney U test. Categorical variables (proportions) were compared using the Chi square test (X2) or its non-parametric equivalent. Univariate and multivariate logistic regression were used to calculate odds ratios (OR) and their 95% confidence intervals (CI) to determine factors associated with being symptomatic among infected individuals. Multivariate logistic regression was conducted using the stepwise backward-elimination method (p-removal > 0.05). Variables significantly associated with being symptomatic at p < 0.25 in univariate logistic regression were included in the multivariate analysis. All data analyses were done in STATA v13 (StataCorp. 2013, College Station, Texas).
Ethical considerations
Permission to conduct the study was obtained from the management of our two study clinics and the Tshwane District Research Committee. Ethical clearance was obtained from the University of Pretoria, Faculty of Health Sciences, Research Ethics Committee (Ref: 401/2015) and the University of California Los Angeles (Ref: 15-001351). The ethics committees also gave permission for expedited partner therapy. Written informed consent was sought from all participants before they were enrolled into the study.
Results
Population characteristics
Socio-demographic characteristics of HIV-infected women tested for Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis in two healthcare facilities in Tshwane district, South Africa (n = 247).
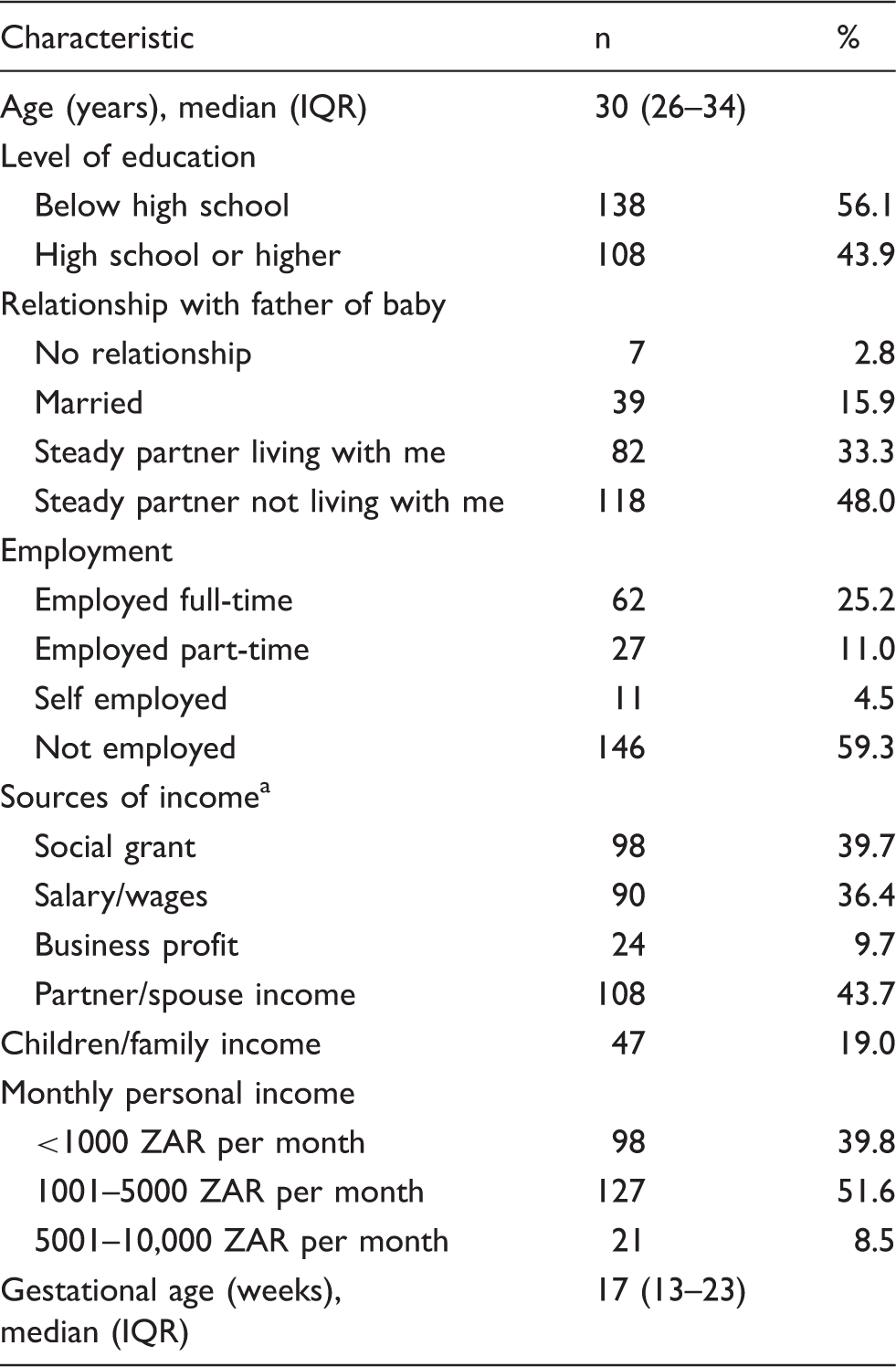
HIV: human immunodeficiency virus; IQR: interquartile range.
One participant had missing socio-demographic data.
Sources of income are not mutually exclusive
STI prevalence
Prevalence of Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis among 247 HIV-infected pregnant women in two healthcare facilities in Tshwane district, South Africa.
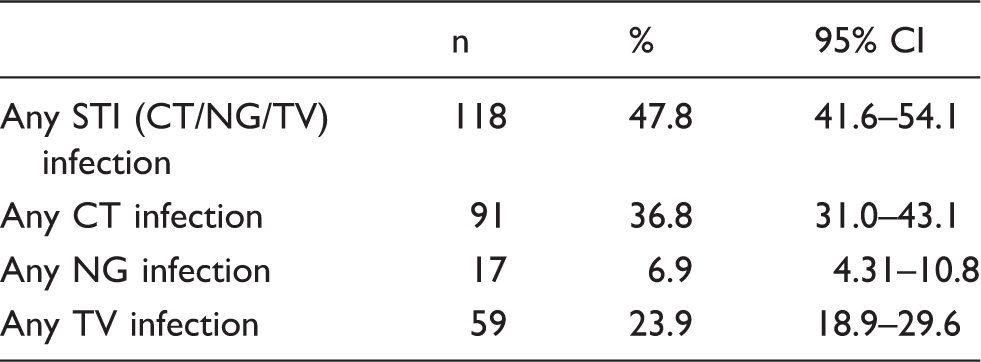
CI: confidence interval; CT: Chlamydia trachomatis; HIV: human immunodeficiency virus; NG: Neisseria gonorrhoeae; STI: sexually transmitted infection; TV: Trichomonas vaginalis.

Mono- and mixed-Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis infections among HIV-infected women with STI co-infections in Tshwane District, South Africa. HIV: human immunodeficiency virus; STI: sexually transmitted infection.
Prevalence varied by socio-demographic and clinical characteristics (Table 3). STI prevalence among pregnant women younger than 25 years (66.7%; 95% CI: 51.0–79.3%) was significantly higher than pregnant women aged 25–35 years (43.5%; 95% CI: 36.1–51.1%), but not significantly higher than pregnant women >35 years (45.9%; 95% CI: 30.6–62.2%). Overall prevalence was significantly higher among pregnant women who reported that they had a steady partner who did not live with them (55.9%; 95% CI: 46.8–64.7%) compared to those who reported that they were married (28.2%; 95% CI: 16.2–44.4%). There were no significant differences in prevalence by other demographic characteristics. There were also no significant differences in prevalence of STIs by clinical characteristics; however, it is notable that prevalence was highest among women attending their first ANC visit during their third trimester of pregnancy (57.1%; 95% CI: 35.4–75.6%), compared to women in earlier trimesters. Primigravidae also had the highest prevalence (58.6%; 95% CI: 39.9–75.1%), in comparison to multigravidae. Pregnant women with detectable HIV viral loads (>50 copies/ml) had a higher prevalence of STIs (54.8%; 95% CI: 42.2–66.9%), compared to those with undetectable viral loads (38.2%; 95% CI: 23.3–55.8%).
Prevalence of symptoms among STI-infected individuals
Prevalence of Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis by clinical and socio-demographic characteristics of HIV-infected pregnant women in two healthcare facilities in Tshwane district, South Africa.
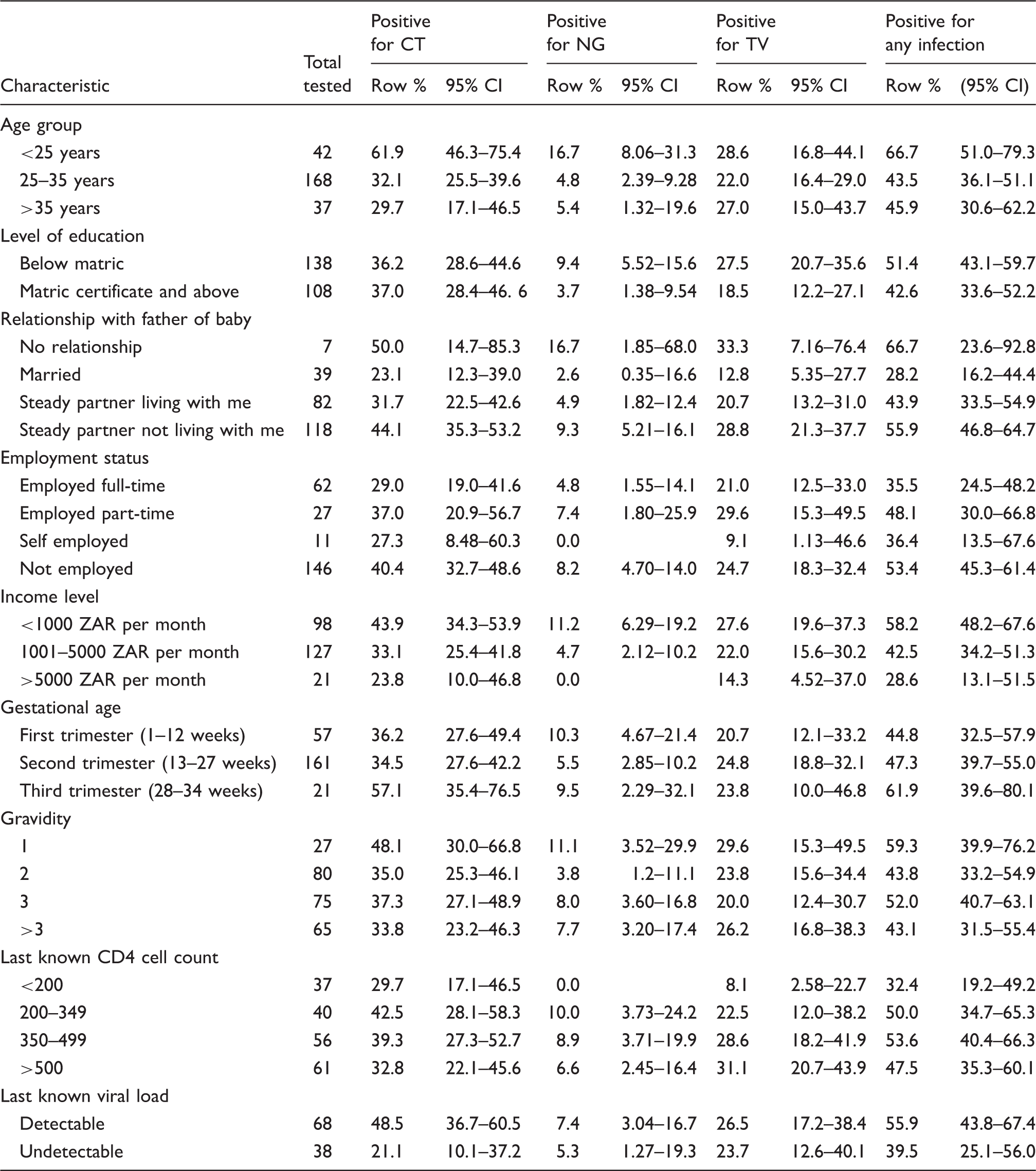
CI: confidence interval; CT: Chlamydia trachomatis; HIV: human immunodeficiency virus; NG: Neisseria gonorrhoeae; TV: Trichomonas vaginalis.
Prevalence of symptoms among HIV-infected women infected with Chlamydia trachomatis, Neisseria gonorrhoeae and Trichomonas vaginalis in two healthcare facilities in Tshwane district, South Africa.
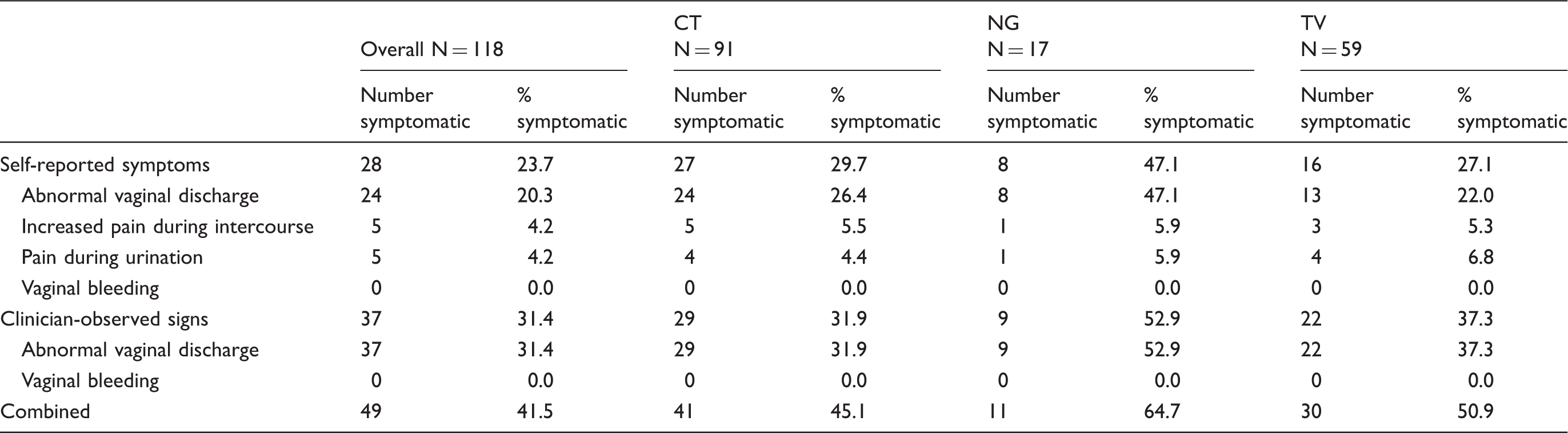
CT: Chlamydia trachomatis; HIV: human immunodeficiency virus; NG: Neisseria gonorrhoeae; TV: Trichomonas vaginalis.
Prevalence of symptoms by socio-demographic and clinical characteristics among HIV-infected pregnant women co-infected with Chlamydia trachomatis, Neisseria gonorrhoeae and/or Trichomonas vaginalis in two healthcare facilities in Tshwane District, South Africa.
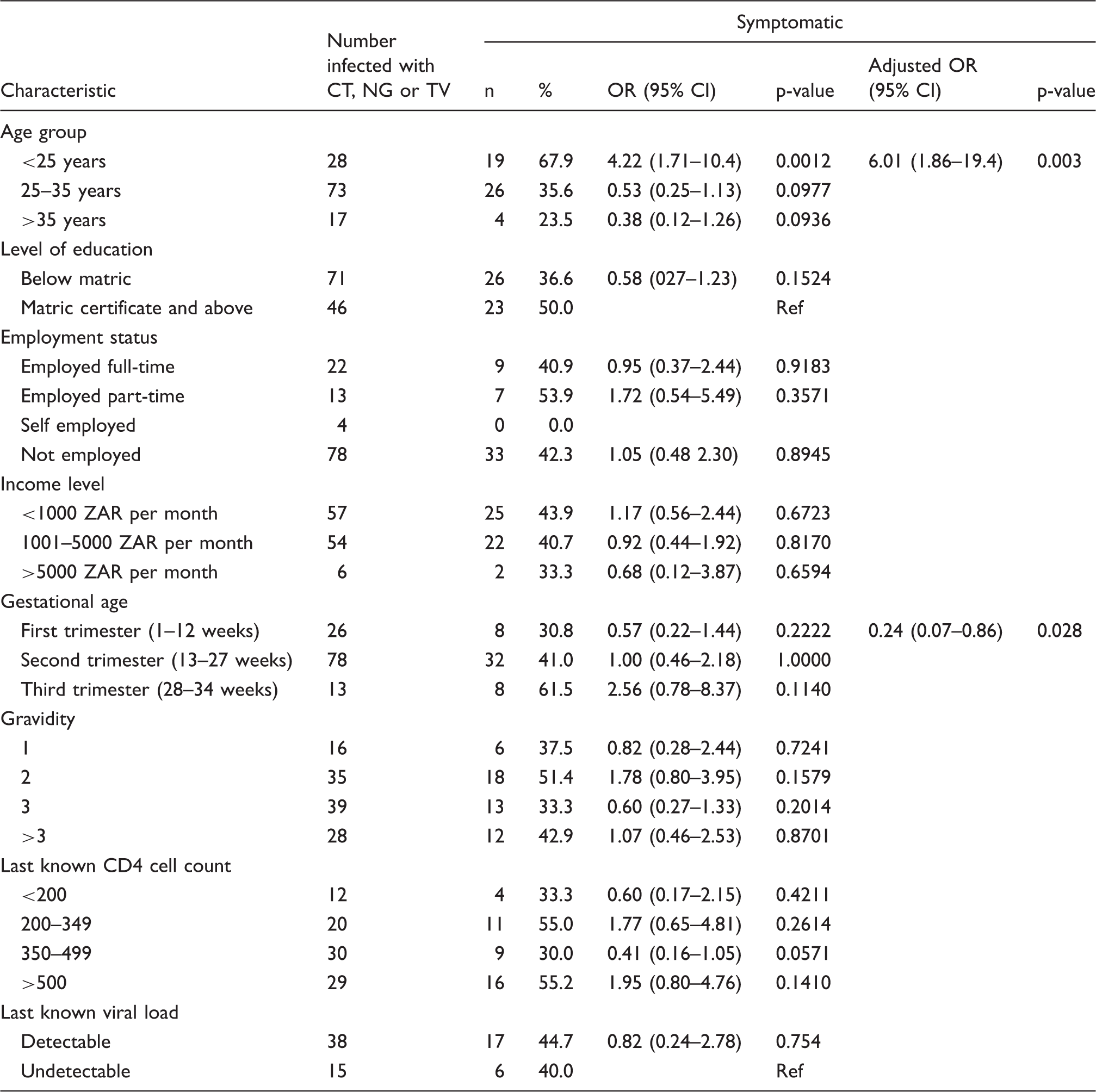
CI: confidence interval; CT: Chlamydia trachomatis; HIV: human immunodeficiency virus; NG: Neisseria gonorrhoeae; OR: odds ratio; TV: Trichomonas vaginalis.
Discussion
To the best of our knowledge, this is only the second study to use a point-of-care molecular diagnostic test to determine prevalence of CT, NG and TV among HIV-infected pregnant women in an African setting. Our study has documented high prevalence of three curable STIs in a population of HIV-infected pregnant women. Nearly 50% of HIV-positive pregnant women in our study sample tested positive for CT, NG and/or TV. The prevalence of CT in our study population is considerably higher than rates reported before among pregnant women in South Africa. In a systematic review that sought to summarise prevalence of curable STIs among pregnant women, Joseph Davey et al. 20 reported an adjusted mean prevalence of 4.4% (95% CI: 2.3–6.6%) for CT, 4.6% (95%CI: 4.0–5.2%) for NG and 24.6% (95% CI: 17.9–31.4%) for TV in the Southern African region. In a multi-site study, Adachi et al. 8 reported a CT prevalence of 21.3% among HIV-infected women in South Africa. Another study, conducted among women visiting a termination of pregnancy clinic, reported an aggregate prevalence of CT, NG and TV of 27%, with a CT-specific prevalence of 14%. 21 Another study, conducted in KwaZulu-Natal province, South Africa, reported CT prevalence of 17.8% (95% CI: 15.8–19.7%), NG prevalence of 6.4% (95% CI: 5.1–7.6%) and TV prevalence of 15.3% (95% CI: 13.5–17.2%) among pregnant women. 22
To our knowledge, our finding of a 36.8% (95% CI: 31–43.1%) prevalence of CT in pregnant women is the highest reported in pregnant women, globally. A possible reason for this higher prevalence is that our study sample consisted exclusively of HIV-infected women – who may be at higher risk of STIs. Unpublished data from our study sample show high levels of sexual risk behaviours including high levels of condomless sex at last sex and having multiple sexual partners in the past 12 months. 23 It should also be noted that the diagnostic assay used in our study is not identical to those used in other studies and there may be disparities in test sensitivity and specificity. Nonetheless, an investigation of drivers of STIs, particularly CT, in this setting is warranted.
Although several studies have shown that HIV-infected individuals are at higher risk of STIs than HIV-uninfected individuals, available evidence suggests CT prevalence does not vary by HIV status.3,4,24 Moodley et al. 22 found statistically significant differences in NG and TV prevalence between HIV-infected and HIV-uninfected pregnant women; however, they found no difference in CT prevalence by HIV status. Interestingly, Mafokwane and Samie 25 reported a CT prevalence difference between HIV-infected individuals taking ARVs and those not taking ARVs (28.5% versus 38.1%). In our study, prevalence of CT was higher among individuals with detectable viral loads compared to those with undetectable viral loads, but there seemed to be no relationship with CD4 cell count, which is a marker for immune status.
Over a third of women in our study with an STI were found to have multiple infections. The significance of multi-infections is mostly unknown; however, they complicate empirical treatment, which forms the basis of syndromic management of STIs.26,27 Prevalence of different combinations of organisms in those with multiple infections tends to vary by location, socio-demographic and clinical characteristics, and seems to be dependent on the prevalence of individual microorganisms.28–30 This highlights the need for targeted treatment based on diagnostic tests. Alternatively, granular context-specific prevalence estimates from sentinel laboratory surveillance activities can guide standardised or epidemiological treatment. Future studies need to investigate the impact of multiple infections on pregnancy outcomes in comparison with mono-infections.
Our finding that pregnant women younger than 25 years have higher STI prevalence compared to women older than 35 years confirms findings from several other studies that reported younger maternal age as a risk factor for STIs.31,32 There are a variety of biological, immunological and behavioural factors that contribute to this increased risk. The trend towards a higher prevalence of STIs among HIV-infected women presenting late for their first ANC consultation, although not statistically significant, is concerning. HIV-infected women who start attending ANC later in pregnancy will have less time to achieve viral suppression if they had not started antiretroviral therapy prior to this. Though viral load is the most important determinant of HIV vertical transmission, 33 STIs are known to increase vaginal shedding of HIV, thus increasing the risk of transmission from mother to child. 9 This highlights the need for early enrolment into ANC.
Consistent with findings from other studies, the majority of women in our study with STIs were asymptomatic.21,22 Self-reported symptoms only identified a quarter of women with STIs, while clinician-observed symptoms could only identify about a third. Though the sensitivity of symptom screening seemed enhanced when self-reported and clinician-observed symptoms were combined, less than half of women with STI infections would have been correctly identified using this combined screening method. These results must be interpreted with caution, as symptoms may be due to infections by micro-organisms that were never tested.
The high prevalence of STIs in HIV-infected pregnant women, and the low sensitivity of symptom screening in identifying those infected with STIs, suggests that universal testing of STIs using definitive diagnostic tests may be justified in this population. Cost–benefit analyses of implementation of these diagnostic tests need to be conducted, including studies to investigate optimal models of delivery. Given reported high rates of late presentation for ANC 17 and loss-to-follow up from care between the first ANC visit and delivery, 34 we believe that point-of-care implementation of these diagnostic platforms, followed by same-day treatment provision, would be beneficial. Finally, efforts must be made to identify drivers of STIs in the general population to aid the design of appropriate interventions.
Footnotes
Acknowledgements
The authors would like to acknowledge the Tshwane District Department of Health and clinic managers who gave permission to conduct the study at the respective sites and the facility staff who accommodated our study teams. We would also like to thank Collin Price and Erika Morikawa for their support in the study.
Authors’ contributions
AM-M and JDK conceived the study and are the primary grant holders. MM, RPP, LDV, DO, DJD and JAM contributed to the design of the study. LDV, DO and EM managed the implementation of the study and oversaw data collection. MM, EM, DJD and RPP conducted data analysis. MM drafted the manuscript. All authors assisted with interpretation of results, commented on draft versions and approved the final version of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: this research has been supported by the Eunice Kennedy Shriver Institute of Child Health and Human Development (NICHD) of the National Institutes of Health (NIH) under award number: R21HD084274-01A1 and the President’s Emergency Plan for AIDS Relief (PEPFAR) through the United States Agency for International Development under the terms of the Cooperative Agreement AID 674-A-12-00017.