
Abstract
Vaginoplasty by penile and scrotal skin inversion is a well-established technique for male-to-female gender confirmation surgery. In this setting, chronic inflammation and lacerations associated with history of human papillomavirus (HPV) infection may induce a high risk of malignant degeneration in the long term. A 78-year-old transgender woman was admitted with genital discomfort and neovaginal discharge. The patient’s history revealed male-to-female gender confirmation surgery with construction of a neovagina by penile and scrotal skin inversion at 33 years of age. Physical examination of the genitalia revealed presence of fecal material, suggestive of recto-neovaginal fistula. A biopsy specimen was positive for well-differentiated HPV-related squamous cell carcinoma. Magnetic resonance imaging (MRI) showed a bulky mass in the posterior wall of the neovagina that infiltrated the urethra, prostatic gland and the anterior rectal wall. Following a multidisciplinary evaluation, we performed a definitive sigmoid colostomy and administered chemotherapy. Long-term follow-up seems advisable in patients after vaginoplasty due to the possibility of delayed development of cancer. Following biopsy, we consider MRI as the modality of choice to identify possible infiltration of the adjacent structures. As data regarding these lesions are scarce and management is complex, a multidisciplinary approach is recommended.
Keywords
Introduction
The number of patients seeking gender confirmation surgery has increased in recent years and several surgical approaches have been described. 1 Vaginoplasty by penile and scrotal skin inversion is a well-established technique for male-to-female gender confirmation surgery. 1 Possible complications include recto-vaginal or urinary fistula, prostate or nerve damage during the dissection, hemorrhage, infection and urethral stricture. 2 Chronic inflammation and lacerations, such as fistulae or burn scars and heterotopic glans and prepuce with a history of human papillomavirus (HPV) infection, increase the risk of long-term malignant degeneration. 3 However, data documenting the risk are lacking due to the small population of patients who undergo this surgery.
We describe a case of HPV-related squamous cell carcinoma in a patient with neovagina after surgical male-to-female gender confirmation surgery.
Case report
A 78-year-old transgender woman was admitted in our centre with genital discomfort and neovaginal discharge. Symptomatology began about two years earlier with a small ulcer on the labia majora that progressively extended posteriorly. Her history was notable for diabetes mellitus, acute myocardial infarction treated by coronary stent placement, cholecystectomy and male-to-female gender confirmation surgery with construction of a neovagina by penile and scrotal skin inversion at 33 years of age. The patient described having several sexual partners in the 45 years since surgery, but she did not have any routine gynecological examinations during this time.
Physical examination of the genital region revealed hyperkeratotic, vascularized and friable neovaginal tissue, and the presence of fecal material, suggestive of a recto-neovaginal fistula (Figure 1). Rectal exploration clearly showed a recto-neovaginal fistula and an ulcerated induration in the recto-neovaginal septum.

Physical examination. Hyperkeratotic and hypervascularization of the neovulva were observed.
A biopsy specimen obtained from the hyperkeratotic vulvar region showed well-differentiated squamous cell carcinoma. HPV-16 infection was confirmed by polymerase chain reaction (PCR). Magnetic resonance imaging (MRI) showed a bulky mass in the posterior wall of the neovagina that infiltrated the urethra, the entire prostatic gland and the anterior rectal wall for 4 cm up to the internal sphincter. No significant large volume loco-regional lymph nodes or pathological inguinal lymph nodes were identified (iT4N0) (Figure 2).
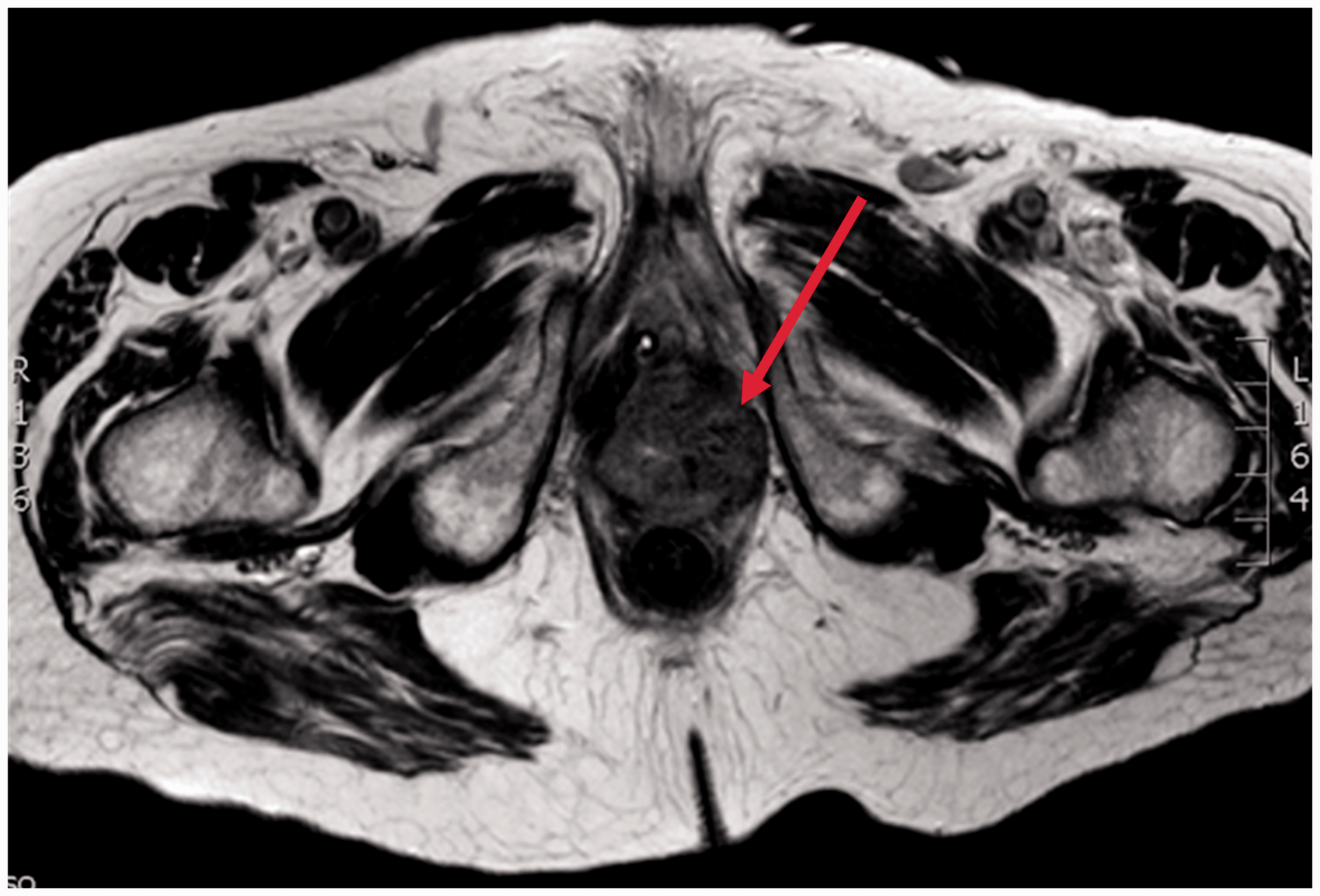
Magnetic resonance imaging showing a bulky mass in the posterior wall of the neovagina.
The patient was evaluated by a multidisciplinary team including a general surgeon, a plastic surgeon, an oncologist and a gynaecologist. The wide tumour extension was considered, and a definitive sigmoid colostomy was performed to improve the local condition and relieve the symptoms. Radiotherapy was not performed due to the presence of local sepsis and inflammation, and an active fistula, but chemotherapy with carboplatin and 5-fluorouracil was administered with the aim to reduce the tumour mass. Despite the antibiotic therapy and the suspension of the chemotherapy, to avoid iatrogenic immunosuppression, the patient died two months later due to sepsis, caused by Pseudomonas aeruginosa and Klebsiella pneumoniae, that resulted in multi-organ failure.
Discussion
Tissues such as the bladder, amnion, dura and bowel may be used to create a blind pouch for neovagina reconstruction following various surgical techniques. 4 Sigmoid colon grafts offer several advantages, such as greater lubrication and injury resistance and a lower risk of stricture. 1 However, vaginoplasty using penile and scrotal skin inversion also has advantages such as the incorporation of sweat glands and hair follicle loss, thus achieving normal anatomical and physiological vaginal characteristics such as pH and microbiological flora. 5 The postoperative complications of this approach include chronic laceration, abscesses, neovaginal and urethral stenosis and recto-neovaginal fistulae. 2 A risk to develop condylomata and HPV-related intraepithelial and invasive squamous carcinoma or adenocarcinoma in the neovagina has been reported with both penile and scrotal skin inversion and sigmoid colon grafts.5–7 A direct relationship between HPV type 16 and 18 infection and penile squamous cell carcinoma has been described previously and was also confirmed in the present case. 8 Neoplasia originates from the original donor tissue. 9 In the case of squamous cell carcinomas, as in the case report presented here, the tumour derives from the scrotal skin graft, while in the case of vaginal reconstruction with intestinal tissue, an intestinal adenocarcinoma may appear. 9
To the best of our knowledge, only one case of HPV-related squamous cell carcinoma of the neovagina after male-to-female gender confirmation surgery has been reported previously. 3 Fernandes et al. 10 reported a case of squamous cell carcinoma of neovagina, but the diagnosis of HPV infection was not confirmed. Cancer development was greatly delayed in the present case (45 years after surgery) as in the two previously reported cases (18 and 21 years later, respectively).3,10
Data regarding neovaginal carcinoma after reconstruction for vaginal agenesis are lacking in the literature, and it is difficult to make comparisons. The incidence of carcinoma is low (0.28%), 11 and the observation of HPV-related neovaginal lesions is earlier in the case of reconstruction for agenesis (median: 8 years). 5
In our opinion, following a biopsy, MRI is the recommended staging tool to detect the infiltration of the adjacent structures (urethra, prostatic gland and rectal wall), and, during the follow-up, routine gynaecological examination is advisable. A long-term follow-up is required due to the delayed cancer observation (mean: 28 years). Therefore, despite the scarcity of scientific evidence, the possibility of HPV-related squamous cell carcinoma must be considered in the differential diagnosis of lesion or ulceration in the neovagina created with penile and scrotal skin. As the treatment of choice for these lesions has not yet been defined, we consider a multidisciplinary approach to be mandatory.
Footnotes
Authors' contribution
Jesús Bollo, Andrea Balla, Carlos Rodriguez Luppi, Carmen Martinez, Silvia Quaresima, Eduard M. Targarona: Made a substantial contribution to the concept and design, acquisition of data or analysis and interpretation of data. Jesús Bollo, Andrea Balla, Carlos Rodriguez Luppi, Carmen Martinez, Silvia Quaresima, Eduard M. Targarona: Drafted the article or revised it critically for important intellectual content. Jesús Bollo, Andrea Balla, Carlos Rodriguez Luppi, Carmen Martinez, Silvia Quaresima, Eduard M. Targarona: Approved the version to be published.
Ethical approval
The approval of the Institutional Review Board of the Hospital de la Santa Creu I Sant Pau was obtained.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.