
Abstract
Chlamydia trachomatis (CT), an obligate intracellular bacterium, requires living cells to replicate. Half of men infected with CT are asymptomatic. CT infection can persist for up to four years within couples and affect their fertility. Chlamydia infection in men acts as a reservoir for transmission to women and can cause urinary tract inflammation, sperm DNA damage, and acute epididymitis. Semen samples from 1080 subfertile patients with normal and abnormal spermograms were examined to detect the presence of CT. An ELISA test was used to detect the presence of anti-CT IgA in these patients’ seminal plasma. CT infection was also confirmed by molecular investigation using specific primers. In order to evaluate the effect of CT infections on the DNA Fragmentation Index (DFI), 40 CT-infected cases and 20 CT-negative controls were analyzed by a Sperm Chromatin Structure Assay using flow cytometry. Among 1080 patients with poor sperm parameters, 155 (14.3%) patients were diagnosed with CT, 11% among those with semen abnormalities and 26% among those without semen abnormalities patients. The DFI was statistically higher in cases than in controls (p < 0.05). Given the prevalence of infection and also the high frequency of asymptomatic CT infection among infertile individuals with poor sperm parameters, screening for infection in these patients is essential in order to avoid adverse sequelae. We propose that the higher rate of DFI in CT-infected infertile men might be an underlying cause of their infertility and this warrants greater attention.
Introduction
Chlamydia trachomatis (CT) is one of the most prevalent sexually transmitted infections in the world and a common cause of pathology in both men and women, causing urethritis, epididymitis, prostatitis, cervicitis, pelvic inflammatory disease, ectopic pregnancy, and tubal factor infertility.1,2 While there are regional differences in prevalence, it remains a common cause of genitourinary pathology in men and women. However, its role in male fertility and also in sperm function, sperm DNA damage, pregnancy rates, and live birth rates is not clear.
CT attachment to human sperm has been demonstrated by transmission electron microscopy and immunofluorescence with monoclonal antibodies to the bacteria. Sperm penetration tests also showed that sperm can carry chlamydia that is connected to itself. 3 Elementary bodies (EBs) and reticulate bodies (RBs) of CT have been observed by electron microscopy in spermatazoa. All stages of RB formation in the head of the spermatozoon were detected after the passage of the infectious EB into the nucleus. Therefore, it can be assumed that CT can infect men and be transmitted by sperm to the female partner, which can cause infertility. 4 Abnormal sperm motility has been seen in men with CT infection. 5 Meanwhile, the effect of CT on semen quality is debated. In vitro studies have shown that coincubation of sperm with Chlamydia can significantly reduce the motile sperm quantity and lead to premature sperm death. Overall, in vivo studies of CT in men have provided inconsistent evidence as to whether it is associated with reduced fecundity. 6
Although some authors have shown that CT infection is associated with poor semen quality,7,8 others have claimed that there is no relation between them; thus, some patients may still remain asymptomatic. For instance, antibodies to CT in semen are not associated with leucocytospermia. Leucocytospermia per se does not appear to be significant for sperm function and also any immune responses to sperm.9,10. As the etiology of approximately 55% of male factor infertility is unknown, it is possible that Chlamydia might contribute to some of these asymptomatic cases as well.
Several studies have been done on the prevalence of CT throughout the world. Some of the variability that has been observed in CT prevalence is likely due to variability of testing methods, which have different sensitivities and specificities. Diagnostic processes to detect CT infections include both direct and indirect methods. Generally, localized infections can be tested by assays for direct pathogen detection, like culture, antigen tests, nucleic acid hybridization, and amplification tests. Indirect techniques depend on detection of antibodies against CT and may be used for diagnostic evaluation of chronic or invasive infection and postinfectious complications. In these conditions, pathogens have crossed the epithelium and may no longer be detectable in mucosal specimens. Serology is inappropriate to diagnose acute infections of the lower genital and anal tract, as the antibody responses become detectable only after several weeks to months. 11 Historically, Chlamydia was grown in culture; however, this was replaced in many centers by antigen detection. The most commonly studied antibodies included those directed against CT IgG and CHSP60. Most individuals with urogenital chlamydial infection develop serum IgG and IgA antibodies, which persist for several years and have been considered a marker of past infection.12,13 Accordingly, serology finds application in the diagnostic work-up of suspected chronic CT infection but is inappropriate to diagnose acute infections.
One of the precise methods for detecting the infection is molecular evaluation of semen or urine. It is thought that the presence of chlamydia in semen may indicate an infection of the upper genital tract; however, this may also reflect a contaminated urethra, through which the ejaculate passes. Semen testing has been shown to detect isolated cases of chlamydial infection. The presence of CT in urethral samples and its absence in semen specimens may indicate an asymptomatic lower genital tract infection that may have less fertility-related relevance. 14
In the present study, we aimed to determine the prevalence of CT in semen samples of the male partners of infertile couples using serological and molecular investigations and to investigate whether CT could be associated with poor semen quality and sperm DNA damage.
Materials and methods
Subjects
According to the guidelines of the Ethics Committee of Royan Reproductive Biomedicine Research Center, the activity did not require institutional review board approval, because our research project involved use of existing information collected from human participants (e.g. secondary datasets, existing biological samples), and there were no identifiers linking individuals to the data/samples. Meanwhile, written consent had been obtained from all patients for the use of their semen specimens.
Semen samples of 1080 subfertile couples (men aged 26–55 years old) attending the Infertility Unit of the Royan Institute were investigated. They were divided into two initial groups on the basis of medical examination and semen analysis: (1) Patients with normal spermogram as the control group and (2) patients with abnormal spermogram as the case group. The case group samples were checked for the WBC count, sperm count and sperm parameters such as sperm motility and morphology. The individuals in the case group who were CT-positive and had an abnormal spermogram with high WBC (above 1000 per ml), low sperm count (less than 30 million per ml), reduced normal morphology (less than 4%), and low sperm motility (less than 50%), were designated as the symptomatic group. That part of control group which were CT-positive and had no particular semen abnormality were considered as the third group called the infected asymptomatic group. Patients with a history of any antibiotic consumption in the last two months, positive for HIV, HBS Ag and HCV Ab, varicocele, and azoospermia and history of epididymitis or epididymo-orchitis, were excluded from this study.
Following confirmation of CT infection in a patient, one course of antibiotics was prescribed. In order to determine the efficacy of this treatment, molecular testing for CT was repeated. In case of a positive result, antibiotic therapy was prescribed again. In case of infection clearance, patients underwent Assisted Reproductive Technique (ART) and the outcome of ART in every patient with CT infection was also followed up.
Semen collection and analysis
Semen samples were collected by masturbation after three days of abstinence. Sperm concentration, motility and morphology were assessed according to the World Health Organization guidelines 15 using a computer-assisted semen analyzer (MICROPTIC); at least 2 × 200 spermatozoa were analyzed from evaluating sperm morphology.
After semen analysis, within 1 h from the time of ejaculation, 100 µl of 60 raw semen samples (40 symptomatic CT-positive cases and 20 controls) were frozen in liquid nitrogen for subsequent Sperm Chromatin Structure Assay (SCSA) analysis. The remainder was centrifuged and then seminal plasma removed and transferred to sterile vials and stored at −20°C for serological testing. The pellet was resuspended in phosphate buffer saline (PBS) and stored at −70°C for molecular testing.
Serological testing for CT
The CT ELISA IgA (A1017, Vircell, Spain) is an indirect immunoenzyme assay to test IgA antibodies against CT in human serum. The ELISA method is based on the reaction of antibodies in the sample tested with the antigen adsorbed on the polystyrene surface. Seminal plasma was tested manually according to the manufacturer’s instructions. Briefly, 5 µl seminal plasma was diluted in 75 µl serum diluents and 25 µl sorbent and then was incubated with the CT antigens coated onto a 96-well plate in 37°C for 45 min. After washing (five times), 100 µl conjugate was added to the wells and incubated for 30 min at 37°C. After further washing, 100 µl substrate was added. The reaction was stopped by stopping solution and optical density was immediately read at 450 nm using ELISA reader STAT FAX 3200. The signal-to-cut-off indices were categorized as per the manufacturer’s instructions as negative, equivocal, and positive.
Molecular methods for detecting CT
DNA extraction from sperm samples was performed using the Qiagen kit (QIAamp DNA mini kit: 51306), and DNA quality was assessed by spectrophotometry (nanodrop2000-thermoscientific). Five microliters of extracted DNA was added to the master mix which consisted of 2.5 µl 10X PCR buffer, 25 mM of MgCl2, 10 mM dNTPs, 10 pM of each primer, 50 U of Taq polymerase, and distilled H2O to a total volume of 25 µl. Specific primers were designed based on Plasmid0001 and plasmid pL2b820007 for amplifying CT DNA that are shown in Table 1. Negative control was prepared by adding 5 µl distilled H2O to one tube containing 20 µl of master mix. The samples were placed into a programmable thermal cycler. The amplifications were run under the following program: initiation denaturation step 94°C (5 min), followed by 40 cycles including denaturation at 94°C (30 s), annealing at 59°C (30 s), and elongation at 72°C (30 s). At the end, the temperature was held at 72°C for 7 min. The PCR products were detected by band which met the appropriate molecular weight in 1.5% agarose gel stained with ethidium bromide (Figures 1 and 2).

Four PCR products of primer CT1 in symptomatic and asymptomatic patients. As shown in the figure patient 3 is not infected. Sample 4 is a positive control. A 100bp ladder is used. PCR: polymerase chain reaction.
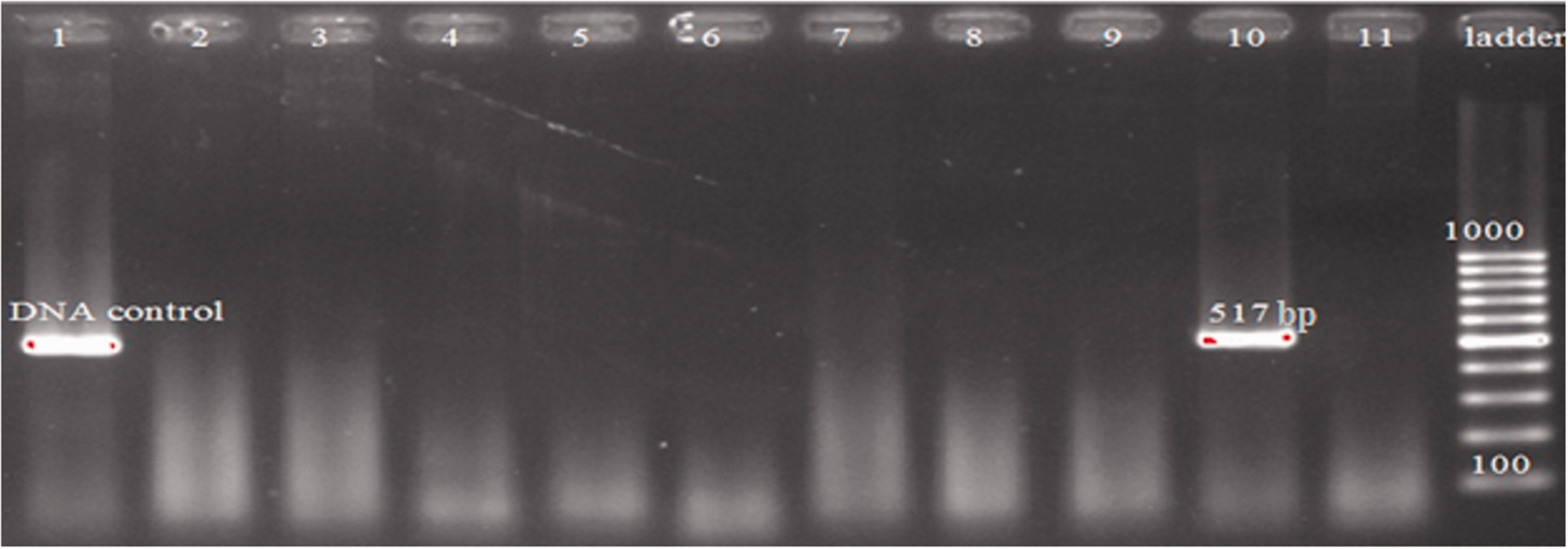
Eleven PCR products of primer CT2 in symptomatic and asymptomatic patients. As shown in the figure patient 10 is infected. Sample 1 is a positive control. A 100bp ladder is used. PCR: polymerase chain reaction.
Primers used in this study.

bp: base pair.
Purified DNA of CT (from Vircell, Spain) was used as a positive control for in vitro diagnosis based on nucleic acid amplification (AMPLIRUN® CHLAMYDIA TRACHOMATIS DNA CONTROL, Vircell, Grenada, Spain).
Any samples which were positive by molecular or serological testing were included as CT-positive samples.
SCSA for sperm DNA damage analysis
The procedure to measure sperm DNA damage by flow cytometry (SCSA) was performed as described by Evenson et al. 16 with a few modifications. Briefly, on the day of analysis, the samples were quickly thawed and analyzed immediately. The semen was washed and resuspended with PBS. This cell suspension was treated with an acid detergent solution (pH 1.2) containing 0.1% Triton X-100, 0.15 mol/l NaCl, and 0.08 N HCl for 40 s, and then stained with 6 mg/l purified Acridine Orange (AO) 17 in a phosphate–citrate buffer, pH 6.0.
Cells were analyzed using a FACSCalibur flow cytometer, equipped with an air-cooled argon ion (488 nm) laser (BD, San Jose). A total of 10,000 events were accumulated for each measurement at a flow rate of 200–300 cells/s. AO intercalated in double-stranded DNA emits green fluorescence, and emission is detected with a 530/30 band pass filter (Fl-1), whereas AO associated with single-stranded DNA emits red fluorescence and emission is detected with a 670 band pass filter (Fl-3). Data were collected and analyzed on the CellQuest program. The percentage of abnormal sperm with detectable DFI (%DFI) was calculated from the DFI frequency Dot plot obtained from the ratio between the red and total (red plus green) fluorescence intensity. 17
Statistical analysis
Data were presented as mean and 95% confidence interval. Statistical analysis was performed using SPSS version 20 (SPSS Inc. Chicago, IL). Quantitative outcomes (WBC and sperm parameters) were analyzed using one-way ANOVA while we computed accuracy indices (sensitivity, specificity, positive and negative predictive values) to compare ELISA findings and PCR (gold standard) results. Levene and Kolmogorov–Smirnov tests were applied to check homogeneity of variances and normality of the data as ANOVA assumptions, respectively. Post hoc test was performed using Tukey and Dunnett T3. Two-tailed P value < 0.05 was determined statistically significant.
Results
The mean age of the subfertile selected men was 36.1 ± 7.1 years. In this study, motility and morphology of sperm in all three groups (control, asymptomatic, and symptomatic) were significantly different (p < 0.05). While WBC and sperm concentration did not show significant differences between the control and asymptomatic groups (p > 0.05), these factors had shown significant differences between the control and symptomatic groups as well as between the symptomatic and asymptomatic groups (p < 0.05) (Table 2).
Statistical analysis results of spermogram parameters in the different groups.

CI: confidence interval.
aIndicates a significant difference between groups and control, p < 0.05.
bA significant difference between symptomatic and asymptomatic, p < 0.05.
The prevalence of CT infection in different groups of individuals in this study was different according to the detection method for CT. When CT was detected with serology tests, only 4.3% of the patients (47 people) were infected; 3% (27 patients) of them were symptomatic and 8% (20 cases) asymptomatic. Once all those with negative serology tests were reexamined by molecular methods, 18 CT infection was detected in 10% (108 people) of these samples; among them 8% (62 patients) were symptomatic and 18% (46 cases) were asymptomatic. Therefore, 14.3% of the patients were CT-infected (155 out of 1080 men) (Table 3). For more confidence all of the positive CT samples from the serology test were examined by the molecular method. ELISA sensitivity and specificity were 30.3 and 100%, respectively. The positive predictive value is 100%, negative is 89.9%, and kappa coefficient is 42.7. The molecular detection tests were also performed for the CT-negative group. Our serological test showed no false-negative results.
The prevalence of Chlamydia trachomatis infection detection by serological and molecular methods in CT-infected patients.

CT: Chlamydia trachomatis; ELISA: enzyme-linked immunosorbent assay; PCR: polymerase chain reaction.
The rest of the patients were excluded from the experiment due to lack of CT infection.
Moreover, there was a significant increase in sperm DFI of patients in comparison to controls (p < 0.05) (Figure 3).
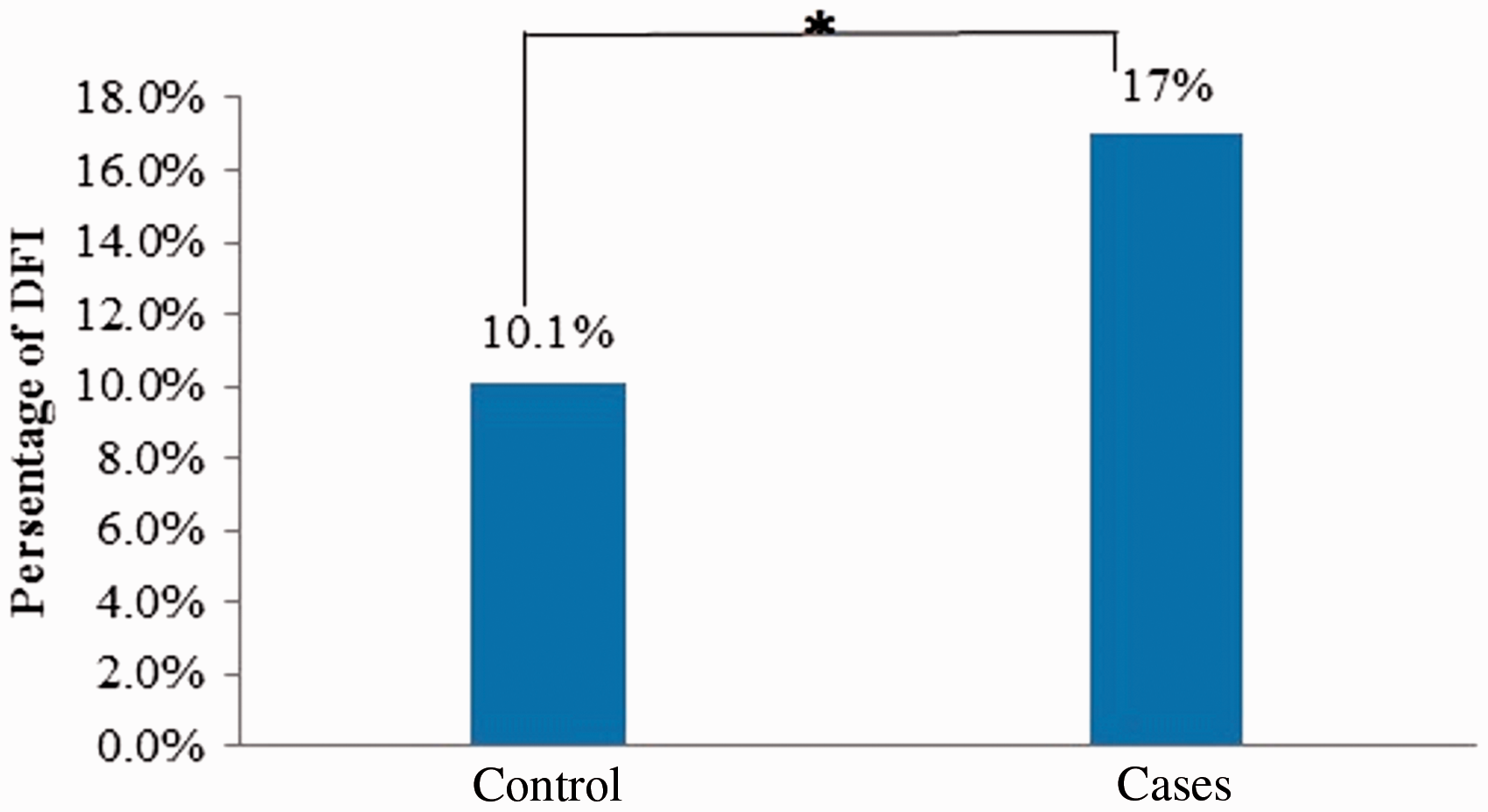
A significant increase in sperm DFI of cases compared to the control group. DFI: DNA fragmentation index.
After one year ART outcome follow-up of CT-positive patients in this project, only 50 (32%) CT-positive patients who were treated by proper doses of antibiotics entered ART cycles, in which 21 individuals (42%) had successful and 29 patients (58%) failed ART cycles. Among patients who had successful ART, 16 (76.2%) and five (23.8%) persons were symptomatic and asymptomatic, respectively. From patients with failed ART, 23 (79.3%) were symptomatic and the remaining six patients (20.7%) were asymptomatic. According to these data, there was no significant difference between the rate of ART success in asymptomatic and symptomatic individuals (p > 0.05).
Discussion
Studying CT infection in men is important, because it can be asymptomatic and act as a reservoir for infection in women. 19 This infection can persist up to four years within couples and affect their fecundity. 20 Although some cases of male infertility have known causes such as genital tract problems and hormonal disorders, many of them remain idiopathic and CT infection might be one of those reasons. 21
Vigil et al. 18 suggested that the possible effect of CT on male fertility may be mainly due to its transmission to female partners, which causes inflammatory processes and promotes the generation of antisperm antibodies. However Idahl et al. 22 showed that decrease in sperm motility and number of progressive spermatozoa, increase in the number of dead sperm, reduced sperm count, the prevalence of leukocytes in the semen, and increase in teratozoospermia index were significantly associated with the presence of IgM and IgG antibodies against CT in the sera of men in infertile couples. These findings were also observed by Veznik et al. 23 in the CT-infected group compared to CT-negative samples.
According to our results, it can be concluded that during the first steps of infection, the motility and morphology of the sperm are the first parameters which are impaired. In later stages and with infection progression, leukocytes can be detected in semen and semen density may also be decreased.
Gdoura et al. 24 reported that the average values of semen volume, sperm concentration, sperm count, sperm motility, sperm morphology, and the number of leukocytes were not associated with the detection of CT DNA in infertile men's semen samples. In contrast, our results showed that concentration, morphology, motility, and leukocytes were associated with CT infection. Similarly Mazzoli et al. 25 found that CT infection affects sperm morphology, concentration, and motility in prostatitis patients.
CT infection can be diagnosed by many different methods. As mentioned before, evaluating anti-chlamydial antibodies is not useful to diagnose epithelial infections of the lower genital tract, because detection of antibodies can be delayed for months, antibody titers may be low, and many serologic tests are not able to recognize antibodies against various chlamydial species. 11
The gold standard for CT detection in the UK is nucleic acid amplification tests (NAATs), which are remarkably more sensitive and specific than ELISA or CT culture. This method also allows for less invasive sampling. 26 Both the sensitivity and specificity of PCR were 100% when the ELISA results of these samples were decoded. Thus, PCR could be used for better diagnosis of C. trachomatis infection in comparison to the commercially available ELISA technique. 27 Although EIA is easy to perform, sensitivity levels can be low, varying between 62 and 97%. 14 The results of this study confirm this disparity.
In one study which was done in 2005 by Schillinger et al. 28 using NAATs, the prevalence of CT infection among DNA extracted from urine samples of 7% of men from four different states of America was reported. Also, Ghanaat et al. 29 in 2008, using urethral swab culture, showed that 9.3% of men with urethritis had CT infection. In the other study, Al-Sweih et al. 30 revealed that the prevalence of this infection among men with urethritis by CT NAAT was 12.4%. Rawre et al. 31 in 2016 screened urine samples for C. trachomatis by cryptic plasmid, ompA gene, and nested ompA gene PCR. Their study showed that 10% of men had CT infection. Nakashima et al. 32 also reported that C. trachomatis is detected more frequently in urine (15.9%) than oral samples (4.2%). Although, the results of these studies are virtually the same as of our findings (14.3%), it should be mentioned that the PCR method was used on different biological samples. In this study semen was used instead of urine for CT detection. However, in another study, the prevalence of CT infection in urine was done by Klovstad et al. 33 using BD ProbeTec Chlamydia Amplified DNA assay in Norway, only 5.1% of the men were diagnosed with CT infection. The CT positivity of 4.3% in urine from sexually active infertile young men with RT-PCR was also reported. 34 These two studies indicated lower level of infection of CT among European infertile men. The prevalence of CT in our study was higher compared to those reported in other studies – this could be due to more CT infection among men with poor sperm parameters. Also, as the present study was done on ejaculated semen samples, infection localised to the upper part of genitourinary system comes out with semen. Evidence about the effects of screening on CT transmission is of low quality because of directness and risk of bias. In a recent study, chlamydia reinfection was found in both general and high-risk populations. 35
Eley et al. 36 coincubated highly motile spermatozoa with extracting lipopolysaccharide from CT and an increase in the percentage of apoptotic spermatozoa from 5% in the control to 25% in the case group was revealed. The most important mechanism that CT can affect on both embryo quality and implantation rate, is DNA fragmentation. 37 So far little research has been done on the relationship between sperm DNA fragmentation index 38 and CT infection. One study in 2005 showed that normal sperm which were incubated for 6 or 24 h with CT had an increase in DFI compared with normal control sperm. 39 On the other hand, Gallegos et al. 40 reported that men who were infected with both CT and Mycoplasma had a 3.2 times higher DFI than the control group. Conversely a study in 2014 showed an increase in DFI in infertile men with CT infection; however, it wasn’t statistically significant. Rybar et al. 41 reported that the contamination of semen by CT, genital Ureaplasma, and Mycoplasma was not associated with sperm DFI. C. trachomatis infection can induce apoptosis in sperm. This effect may also illuminate the negative direct impact of C. trachomatis on sperm fertilizing ability. 42 Given the conflicting data, we sought to analyze the sperm DFI of patients infected by CT. In our study, we also found that DNA fragmentation was significantly higher in subfertile men infected with CT compared to the uninfected group. Our result is compatible with Satta's and Gallegos' findings. As the sperm DFI was compared in 20 symptomatic-infected patients and control fertile samples, we conclude that the correlations between the sperm DFI and the changes in the seminal parameters such as concentration, motility, morphology, and vitality in the infected samples could be attributable to the infection.
Accordingly, the relatively low result seen in ART outcomes for these patients might be due to incomplete repair of DNA damage and consequently, lack of sufficient recovery in the spermatogenesis process after CT infection, even though antibiotic treatment was prescribed.
Conclusions
If CT remains unchecked, infection will continue to pose a threat to reproductive life. Since asymptomatic cases are common in the population, regular screening should be encouraged in every unexplained infertile couple, particularly molecular analysis of semen samples. This study showed considerable prevalence of CT infection in infertile male patients, which necessitates screening and treatment for this infection. In comparison to ELISA methods, PCR-based methods have more sensitivity with equal specificity.
Footnotes
Acknowledgment
The authors would like to thank Dr Adrian Eley, University of Sheffield Medical School.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by Royan Institute Department of Genetics, Reproductive Biomedicine Research Center with Grant Number 90120700.