
Abstract
We report the first case of Nocardia beijingensis pericarditis in a 32-year-old HIV-infected patient. He presented with cardiac tamponade after failing to respond to treatment for smear-negative pulmonary and pericardial tuberculosis (TB). The pericardial fluid was examined several times before it eventually revealed filamentous branching organisms in Gram and modified acid-fast bacilli stain. The culture grew Nocardia spp. and was identified by 16s rRNA sequencing as N. beijingensis. Eight previously reported cases of Nocardia pericarditis in HIV-infected patients were caused by Nocardia asteroides. All patients had low CD4 cell count (range: 17–239 cells/mm3) and 50% of patients were treated for tuberculous pericarditis prior to making the correct diagnosis of Nocardia pericarditis. This report revisits the issue of nocardiosis as a great TB mimicker. It should always be considered in the differential diagnosis among HIV-infected patients suspected of having pericardial TB that is failing treatment.
Case report
A 32-year-old man was referred to our hospital with a sudden onset of chest pain and progressive dyspnea. He had been diagnosed with smear-negative pulmonary tuberculosis (TB) with pericarditis and human immunodeficiency virus (HIV) infection seven weeks prior, when he presented to the local hospital with fever and productive cough for two weeks. He also reported unintentional weight loss in the past three months. During this time, he had received dexamethasone, anti-tuberculous therapy, combination antiretroviral therapy (cART), and sulfamethoxazole/trimethoprim (SMX/TMP) for Pneumocystis jiroveci pneumonia (PJP) prophylaxis. On arrival, he had fever of 38.5°C, tachycardia (126/min), blood pressure of 97/71 mmHg, tachypnea and hypoxia. Physical examination revealed significant findings of prominent jugular venous distension, ill-defined point of maximum impulse and distant heart sounds. Clinical diagnosis of cardiac tamponade was made. Emergency pericardiocentesis was performed at the bedside and yielded 1 L of frank pus. Further evaluation with chest computed tomography demonstrated a large complicated pericardial effusion, pericardial enhancement with circumferential thickening, multifocal consolidations of both lungs with internal cavities, and centrilobular nodules with tree-in-bud appearance (Figure 1(a)). Two attempts of pericardial fluid examination including acid-fast bacilli (AFB) stain, Gram stain and culture were unrevealing. Sputum AFB and nucleic acid amplification tests for TB were negative. The follow-up echocardiogram three days later showed effusive constrictive pericarditis causing impaired diastolic function. Therefore, a second pericardial drainage was performed and 380 mL of pus was drained. Pericardial fluid Gram stain revealed numerous Gram-positive beaded filamentous branching organisms, which were also present using a modified AFB technique (Figures 1(b) and (c)). The diagnosis of disseminated nocardiosis was made. He received treatment with SMX/TMP and imipenem/cilastatin, and the anti-tuberculous therapy was discontinued. Pericardial effusion culture grew a Nocardia spp. DNA was isolated using QIAamp DNA Mini Kit (QIAGEN, Germantown, MD, USA). Further, 16S rRNA polymerase chain reaction and sequencing was performed using universal primers B27F and U1492R. The sequence showed 100% homology of 2074 base pairs with 96% identity to Nocardia beijingensis (GenBank® accession NR_118618.1) on BLAST searching of the NCBI database. Unfortunately, the patient suffered from re-accumulation of the pericardial effusion and underwent emergency pericardial window surgery, which yielded another 300 mL of anchovy-colored effusion. He developed septic shock with multiorgan system failure after the surgery. Septic work-up failed to recover an alternative causative organism. Despite aggressive treatment, he did not improve and he died after palliative measures were undertaken.
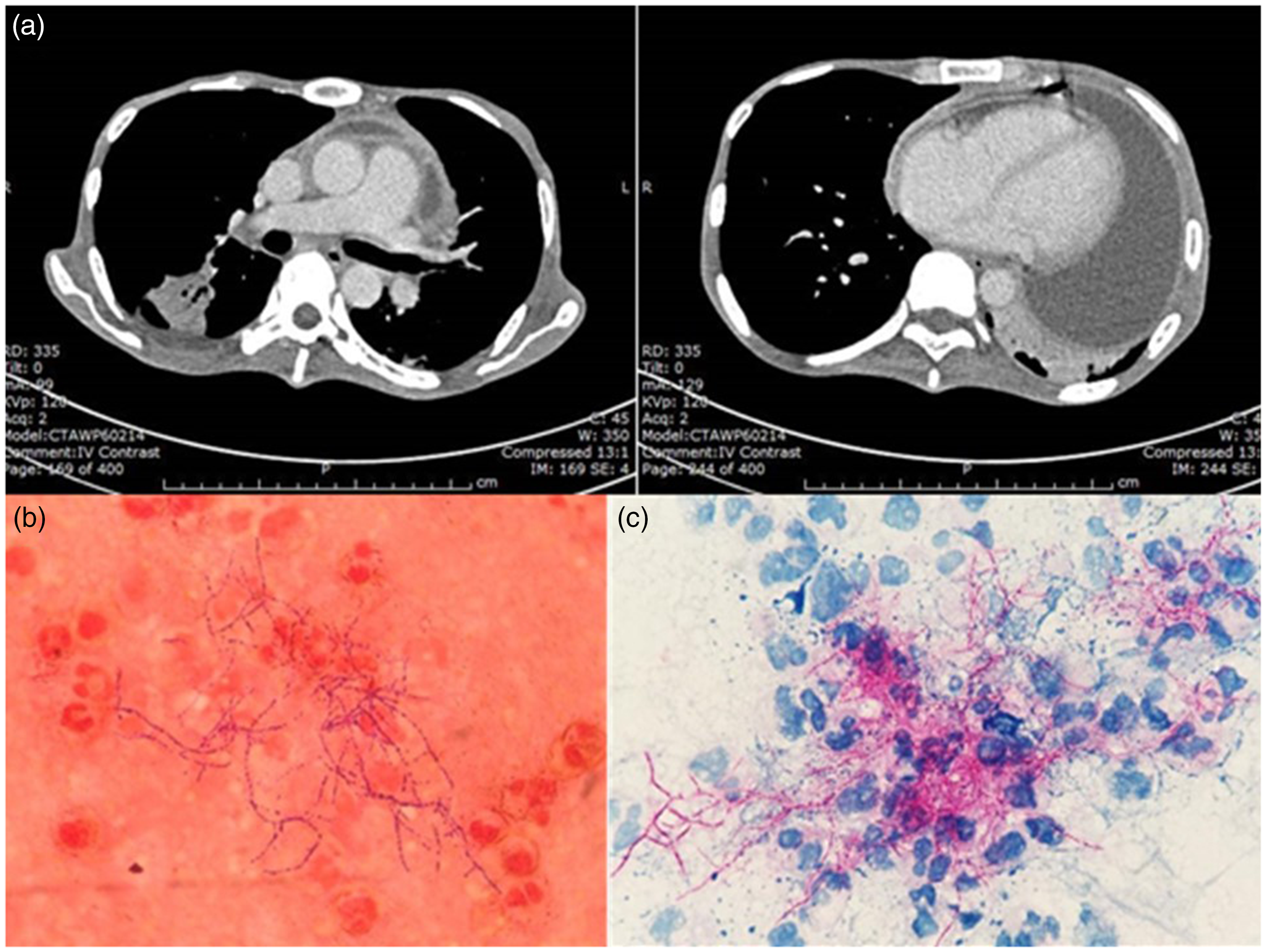
(a) Chest CT revealing large complicated pericardial effusion, pericardial enhancement with circumferential thickening, multifocal pulmonary consolidations with internal cavities, and centrilobular nodules with tree-in-bud appearance. (b) Gram stain of pericardial effusion showing Gram-positive beaded, filamentous branching organisms (original magnification 1000×). (c) mAFB stain of pericardial effusion showing positive red-stained branching filaments of Nocardia spp. (original magnification 1000×).
Discussion
Invasive Nocardia infection is usually observed among patients with malignancies, chronic pulmonary disease, on high-dose steroids, and hosts with defects in cell-mediated immunity, including HIV infection.1–3 The incidence of nocardiosis among HIV-infected patients is relatively low (0.2–1.8%), 4 especially compared to other opportunistic infections. This could potentially be explained by a protective effect from the wide use of SMX/TMP for PJP prophylaxis. 3
Since 1985, only nine cases of Nocardia pericarditis in HIV-infected patients have been reported in the literature, all of whom were cART naïve and had low CD4 cell counts (range: 17–239 cells/mm3), including our patient (Table 1). The presentation is usually subacute to chronic and 55% eventually developed cardiac tamponade,4–7 which is difficult to distinguish from TB infection. Eight cases (89%) presented with pulmonary infection that represented contiguous spread, but one case did not have strong evidence of active pulmonary infection which led us to speculate that Nocardia pericarditis could have been caused by distant dissemination. 7 All of them had at least one large-volume pericardial fluid drainage. The diagnosis was delayed in four cases. One reported laboratory misidentification of Nocardia with TB. 8 The other three were treated for presumptive TB infection and required several attempts before Nocardia was recovered from clinical specimens.5,6 Although pulmonary TB and Nocardia co-infection in HIV-infected patients are not unheard of, 9 only one case had proven evidence of both tuberculous and Nocardia pericarditis. 10 Overall, the treatment of Nocardia pericarditis by drainage combined with systemic antibiotics was successful (78%). SMX/TMP was commonly used as a part of the antibiotic regimen, except for one case that reported the effective use of ceftriaxone combined with minocycline in a SMX/TMP-allergic patient. 11 Our patient did not have a favorable outcome, which was possibly related to his severely immunocompromised state and prolonged course of illness before the precise diagnosis was made.
Previous case reports of Nocardia pericarditis in HIV-infected patients.
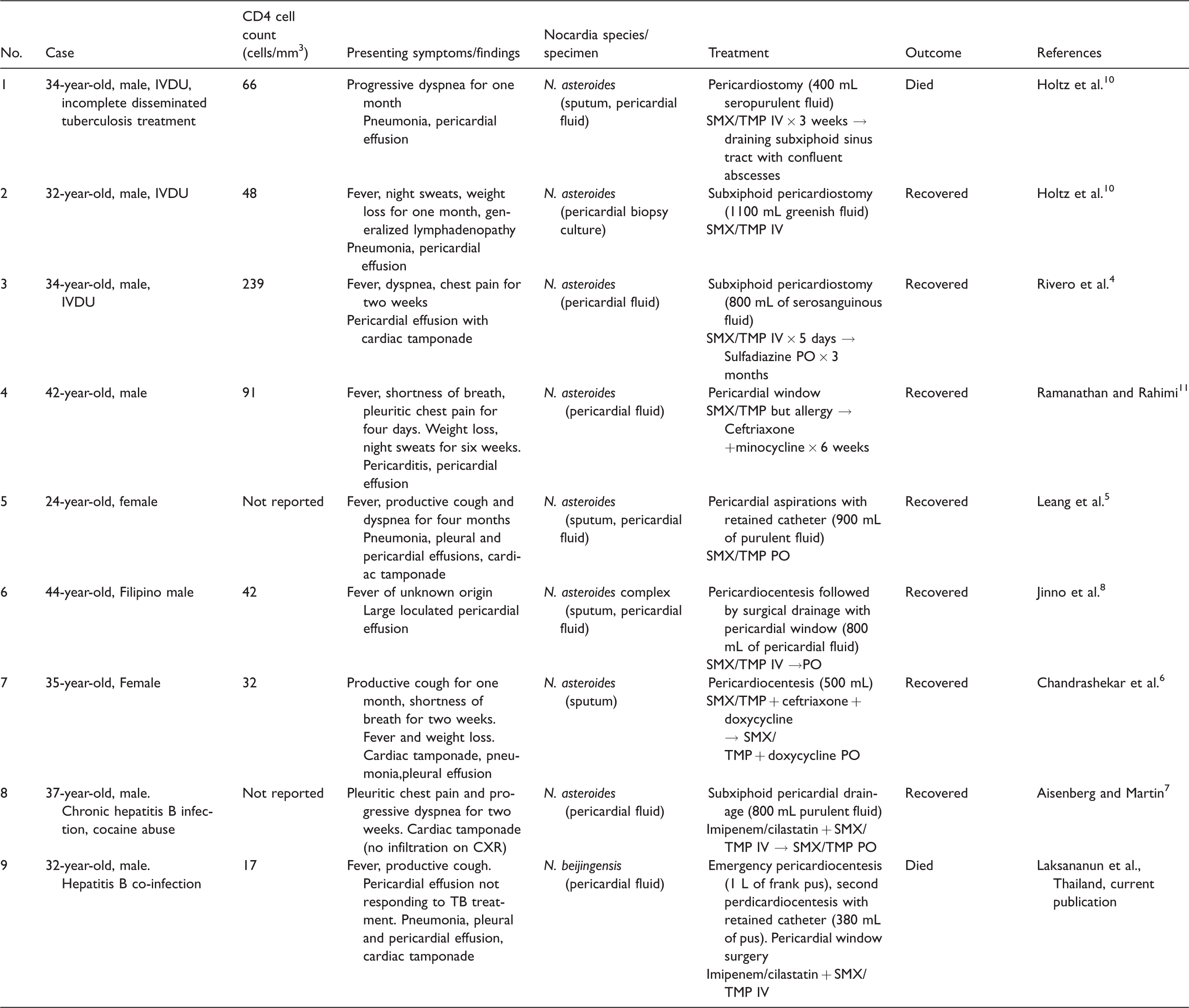
IVDU: intravenous drug user; SMX/TMP: sulfamethoxazole/trimethoprim; IV: intravenous; PO: per oral; TB: tuberculosis.
To our knowledge, this is the first case report of N. beijingensis pericarditis. All other previous Nocardia pericarditis reports were caused by Nocardia asteroides, the most common species causing invasive nocardiosis worldwide. 1 N. beijingensis was first isolated from Beijing, China in 2001, and it has been found to be quite prevalent among clinical isolates in Asia, including Thailand. 12 This report reemphasizes that nocardiosis is a great TB mimicker, although sometimes co-infection is possible. 10 Nocardiosis should always be considered in the differential diagnosis in HIV-infected patients suspected of having pericardial TB infection, especially when it is difficult to recover the pathogen or the patients do not respond to anti-tuberculous therapy. This suspicion should prompt repetitive examinations of clinical specimens to increase the chance of pathogen discovery. Newer techniques, such as 16s rRNA gene sequencing, are useful to expedite the identification and speciation of causative pathogens in the modern medicine era.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.