
Abstract
Adolescents in Africa are at high risk for HIV infection, other sexually transmitted infections (STIs) and bacterial vaginosis (BV). Since behavior and burden of STIs/BV may influence HIV risk, behavioral risk factors and prevalence of STIs/BV were compared in HIV-seronegative adolescent females (n = 298; 16–22 years) from two South African communities (Soweto and Cape Town). STIs (Chlamydia trachomatis, Neisseria gonorrhoeae, Trichomonas vaginalis, Mycoplasma genitalium, herpes simplex virus (HSV)-1, HSV-2, Treponema pallidum, and Haemophilus ducreyi) were detected by multiplex polymerase chain reaction, human papillomavirus (HPV) by Roche Linear Array, and BV by Nugent scoring. Rates of BV (Nugent ≥7; 46.6%) and HPV (66.8%) were high in both communities. Prevalence of C. trachomatis and N. gonorrhoeae were >2-fold higher in Cape Town than Soweto (Chlamydia: 42% [62/149] versus 18% [26/148], p < 0.0001; gonorrhoea 11% [17/149] versus 5% [7/148], p = 0.05). Only 24% of adolescents with vaginal discharge-causing STIs or BV were symptomatic. In South African adolescents, clinical symptoms compatible with vaginal discharge syndrome had a sensitivity of 23% and specificity of 85% for the diagnosis of discharge-causing STI or BV. In a region with high HIV prevalence and incidence, >70% of young women with treatable conditions that could enhance HIV risk would have been missed because they lacked symptoms associated with syndromic management.
Introduction
Sexually transmitted infections (STIs) are one of the top five disease categories for which healthcare is accessed globally, with >1 million people infected daily. 1 Sexually active adolescents are at higher risk of acquiring STIs than their older adult counterparts. 2 This increased risk may be influenced by several factors, including relatively higher risk behavior, poor knowledge around STIs, 3 reduced access to sexual and reproductive health services, 4 participation in sexual networks with a high STI prevalence, 5 and a lack of acquired immunity to STIs. 6 Untreated STIs may influence reproductive morbidity including pelvic inflammatory disease, infertility, and cervical cancer in women. 7
In South Africa, young women (aged 15–24 years) bear the highest burden of HIV risk (∼2.5% incidence). 8 STIs are an important influence on HIV risk.9–12 Curable STIs account for ∼14% of new HIV infections in women, 13 and high HIV prevalence rates in this region may be driven by the synergy between HIV and the other common STIs.12,14 Even when asymptomatic, STIs are thought to influence HIV risk 15 by damaging the epithelial layer of the lower female reproductive tract and increasing genital inflammation, which increases target cell availability to the genital mucosa.16–19
Bacterial vaginosis (BV), a dysbiosis of the lower reproductive tract microbiome, is the most common cause of vaginal discharge in women of reproductive age. 20 BV also enhances the risk of HIV acquisition, 21 in addition to increasing complication rates of pelvic inflammatory disease, endometritis, preterm delivery, spontaneous abortion, and maternal/neonatal sepsis.22–24 BV also increases susceptibility to other STIs including Neisseria gonorrhoeae and Chlamydia trachomatis (1.8-fold and 1.9-fold, respectively). 25
Syndromic management, based on identification of defined clinical symptoms and signs, was introduced in South Africa and neighboring countries in the late 1990s, to improve management of symptomatic individuals with presumed STIs. 26 As well as treating the main STIs responsible for vaginal discharge, the vaginal discharge algorithm also enabled appropriate management of symptomatic BV and candidiasis. Syndromic management has led to a decrease in the prevalence of genital ulcer-associated sexually transmissible bacterial pathogens world-wide (e.g., Haemophilus ducreyi), although the approach has failed to control STIs where asymptomatic infections are common, such as chlamydial and gonococcal infections. 13 Untreated asymptomatic STIs and/or BV are important as they cause inflammatory changes in the lower female genital tract, which can increase the risk of HIV acquisition15,27,28 and result in reproductive complications. 29
To better understand the prevalence of asymptomatic STIs and BV in adolescent South African women, which may influence their HIV risk, the objective of this study was to compare the prevalence of symptoms associated with laboratory-diagnosed STIs and BV in two low-income South African communities.
Materials and methods
Cohort and specimen collection
Between November 2013 and February 2015, the Women’s Initiative in Sexual Health (WISH) study enrolled 298 young women (16–22 years old) from two South African communities with large adolescent populations and a high HIV incidence, located in Cape Town (through the Desmond Tutu HIV Foundation, DTHF, University of Cape Town) and Soweto (through the Perinatal HIV Research Unit, PHRU, University of the Witwatersrand). The objective of this study was to identify risk factors associated with HIV acquisition in South African adolescents, and to explore the granularity of risk across the country, by enrolling young women from resource-poor communities in two major cities (Johannesburg and Cape Town). Cape Town participants were recruited at a youth center, which offers family planning services while Johannesburg (Soweto) participants were recruited from community outreach programs. All participants were enrolled and had procedures done either at DTHF or PHRU. Both clinical sites offer adolescent-friendly, free STI syndromic management, condoms, and HIV counseling and testing with referral if needed. Women from Soweto attended a single study visit (due to budget constraints) while those from Cape Town were followed longitudinally for three visits: baseline and then every two months for four months if they were using norethisterone enanthate, combined oral contraception, NuvaRing® (Merck and Co., Kenilworth, NJ, USA) (offered to a participant as part of a previous study at the DTHF) or Implanon® (Merck and Co., Kenilworth, NJ, USA), or every three months for six months (enrollment and two further visits) if they used depot medroxyprogesterone acetate (DMPA) (Depo Provera®, New York, NY, USA) for ease of follow-up.
Eligible women were HIV-negative, sexually active, healthy, and neither pregnant nor menstruating at the first study visit. Two women in Soweto and one in Cape Town, who were screened out, were HIV-positive at screening and therefore not eligible to enroll. Pregnant women were excluded from the study and referred for appropriate care while those who were menstruating were asked to return two days after their menses were complete. Women were not enrolled if they had taken antibiotics in the previous two weeks. Women from both sites were counseled to abstain from sex, douching or using spermicides for 48 h prior to study visits. HIV status and pregnancy tests were confirmed negative at each visit with a HIV rapid test (Alere Determine™ HIV-1/2 Ag/Ab Combo, Alere, Waltham, MA) and a urine pregnancy test (U-test Pregnancy, Humor Diagnostica, Pretoria, South Africa), respectively.
A questionnaire to assess socio-demographics and sexual behavior was administered at enrollment. A pelvic exam was performed at each visit. A sub-analysis was done on women from Cape Town, where information was collected about any symptoms suggestive of STIs or BV (abnormal vaginal discharge, dysuria and vulval itching/burning). Participants were reimbursed ZAR50 for screening and ZAR150 for study visit, in accordance to SA Medicines Control Council regulations. 30
The Universities of Witwatersrand and Cape Town Research Ethics Committees approved this study. Women who were ≥18 years old provided written informed consent and those <18 years provided written assent and consent was obtained from their parent(s) or legal guardian(s).
Screening for BV and STIs
A vulvovaginal swab was collected at each visit for STI testing. Under speculum examination, a lateral wall/posterior fornix swab was collected for vaginal pH measurement, Nugent scoring for BV, and detection of fungal infection by microscopy using a Gram-stained vaginal smear. A Nugent score ≥7 was considered as BV, a Nugent score of 4–6 indicated intermediate vaginal flora, and smears with a Nugent ≤3 were considered normal flora. Vaginal pH was measured using color-fixed indicator strips (Macherey-Nagel, Düren, Germany). An endocervical swab was used for human papillomavirus (HPV) detection and genotyping. HIV rapid tests (Alere Determine™) were performed at each visit in the clinic from a finger prick sample. Serum for herpes simplex virus (HSV)-2 serology was collected in Cape Town only. Vulvovaginal swabs were assayed for the presence of N. gonorrhoeae, C. trachomatis, Trichomonas vaginalis, Mycoplasma genitalium, HSV, Treponema pallidum and H. ducreyi using real-time multiplex polymerase chain reaction (PCR) assays, as previously described. 31 Specimens that were positive for C. trachomatis were further tested for lymphogranuloma venereum-associated L1–L3 serovars. 31 HSV-positive specimens were typed with the HSV-I/II typing Real-TM PCR assay (Sacace Biotechnologies, Como, Italy). HSV-2 serology was performed using the HerpeSelect HSV-2 ELISA Kits (Focus Diagnostics, Cypress, CA, USA). HPV DNA was detected and genotyped using the Roche Linear Array HPV Genotyping assay (Roche Molecular Systems, Pleasanton, CA, USA).
Treatment of STIs and BV
Treatment was provided immediately to all women with a diagnosis of vaginal discharge syndrome according to the national STI management guidelines. In addition, those who were asymptomatic but with positive laboratory results were recalled for treatment. Individuals with C. trachomatis infections were treated with a seven-day course of doxycycline at the beginning of the study; this was later changed to a single 1 g dose of azithromycin to improve adherence. M. genitalium was treated with a single 1 g dose of azithromycin. N. gonorrhoeae was treated with 250 mg intramuscular injection of ceftriaxone, and T. vaginalis and BV (Nugent ≥7) with a 2 g single dose of oral metronidazole. Symptomatic fungal infections were treated with 1% clotrimazole cream. Women were given the choice of patient- or provider-initiated partner notification or treatment.
Statistical analyses
Statistical analysis was conducted using GraphPad Prism 6·0 (GraphPad Software, Inc., La Jolla, CA, USA) and STATA™ version 12 (StataCorp, College Station, TX, USA). Fisher’s exact test compared proportions; the non-parametric Mann–Whitney U test was used to compare sample means. Descriptive measures (such as median, standard deviation, interquartile range, frequencies, and percentages) were used to summarize data. Sensitivity, specificity and corresponding 95% confidence intervals assessed the predictive accuracy of each clinical condition.
Results
The study was censored on 28 February 2015, and not all Cape Town women completed all the visits (with 127/149 attended the second visit, and 88/149 all three visits). The majority of the adolescent women included in this study were high school students, living in the local communities in Cape Town or Soweto. They were between the ages of 16 and 22, having a median age of 18 (interquartile range [IQR]: 17–20) at enrollment, a median age of sexual debut of 16 years (IQR: 15–17), and a median of two sexual partners in their lifetimes (IQR: 1–13; Table 1). They were predominantly black (99%) South Africans (100%), who self-identified as heterosexual (99%).
Reported sexual risk behavior in adolescent and young women at baseline.

DMPA: depot medroxyprogesterone acetate; IQR: interquartile range; IV: intravenous; STI: sexually transmitted infection.
Young women from Cape Town reported lower rates of regular condom use than their Soweto counterparts (16% vs. 47% women reporting always using a condom, respectively; p = 0·0004) or condom use at last sex act (76% vs. 90%, p = 0·005). Twice as many adolescents from Cape Town reported multiple partners in the last 12 months (30% vs. 15%, p = 0·0076) and a higher frequency of previous STIs symptoms (16% vs. 8%, p = 0·0470) than those in Soweto. Adolescents from Soweto were more likely to report sex with a known or suspected intravenous drug user (9% vs. 1%, p = 0·0007) or inter-generational relationships (partner age difference ≥10 years; 13% vs. 4%, p = 0·0245). Reported transactional sex rates were low in both communities. Prior pregnancies in both groups of young women were high (23% in Cape Town and 27% in Soweto), with more pregnancies in Soweto (14%) being planned than in Cape Town (0%). There was one incident pregnancy in Cape Town during the study. There were no HIV seroconversions identified during follow-up of the longitudinal cohort.
High burden of C. trachomatis in young women
C. trachomatis DNA was detected in 30% (88/297) of the young women at enrollment. The chlamydial prevalence in Cape Town was almost three times higher than in Soweto (42% [62/149] vs. 18% [26/148], respectively; p < 0.0001; Table 2). None of the Chlamydia cases involved L1–L3 serovars.
·Clinical symptoms and laboratory-diagnosed STIs and BV in adolescent women.

HSV: herpes simplex virus; HPV: human papillomavirus; STI: sexually transmitted infection; BV: bacterial vaginosis; NA: not available.
HPV high-risk types = 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, 81, 82.
HPV low-risk types = 6, 11, 40, 42, 54, 55, 61, 62, 64, 67, 69, 70, 71, 72, 81, 82, 83, 84, CP6108, IS39.
Prevalence of other vaginal discharge-associated STIs
The prevalence of N. gonorrhoeae (8% [24/297]), T. vaginalis (5% [16/297]), and M. genitalium (4% [11/297]) infections were generally low. The burden of these bacterial STIs was similar in younger versus older women in the cohort (16–17 years compared to ≥18 years; data not shown).
Prevalence of genital ulcer-associated pathogens
No HSV-1 DNA was detected at either site at enrollment. However, in Cape Town, 4% (5/127) of women at visit 2 and 5% (4/88) at visit 3 was HSV-1 DNA positive. HSV-2 DNA was detected in 5% (7/149) of women in Cape Town and 1% (1/148) of woman from Soweto (p = 0.666). In Cape Town, where plasma was collected, 21% (31/149) of adolescents were HSV-2-seropositive at enrollment, and five adolescents became HSV-2 seropositive during follow-up. No cases of T. pallidum or H. ducreyi were detected.
HPV infections in adolescents
HPV DNA was detected 68% of women in Cape Town and 65% of those in Soweto (p = 0·6774). More than 50% of the HPV seen in both sites was high risk (p = 0.8979) (Table 2). Despite high prevalence of HPV infections, only two women in Cape Town were determined to have CIN1.
High burden of BV and intermediate flora in adolescents from two communities
More than 40% of the young women in the two communities sampled had BV (Nugent scores ≥7: 45% [64/143] in Soweto vs. 48% [71/147] in Cape Town; p = 0.4830) or intermediate flora (Nugent 4–6; 16% [24/143] in Soweto vs. 12% [17/147] in Cape Town; p = 0.3960), with a median vaginal pH of 5.0 (4.4–5.3) (5.0 [4.7–5.6] in Soweto vs. 4.7 [4.4–5.3] in Cape Town; p = 0.0015; Table 2).
STI recurrence or reinfection rates at repeat visits
Adolescents in Cape Town were followed for a total of three visits over six to eight months (Table 2). As part of this study, all those diagnosed with an STI or BV were treated. More than 60% of those infected with C. trachomatis at visit 3 were infected at all three visits (10/16), suggesting unresolved infections or re-infection (despite efforts to treat partners). Only two partners opted to come to the clinic for treatment, the majority of adolescents took treatment home for their partners. Similarly, despite metronidazole treatment for those with BV, 69% of adolescents with BV at enrollment also had BV at their second visit, and 37% had BV at all the three visits, suggesting high recurrence rates or a poor response to the single-dose metronidazole regimen. Other highly prevalent conditions, such as HPV infection, remained stable over all three visits (Table 2).
Clinical symptoms are poor indicators for STIs or BV in adolescents
Despite the high rates of laboratory-diagnosed STIs or BV detected in these female adolescent women, only 24% were symptomatic, with the most frequently reported STI-associated symptom being abnormal vaginal discharge (25%; Table 2).
Clinical symptoms were insensitive in diagnosing the discharge-causing STIs, with a sensitivity of only 23% (specificity 85%, positive predictive value [PPV] 50%, negative predictive value [NPV] 65%) for any symptom being present compared to evaluating abnormal discharge (sensitivity 21%, specificity 87%, PPV 46%, NPV 65%), genital burning/irritation (sensitivity 7%, specificity 96%, PPV 50%, NPV 64%), or dysuria (sensitivity 4%, specificity 94%, PPV 25%, NPV 63%) independently (Figure 1). Furthermore, having any symptom had an area under the receiver operating characteristic curve of 54% in identifying adolescent women with a discharge causing STI or BV (data not shown).
Sensitivity (top panel) and specificity (bottom panel) of clinical symptoms (dysuria, abnormal discharge, genital irritation, dyspareunia) and any other symptom for diagnosing a discharge-causing STI/BV (a), STI only (b); or BV only (c); together with their 95% confidence intervals.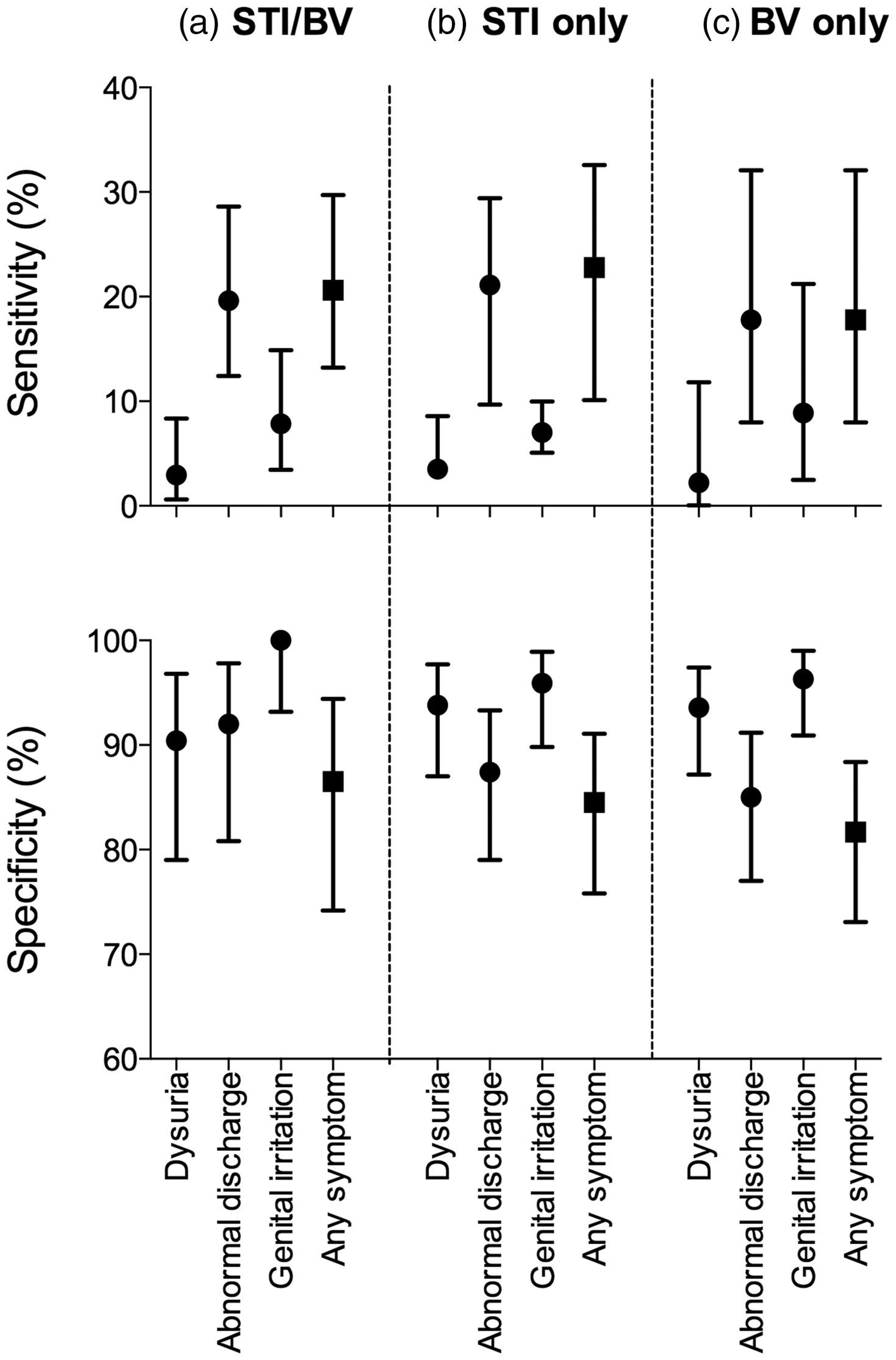
Discussion
In adolescent and young women at high risk for HIV infection from two low-income communities in South Africa, this study confirmed an extremely high prevalence of laboratory-confirmed STIs, in particular C. trachomatis infection, and BV. 32 Furthermore, a combination of clinical symptoms was a poor predictor of vaginal discharge-causing STIs or BV, with a sensitivity of 23% and specificity of 85% in this age group. The majority of adolescents/young women with an STI or BV were asymptomatic (76%), including those infected with C. trachomatis or N. gonorrhoeae, suggesting that reliance on symptoms alone is not effective in managing STIs in this setting, resulting in a highly prevalent and silent epidemic of undiagnosed genital tract infections that may increase HIV risk and/or reproductive complications.7,33,34 Although adolescents with symptoms were likely to be infected with an STI/BV, the majority were either asymptomatic or failed to recognize symptoms that would trigger the vaginal discharge syndromic treatment algorithm. With the roll-out of more affordable point-of-care diagnostics for STIs and BV and an ever expanding STI-focused vaccine agenda, adolescents should be prioritized in these efforts.
The very high prevalence of C. trachomatis in these adolescents was striking compared to the reported prevalence rates in other parts of Africa and worldwide (2.6% in African adult women 35 ; 4.7% in the United States 36 ) These high prevalence rates may be caused by a combination of factors, including the high proportion of asymptomatic infections, re-infection from untreated partners, lack of condom use, and participation in dense sexual networks harboring C. trachomatis.
The difference in prevalence rates of C. trachomatis seen in Cape Town (42%) compared to Soweto (18%) was marked. This was despite both cohorts being enrolled from similar socio-economic communities in Cape Town and Soweto. There were some important differences that could possibly account for this: reported behavior was generally riskier in Cape Town than Soweto, and the Cape Town site was also smaller and more isolated, possibly allowing high incidence sexual networks to evolve, while Soweto is bigger and more integrated into the urban environment.
This study had some limitations. Self-reported data, in the form of socio-behavioral questionnaires, were used to collect information and reporting bias may have occurred. Only the Cape Town cohort was followed longitudinally, and similar follow-up in Soweto would have enabled evaluation of treatment in a different population. Data on health-seeking behavior outside of the clinics were not available. Partners were not enrolled in our study and no information on their treatment or STI prevalence was available. The role of re-infection in maintaining STIs can therefore not be established. A single 2 g dose of metronidazole was used to treat vaginal discharge syndrome and while this is still recommended under the South African syndromic guidelines, this regimen results in higher failure rates than a one week’s course of treatment.37,38 Additionally, asymptomatic cases of BV are not normally treated. We did not examine the possibility of antimicrobial resistance for C. trachomatis or N. gonorrhoeae.
In conclusion, we report an extremely high prevalence of treatable STIs and BV in adolescent women from two communities in southern Africa who are at high risk for HIV infection. Given these findings that symptom-based treatment in young and adolescent women had an overall diagnostic accuracy of ∼50%, this study calls for an urgent review of the syndromic management policy, particularly for adolescents, and implementation of more reliable, affordable point-of-care NAATs and microscopy to diagnose these important reproductive infections, ideally within the current family planning clinic framework in place in South Africa.
Footnotes
Acknowledgements
We thank the WISH Study Teams particularly Ms Pinky Ngobo (Desmond Tutu HIV Foundation – participant recruitment), Sr Janine Nixon RN (University of Cape Town – sample collection), and all the young women who kindly participated in the study. Furthermore, this study would not have been possible without the technical and laboratory support offered by Ms Hoyam Gamieldien, Dr Lindi Masson, Mr Etienne Muller, Ms Venessa Masheku, Prof Lynn Morris, Ms Reveshnie Durgiah and Dr Zizipho Mbulawa. We are also grateful to Prof Francesca Chiodi (Karlinska Institute, Stockholm, Sweden), Prof Thomas Hope (Northwestern University, Chicago, IL, USA) and Prof Robin Shattock (Imperial College London, UK) for partnering with us on this EDCTP Strategic Primer study. Shaun Barnabas had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the European and Developing Countries Clinical Trials Partnership (EDCTP) Strategic Primer grant (SP.2011.41304.038) and the South African Department of Science and Technology (DST/CON 0260/2012). SLB was supported by the HIV Vaccine Trials Network SHAPe Program, the Fogarty Foundation and the South African Medical Research Council (MRC). SD was supported by the National Research Foundation (NRF) of South Africa and the Poliomyelitis Research Foundation. This work (ALW) was partially based upon research supported by the South African Research Chairs Initiative of the Department of Science and Technology and National Research Foundation. The DTHF also recognizes the support from ViiV health care in their YouthShield program. Perinatal HIV Research Unit was supported through funding from the South African MRC.
Ethical approval
University of Cape Town HREC Ref: 267/2013; University of Witwatersrand Clearance Certificate No: M1307.