
Abstract
The care of patients with HIV and Burkitt lymphoma poses a challenge to clinicians. Due to the limited treatment options that exist for relapsed/refractory Burkitt lymphoma, there is a need for the development of new therapies. This review aims to discuss evidence for current management strategies including chemotherapy and stem cell transplant, and highlight gaps in knowledge that will need to be addressed in the future.
Introduction
Burkitt lymphoma (BL) is an infrequent but very aggressive hematologic malignancy. 1 It may be overrepresented in human immunodeficiency virus (HIV)-infected patients. 1 In fact, recent statistics mention that in contrast to BL in the general population, BL comprised 25%–40% of HIV-associated non-Hodgkin’s lymphoma (NHL) before the era of highly active antiretroviral therapy. 2 The World Health Organization recognizes three clinical variants of BL: sporadic, endemic, and immunodeficiency related. 3 The last of these is particularly common in patients with HIV, in whom the lifetime incidence of BL has been estimated at 10%–20%. 3 The care of patients with both conditions poses a challenge to clinicians.
Interactions between Epstein-Barr virus (EBV) and HIV virus have been identified in the pathogenesis of BL. The presence of EBV confers a higher mutation rate in the lymphomagenesis process. 4 Studies have shown that EBV-negative BL arises from an early centroblast, while EBV-positive BL arises later in the development process from a memory B cell or late germinal center cell. 5 Gene expression signatures of the three variants also appear to be distinct. The expression of MyC is a near-universal phenomenon of BL.4–6
The use of concomitant high intensity chemotherapy regimens and antiretroviral therapy seems to be the standard of care. There is no preferred antiretroviral regimen but single tablet combinations are more pragmatic in the setting of toxic chemotherapy. No head to head comparison has been made among the standard chemotherapy regimens used (e.g. HyperCVAD, R-EPOCH, R-CODOX-RIVAC). Patients usually respond well to chemotherapy and cure rates of above 90% are commonly seen. Immune reconstitution of T cell counts is usually uneventful. 7 HIV RNA PCR viral loads are maintained during chemotherapy treatments.7–9 Relapse rates in HIV-infected populations appear to be higher compared to non-HIV-infected populations for reasons that are unknown. 9 Issues such as uncontrolled HIV viral load and its impact in the interaction between HIV PCR viral load and oncogenes is still unknown.
The management and treatment strategies of relapsed/refractory BL in the HIV-infected population have not been studied in depth. We perform a literature review of relevant information, treatment alternatives and the role of bone marrow transplant in patients with relapsed/refractory BL.
Epidemiology of BL in HIV-infected patients
BL patients present with higher risk features as compared with other NHL B-cell malignancies. 10 The salient features are usually the presence of extranodal diseases and poor Eastern cooperative oncology group score. 10 International prognostic index score is an independent prognostic factor for predicting overall survival (OS) and progression-free survival (PFS). 10
BL presents as sporadic, endemic, or epidemic disease. Endemicity is pathogenetically linked to an imbalance of the immune system, which occurs in African children infected by malaria parasites and EBV, while the epidemic form strictly follows the pattern of infection by HIV. BL shows propensity to extranodal involvement of abdominal organs, bone marrow, and the central nervous system, and can cause severe metabolic and renal impairment. Nevertheless, BL is highly responsive to specifically designed short-intensive, rotational multi-agent chemotherapy programs, empowered by the anti-CD20 monoclonal antibody rituximab. 11
In a recent study conducted by the Blood and Marrow Transplant Clinical Trials Network 0803/AIDS Malignancy Consortium 071 trial, seven cases of HIV-infected patients who underwent autografts for relapsed/refractory were reported. In this study, one-year transplant-related mortality was 5.2% for all cases of lymphoma autograft. 12
Treatment of BL in the HIV-positive patient population
Hoelzer et al. 13 was the largest prospective trial conducted for adult BL patients. This study sought to validate the efficacy of using rituximab in combination with short intensive chemotherapy for the treatment of BL. Patients enrolled in this study were treated with a total of six five-day cycles consisting of high-dose methotrexate, high-dose cytosine arabinoside, cyclophosphamide, etoposide, ifosfamide, corticosteroids and triple intrathecal therapy. A total of eight doses of rituximab were also given to each patient. The five-year OS in these patients was 80%, five-year PFS was 75% and complete response (CR) was 88%. Twelve percent of patients experienced relapse, with the most common sites of relapse being the central nervous system, either as the primary site or combined with other sites, followed by bone marrow.
Several European studies have applied the GMALL-B-ALL/NHL, 2002 protocol that was used in the Hoelzer et al. 13 study, validating the favorable results. The results of these studies are summarized in Table 1. The Intermesoli et al. 14 study assessed the long-term outcomes and toxicities of the B-NHL, 2002 regimen based on pre-treatment risk factors in high-risk adults with BL. Treatment was based on the extent of disease. Patients received six to eight cycles of rituximab and four to six courses of intensive chemotherapy with high-dose methotrexate, fractionated cyclophosphamide/ifosfamide, other drugs in rotation (i.e. vincristine, teniposide/etoposide, adriamycin), and intrathecal chemoprophylaxis with either methotrexate or cytarabine. HIV-positive and HIV-negative patients demonstrated similar rates in three-year OS, CR, and three-year PFS. The incidence of relapsed and refractory disease was greater among patients who were HIV negative compared to those who were HIV positive. In terms of toxicities, HIV-positive patients showed similar rates of hematologic toxicities to HIV-negative patients. HIV-positive patients also had significantly higher rates of gastrointestinal and hepatic toxicities when compared to HIV-negative patients. Furthermore, there was a statistically significant increase in febrile and infectious episodes other than sepsis/bacteremia and pneumonia in patients who were HIV positive.
Studies on the treatment of Burkitt lymphoma in the HIV-positive population.
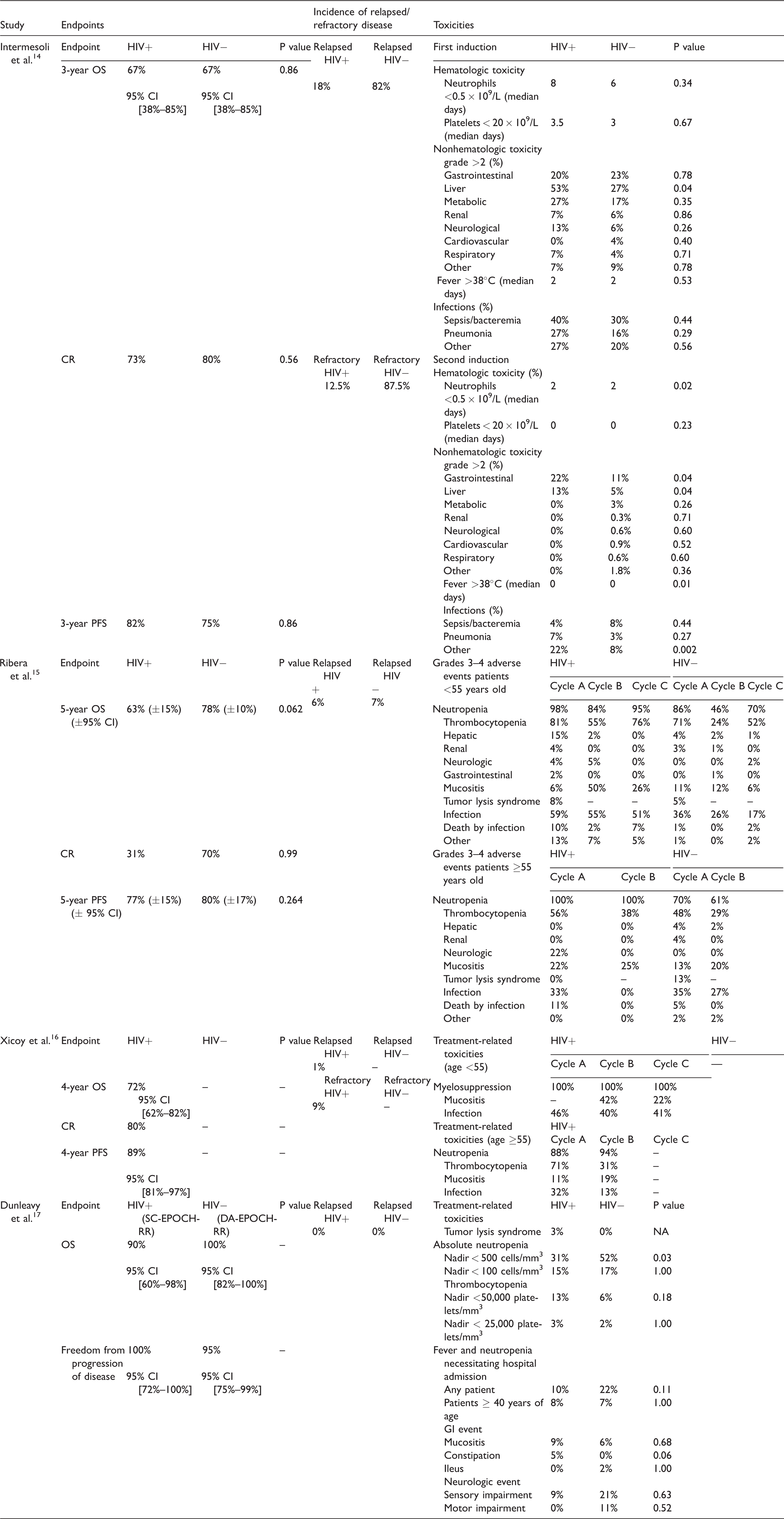
CI: confidence interval; CR: complete response; OS: overall survival; PFS: progression-free survival.
The Ribera et al. 15 study evaluated and compared the outcomes and toxicities of HIV-positive and HIV-negative patients with BL who were treated with either four or six cycles of intensive chemotherapy in combination with rituximab. There was no statistically significant difference in five-year OS, CR, and five-year PFS among HIV-positive and HIV-negative patients. Six percent of HIV-positive patients experienced relapse of disease while 7% of HIV-negative patients experienced relapse of disease. HIV-positive patients <55 years of age experienced significantly more hematologic toxicity, mucositis, and infections compared to HIV-negative patients <55 years of age. There was no difference in toxicity among those HIV-positive and HIV-negative patients ≥55 years of age.
Xicoy et al. 16 examined the effects of dose-intensive immunochemotherapy in HIV-related BL in Spanish and German cohorts. Eighty percent of patients achieved CR. Four-year OS was 72% and four-year PFS was 89%. There were no differences between the two cohorts of patients. In terms of treatment-related toxicities, myelosuppression (including neutropenia and thrombocytopenia), mucositis and infection were the most common toxicities experienced by patients in both cohorts. The authors of this article concluded that rituximab in addition to intensive chemotherapy was effective but toxic in HIV-related BL.
A study published in the New England Journal of Medicine, Dunleavy et al., 17 compared the effects of two EPOCH-R regimens. Standard DA-EPOCH-R was administered to HIV-negative patients while a lower-dose short-course with a double dose of rituximab (SC-EPOCH-RR) was administered to HIV-positive patients. OS and rate of freedom from progression of disease in the DA-EPOCH-R group were 100% and 95%, respectively. In the SC-EPOCH-RR group, OS and rate of freedom from progression of disease were 90% and 100%, respectively. Recurrence of disease and deaths from BL were absent in both groups. The most common treatment related toxicities in both groups were absolute neutropenia and fever and neutropenia necessitating hospital admission.
Treatment options in the setting of relapsed/refractory BL
Per the most recent guidelines, there are no clearly defined treatment options for relapsed/refractory BL. Ideally, patients experiencing relapsed/refractory BL should be treated with a well-designed clinical trial.18,19 On the contrary, patients who have reasonable duration of remission after first-line induction chemotherapy can be treated with second-line chemotherapy in combination with rituximab-containing regimens, high-dose chemotherapy and autologous or allogeneic hematopoietic stem cell transplant (HSCT). 19 Second-line therapy should consist of chemotherapeutic agents that the patient was not previously exposed to or only partially exposed to. 20 Commonly used second-line agents include: dose-adjusted EPOCH (etoposide, prednisone, vincristine, cyclophosphamide, doxorubicin) plus rituximab and intrathecal (IT) methotrexate (MTX); RICE (rituximab, ifosfamide, carboplatin, etoposide) plus IT MTX, if not administered previously; RIVAC (rituximab, ifosfamide, cytarabine, etoposide) plus IT MTX, if not administered previously; RGDP (rituximab, gemcitabine, dexamethasone, cisplatin); or high dose cytarabine plus rituximab. Unfortunately, there are limited data on the efficacy of these regimens for the treatment of relapsed/refractory BL. 19 One study that demonstrated efficacy, Griffin et al., 21 looked at the effect of RICE in pediatric patients with relapsed/refractory B-cell and NHL lymphoma. Out of the 14 patients with BL and B-ALL, 28.6% achieved CR and 35.7% achieved PR. Correspondingly, salvage therapy in this population is generally ineffective. 12
Depending on their condition, some patients may not be suitable for treatment with either a clinical trial or subsequent intensive combination chemotherapy regimens. In these instances, the appropriate treatment would be management with best supportive care.19,22 Best supportive care includes management of pain, dyspnea, anorexia and/or cachexia, nausea and vomiting, constipation, diarrhea, malignant bowel obstruction, fatigue, delirium, and psychological distress. 23
Due to the limited treatment options that exist for relapsed/refractory BL, there is a need for the development of new therapies. Currently, there are ongoing clinical trials investigating the benefit of using bromodomain and bromodomain extraterminal (BET) inhibitors for the treatment of newly diagnosed or relapsed BL.18,24 Bromodomains are proteins that have a high affinity for binding to acetylated histone proteins in chromatin. BET inhibitors selectively inhibit the interaction between BET proteins and chromatin as well as regulate gene transcription. 25 JQ1, a BET inhibitor, effectively decreased c-MyC expression in the BL cell line Raji in vitro in addition to inhibiting tumor growth without causing significant adverse effects. Furthermore, JQ1 improved survival in a mouse model xenografted with the Raji cell line.25,26 BET inhibitors, such as OTX015 and I-BET151, have also proven to be beneficial in several other BL cell lines due to their antiproliferative effects.27,28
Additionally, there are presently over one hundred studies on adult relapsed/refractory BL in the National Institute of Health’s clinical trials database. Some of these studies have investigated the effects of novel drugs with unique mechanisms of action, such as Belinostat, Ixabepilon and Imexon. Table 2 summarizes the results of these trials as well as provides the mechanisms of these novel therapies. Other trials on the horizon that are investigating patients with relapsed/refractory BL include: Pembrolizumab and Ibrutinib in treating patients with relapsed or refractory NHL; Alisertib and Romidepsin in treating patients with relapsed or refractory B-cell or T-cell lymphomas; Nivolumab with or without Varlilumab in treating patients with relapsed or refractory aggressive B-cell lymphomas; and Venetoclax, Ibrutinib, Prednisone, Obinutuzumab, and Revlimib (ViPOR) in relapsed/refractory B-cell lymphoma. 29
Novel antineoplastic agents for relapsed/refractory Burkitt lymphoma.
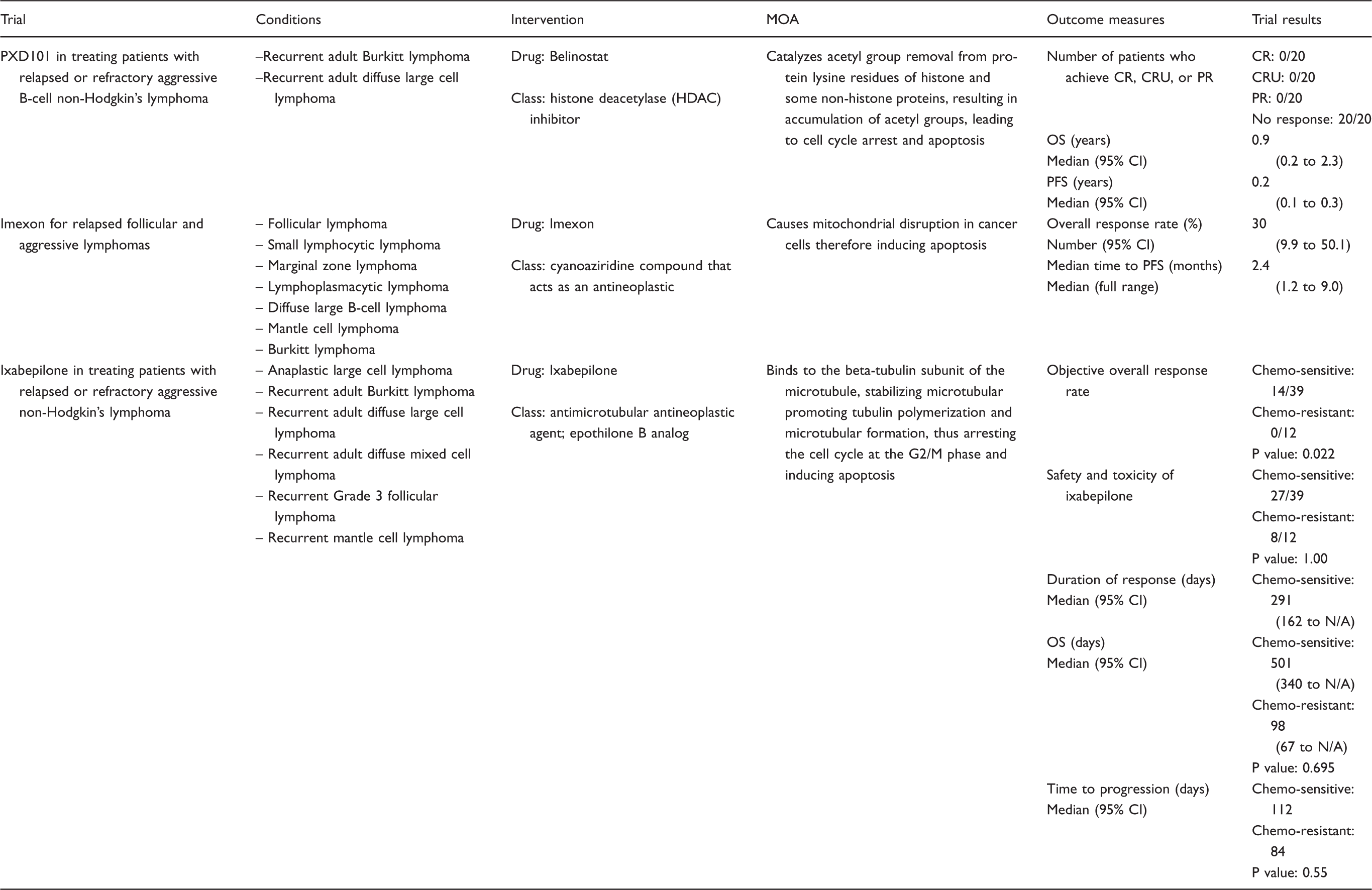
CR: complete response; CRU: complete response unconfirmed; PR: partial response; OS: overall survival; PFS: progression-free survival; MTD: maximum tolerated dose.
Role of stem cell transplantation
While stem cell transplantation (SCT) in the setting of relapsed/refractory BL has been studied, the results have not been promising. For instance, in a retrospective review from the European Group for Blood and Marrow Transplantation, the overall survival (OS) at three years of patients with chemo-sensitive relapse was compared to the OS at three years of those with resistant disease treated with autologous SCT. The OS at three years for chemo-sensitive relapse patients was 37% compared to 7% for chemo-resistant relapse patients. 22 At present, there are no data to suggest that allogeneic transplant is beneficial for the treatment of relapsed/refractory BL. 12
Reports on bone marrow transplant in HIV-infected patients come from few centers. The most extensive review, a phase II trial of 50 patients who underwent autograft stem cell transplant, comes from the Blood and Marrow Transplant Clinical Trials Network 0803/AIDS Malignancy Consortium 071 trial. Patients received a preparative regimen consisting of carmustine, etoposide, cytarabine, and melphalan and received consistent management of peri-transplant antiretroviral treatment. A total of 43 patients were enrolled; 40 underwent autologous hematopoietic cell transplantation. At a median follow-up of 24.8 months, one-year and two-year OS probabilities were 87.3% (95% confidence interval [CI], 72.1–94.5) and 82% (95% CI, 65.9–91), respectively. One-year transplant-related mortality was 5.2%. Median time to neutrophil and platelet recovery was 11 days and 18 days, respectively. 12
Conclusion
Despite being a highly curable disease in the initial presentation, relapsed BL is less responsive in the refractory setting. Relapsed/refractory BL in HIV patients appears to happen with more frequency that in their non-HIV counterparts. There are still no clear data to deduce appropriate management strategies including preferred antiviral therapy combinations and preferred chemotherapy regimens. The benefit of autologous SCT at second remission appears to be present only in chemo-sensitive disease. The benefit of allogeneic SCT at second complete remission is still debatable.
With the aging of the HIV population, presence of more comorbidities, presence of more complex geriatric syndromes, less functional capabilities and potentially increasing cases of BL with consequent increasing frequency of relapse/refractory disease cases, a more comprehensive approach in the management of this condition is needed. Further clinical trials including relapse/refractory patients with HIV infection are also needed.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.