
Abstract
This study compared sexually transmitted infection (STI)-associated risks between young Black cisgender men who have sex with men (YBMSM) and young Black transwomen who have sex with men (YBTWSM). Comparisons pertained to: (1) prevalence of infections; (2) sexual risk; (3) partner-related risks; and (4) socioeconomic marginalization. YBMSM (n = 577) and YBTWSM (n = 32) were recruited from an STI clinic in the USA. Volunteers completed a computer-assisted self-interview and medical records were abstracted for STI/HIV information. Significantly greater prevalence of pharyngeal Chlamydia (P < .001) and pharyngeal gonorrhea (P = .04) occurred among YBTWSM; however, both associations were moderated and only significant for HIV-uninfected volunteers. YBTWSM had more oral sex partners and more frequent engagement in oral sex. The number of new sex partners for anal receptive sex was greater in YBTWSM. YBTWSM were more likely to exchange sex for money/drugs (P < .001), have sex with men recently in prison (P < .001), who were “anonymous” (P = .004), or who were “one night stands” (P < .001). YBTWSM were more likely to depend on sex partners for money food, etc. (P < .001), to miss meals due to lack of money (P = .01), and to report having ever being incarcerated (P = .009). Compared to cisgender YBMSM, YBTWSM experience multiple risk factors relative to the acquisition/transmission of STIs and HIV.
Keywords
Introduction
Worldwide, young transgender women who have sex with men are at significant increased risk of HIV acquisition.1,2 The World Health Organization includes transgender people as one of four populations at greatest risk of HIV acquisition. 1 In the United States, this already heightened risk is further magnified when considering the inordinate proportion of young Black males (a biological term) who have sex with HIV-infected males, thus inflating the odds of young Black males whose gender identity is that of transgender women, and who have sex with males, encountering infected HIV-infected partners. 3 In this article, young Black men who have sex with men (YBMSM) and whose gender identity is also male are referred to as cisgender YBMSM. In contrast, young Black biological men who have sex with men (YBMSM) and who identify as transgender women are referred to as young Black transwomen who have sex with men (YBTWSM).
Unfortunately, U.S. public health surveillance data have not distinguished YBMSM and YBTWSM, thereby limiting the information that is specific and unique to YBTWSM. What is known for the U.S. is that YBMSM (including YBTWSM) have experienced a far more rapid escalation of the HIV/AIDS epidemic than MSM who identify as White or Latino or any other sub-population in the U.S.3–8 One important estimate of the HIV burden among YBTWSM comes from the National HIV Surveillance System, which first included reports of HIV incidence among transwomen from 2009 to 2014. Of the incident cases among transwomen, 50.8% were non-Hispanic Blacks. 9 The U.S. CDC estimates that just over 50% of all transwomen living with HIV in the U.S. are Black. 3 YBTWSM experience adverse social and structural conditions that contribute to their HIV risk and that are markedly different from those experienced by YBMSM.1,2,10–12 Thus, specific considerations in regards to research and intervention development are warranted.1,9,11,12
Transwomen experience a high burden of HIV worldwide with pooled prevalence estimates at just under 20%. 13 In the U.S., the burden of HIV for transwomen may be even higher, especially among Black transwomen.13–15 Estimates from a meta-analysis suggest that roughly 56% of Black transwomen tested positive for HIV as compared to one of every six for White and Hispanic transwomen. 14 A particularly poignant question involves the sexually transmitted infection (STI)-related risk of YBTWSM. The current study sampled young, Black males (those assigned male at birth) who have sex with males and then used ensuing answers to survey data to create two groups: those identifying as cisgender (YBMSM) and those identifying as transwomen (YBTWSM).
A key aspect, one often overlooked, of sexual health for YBMSM and YBTWSM is the acquisition of non-viral STIs. In addition to the direct morbidity caused by these infections, heightened risk of HIV acquisition (for those who are HIV-uninfected) and transmission (for those who are HIV-infected) has been well established.16–19 Unlike studies with a focus strictly on HIV, the investigation of differences in non-viral STIs among MSM and transwomen necessitates the corresponding investigation of differences in oral and anal sex behaviors. For instance, one recent study in Peru examined extra-genital chlamydial or gonococcal infections among MSM and transgender women and found that transgender women were twice as likely to be infected with a pharyngeal infection. 20 To date, no studies in the U.S. have specifically compared the site-specific prevalence of STIs between YBMSM and YBTWSM.
Although many studies of transwomen in the U.S. have described risk factors relative to sexual risk behaviors,21–27 few have taken place in the southern U.S., 28 which bears a disproportional burden of the HIV/STI epidemic.29–32 Moreover, studies to date have not directly compared the sexual risk behaviors of young Black transwomen who have sex with men to those of their YBMSM cisgender counterparts (recruited in the same sample).
Finally, it is vital to investigate and better understand the behavioral aspects of sexual risk that transcend simply counting acts of sexual behaviors (i.e. frequency). This is achieved by considering whom people select as sex partners within the context of the possible socioeconomic marginalization experienced by transwomen.14,24,33
Accordingly, the purpose of this study was threefold: To compare YBTWSM to YBMSM regarding: (1) the prevalence of site-specific Chlamydia and gonorrhea infections, as well as past syphilis infections, (2) selected sexual risk behaviors, and (3) measures of “who” their sex partners have been in the past 90 days and selected measures of socioeconomic marginalization.
Methods
Study sample
This is a secondary analysis of data collected as part of an NIH-funded randomized controlled trial (RCT) of a safer sex intervention program designed specifically for YBMSM. A convenience sample of 600 young Black males (assigned male at birth) who have sex with males was recruited. Only baseline data (collected before randomization and intervention) are presented. Participant recruitment occurred in a federally-supported clinic designated for the diagnosis and treatment of HIV and other STIs. The clinic was located in a mid-size southern city where incidence rates of HIV are particularly high. Inclusion criteria included: (1) assigned male at birth; (2) self-identification as Black/African American; (3) aged 15 to 29 years; (4) attending the clinic to be tested for HIV or other STIs, (5) having engaged in anal sex with a male partner at least once in the past six months, and (6) the ability to speak and comprehend English.
From September of 2012 through October of 2015, based on review of charts for age, gender at birth, and identifying as Black, potential volunteers were approached in the clinic waiting area and asked about their interest in participating in an HIV prevention study. Using an electronic tablet, those expressing interest were screened for eligibility. Those screening eligible and expressing interest in study enrollment were taken to a private room in the nearby clinic for consenting and completing the baseline interview. In the event that time did not allow any given volunteer to complete the consenting and interviewing process on the day of recruitment, an appointment was made to return within the next three days. All study procedures were approved by the Institutional Review Boards of the participating universities.
Study procedures
After providing written informed consent (or parental consent for those under 18 years of age), participants completed an online questionnaire using Qualtrics© (Provo, UT, USA) in a private office not physically connected to the clinic. The self-administered questionnaire had an optional audio component in the event that men experienced literacy issues. The questionnaire collected information relative to sociodemographic characteristics, including age, race, gender identity, sexual risk behaviors, and their sexual experiences.
Biological outcome measures
Seven biological outcomes were assessed. All participants were evaluated for Chlamydia and gonorrhea in three anatomic locations: urethral and rectal infections were detected through nucleic acid amplification testing (NAAT) performed on a urine specimen and a rectal swab, respectively; oral infections were detected through NAAT testing of an oral swab. In addition, HIV testing was performed (if not HIV-infected) by using Clearview® Complete HIV 1/2 (Alere™, Waltham, MA, USA) or by standard HIV test processed at the Mississippi State Department of Health Public Health Laboratory (MSDH PHL) in blood specimens. Syphilis screening was performed with the rapid plasma reagin (RPR) processed at the MSDH PHL. Medical records were abstracted for HIV and STI test results corresponding at the study visit, including verification of HIV status for those reporting to be HIV infected.
Self-reported outcome measures
Eleven items assessed selected sexual risk behaviors, using a 90-day recall period. These included measures related to anal sex (both receptive and insertive), oral sex, and sex with new partners (with “new” being defined as occurring in the past 90 days).
Seven measures of “who” study participants had sex with recently (past 90 days) were assessed. These were: (1) “Have you had anal sex with a male in exchange for money or drugs?”; (2) If yes to #1, “How many times have you been paid to have sex with a guy?”; (3) “Do you depend on your sexual partners for any of the following? (transportation, food, money, drugs, gifts, or housing)”; (4) “Have you had anal sex with a male recently released from prison?”; (5) “Have you had anal sex with a male you did not know at the time?”; (6) “Have you had a one night stand, meaning you had anal sex with a male you just met that same day/night and you have not had anal sex with that male again?”; and (7) “How many female sex partners have you had (not counting oral sex)?”
Five items of socioeconomic marginalization were assessed. These were: (1) “In the past 12 months have you missed meals because you didn’t have enough money to eat?”; (2) “In the past 12 months, have you had to borrow money to get by?”; (3) “In the past 12 months have you received food stamps?”; (4) An item asking how many cell phone numbers volunteers had in the past 12 months (those indicating “0” were coded as not having a cell phone); and (5) “How many times have you been incarcerated?”
Data analysis
The primary predictor variable was gender identity and was based on a single question: “Do you consider yourself transgender – an MTF (male-to-female) person?” Those replying “yes” were classified as YBTWSM and compared to those replying “no.” Outcome measures were restricted to sexual risk behaviors occurring in the past three months. The questionnaire included 11 items relative to STI-related sexual risk and protective behaviors.
Contingency table analyses, using chi-squared tests, were used to determine bivariate associations between gender identity and the dichotomous outcomes. Because a relatively small proportion of the sample identified as transwomen, which created a statistical power issue, the rate ratio (rate in transwomen/rate in YBMSM) was used as a supplement to significance testing.
Independent group t-tests were used to evaluate the bivariate associations between gender identity and the outcomes assessed at a continuous level. Again, due to low statistical power a supplemental measure of association was used: the percent relative difference (PRD) (difference between means/mean of YBMSM × 100). A PRD value of >.50 was considered meaningful. 34
Finally, for the tests of association with prevalent non-viral STIs, each association was also evaluated for an interaction effect with HIV status. This was done by use of layered chi-square analyses. Interactions were declared to occur when one of the two Chi square tests (either the tests among HIV-uninfected or among HIV-infected volunteers) was significant and the other was not significant.
Results
Sample and demographic characteristics
A total of 890 were screened; of these, 630 were eligible. After being offered the opportunity to enroll, 21 declined, and 9 were enrolled in a pilot study only, yielding an overall participation rate of 96.6% and a sample size of 600 volunteers.
Mean age was 22.62 years (SD) = 3.2. An average monthly income of less than $1000 was reported by 46.1%. The majority of participants (58.6%) reported they were currently employed. More than one-half of the sample (59.8%) reported having education beyond high school graduation and 47.3% reported currently enrollment in a school or college. Table 1 displays these and other characteristics stratified by identification as transgender versus cisgender MSM.
Characteristics of the sample, stratified by identification as transgender versus cisgender MSM.
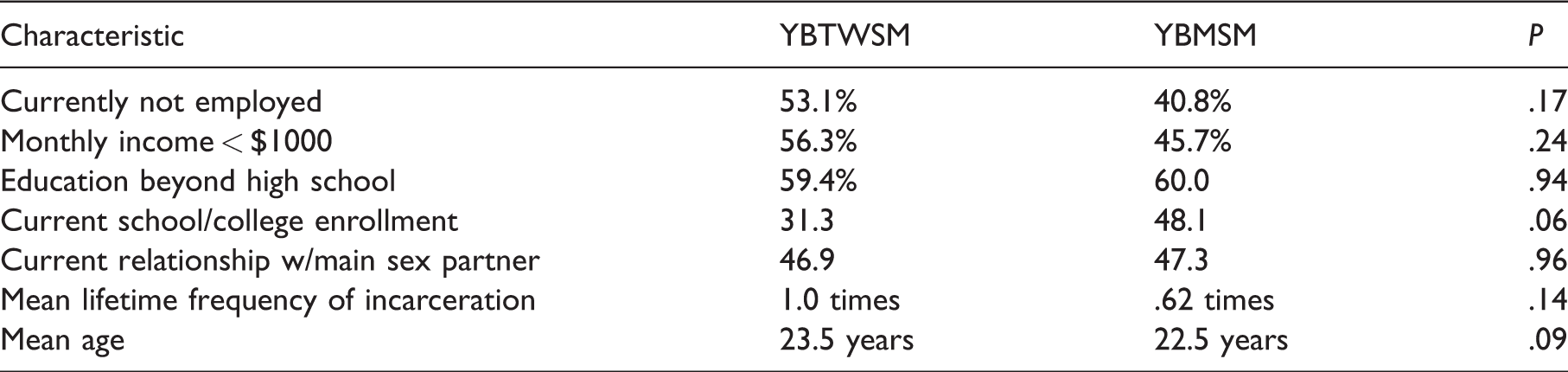
YBMSM: young Black cisgender men who have sex with men; YBTWSM: young Black transwomen who have sex with men.
Given the large percent of HIV-infected volunteers (25.5%), it was important to determine whether differences in HIV status occurred between the two groups. Among the YBTWSM with valid HIV test results (n = 31), 8 (25.8%) were HIV-infected versus 132 (25.4%) of 519 YBMSM with valid test results (not significantly different).
Prevalence of STIs
Table 2 displays the prevalence rates for seven STIs and depicts group comparisons between YBTWSM and YBMSM. As shown, only pharyngeal Chlamydia and pharyngeal gonorrhea were significantly associated with the YBTWSM group. In each case, these infections were significantly more likely to be diagnosed among YBTWSM.
Comparison of site-specific prevalence of selected sexually transmitted infections by group.
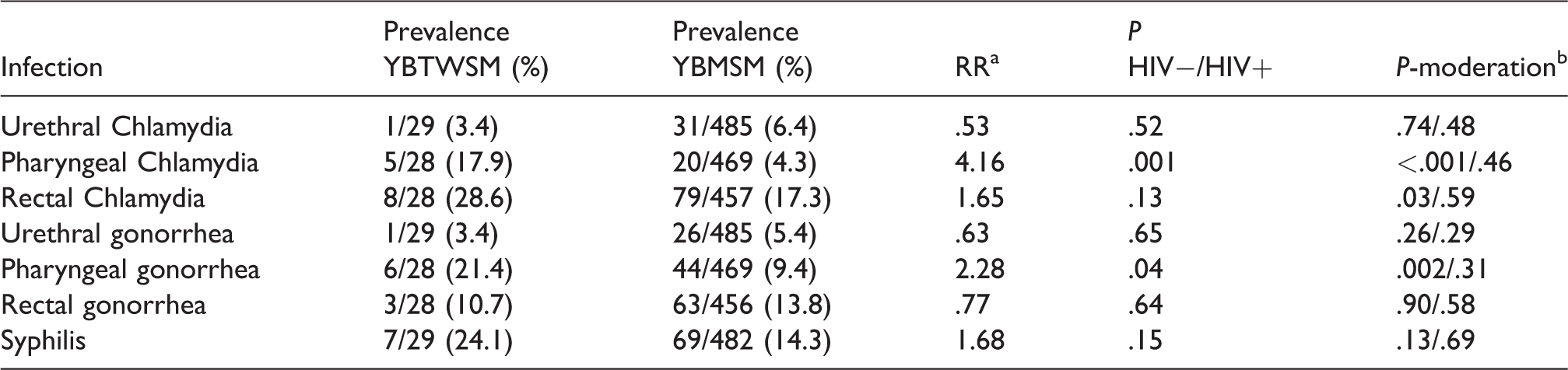
YBMSM: young Black cisgender men who have sex with men; YBTWSM: young Black transwomen who have sex with men.
aRate ratio (YBTWSM prevalence/YBMSM prevalence).
bIn each case where moderation occurred, the association was only significant for HIV-uninfected volunteers.
Additionally, the far right-hand column of Table 2 shows whether the association between infection and gender identity group was moderated by HIV status. This column shows the P-value for volunteers who were HIV-uninfected and the P-value for HIV-infected volunteers. As shown, moderation occurred for three associations, with each being significant only for those who were HIV uninfected. Thus, among HIV-uninfected volunteers, the prevalence of pharyngeal Chlamydia was 23.8% among YBTWSM versus 3.2% for YBMSM (P <.001). For rectal Chlamydia, prevalence was 33.3% among HIV-uninfected YBTWSM versus 15.2% for HIV-uninfected YBMSM (P =.03). Lastly, for pharyngeal gonorrhea, the prevalence was 28.6% among HIV-uninfected YBTWSM versus 8.1% for HIV-uninfected YBMSM (P= .002).
Differences in sexual risk behaviors
Table 3 displays the bivariate associations between gender identity and 11 sexual risk behaviors. As shown, using the significance criteria of >50.0 PRD, 5 of 11 differed and each indicated greater risk for YBTWSM compared to YBMSM. Additionally, YBTWSM reported a relatively greater number of sex partners when they were the “bottom” or receptive partner, more frequent sex as a “bottom” or receptive partner, and more frequent sex as a “top” or insertive partner with a new partner, compared to YBMSM. Lastly, YBTWSM reported having a greater number of oral sex partners and more frequent oral sex compared to YBMSM.
Bivariate associations between identification as transwomen and 11 sexual risk behaviors (using a 90-day recall period) among YBTWSM and YBMSM.
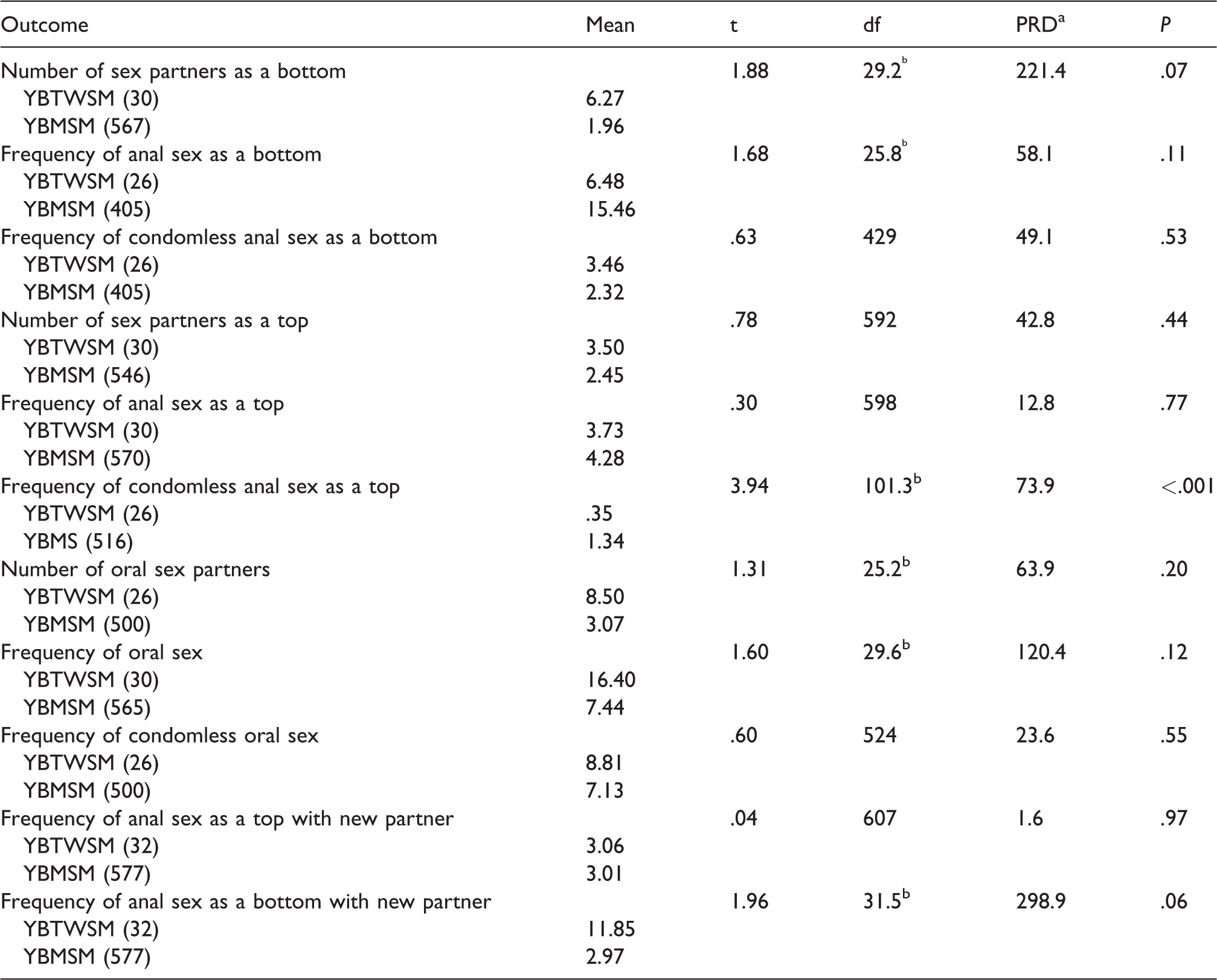
YBMSM: young Black cisgender men who have sex with men; YBTWSM: young Black transwomen who have sex with men; PRD: percent relative difference.
aCalculated as the difference between means/mean of YBMSM × 100.
bDue to lack of homoscedasticity (inequality of variances) the t-test was conducted with an unequal variances method.
Differences in sex partners and socioeconomic marginalization
Table 4 displays the associations with seven measures of “who” volunteers had as sex partners and five measures of socioeconomic marginalization. As shown, 8 of the 12 measures had significant associations with gender identity. For each measure, the direction of association suggests greater risk for YBTWSM. Of the four tests not obtaining significance, two had marginal P-values: (1) the measure of borrowing money “just to get by” (P = .06) had a rate ratio of 1.42 (falling under the same 50% criteria used for the PRD) and (2) the measure of receiving food stamps (P = .08) had a rate ratio of 1.54 (being above the 50% criteria used for the PRD).
Comparison of measures representing “Who” study volunteers had sex with and socioeconomic marginalization, by identification as YTWSM and YBMSM.
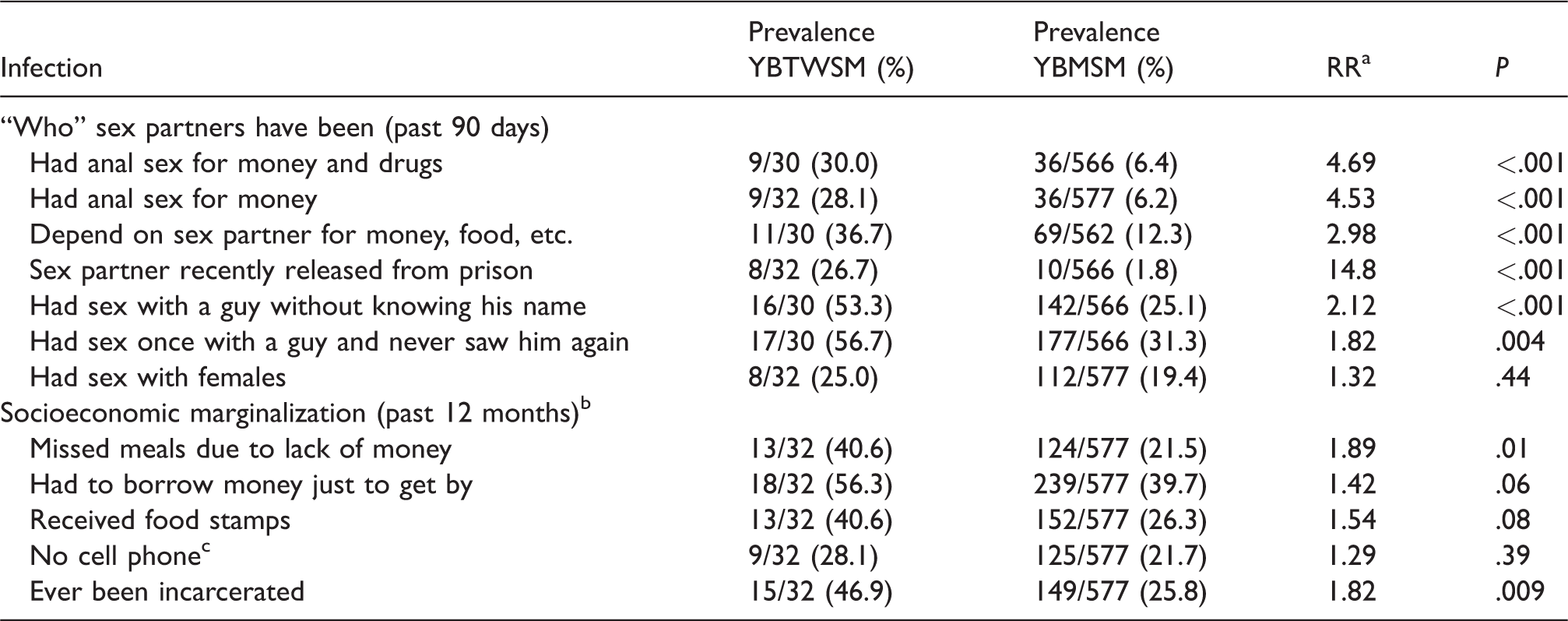
YBMSM: young Black cisgender men who have sex with men; YBTWSM: young Black transwomen who have sex with men.
aRate ratio (YBTWSM prevalence/YBMSM prevalence).
bWith the exception of the last table entry (ever been incarcerated).
cThis variable was used as a proxy measure of poverty.
Discussion
This empirical study reports findings from a sample of MSM living in an area of the southern U.S. characterized by high incidence of HIV and that examined behavioral, social and structural differences between those identifying as YBMSM and those identifying as YBTWSM. Our findings suggest the possibility that YBTWSM may have the same or greater level of HIV risk compared to their YBMSM counterparts. For example, with the exception of significantly elevated prevalence of pharyngeal Chlamydia and pharyngeal gonorrhea among YBTWSM, the biological laboratory findings show similar and high rates of confirmed Chlamydia, gonorrhea, and syphilis. Although direct causation cannot be determined, the greater number of pharyngeal infections may stem from a greater number of oral sex partners and a greater frequency of engaging in oral sex among YBTWSM. Although our measure of oral sex was not behaviorally specific (i.e. insertive vs. receptive), the prevalence of pharyngeal infections suggest that YBTWSM may be more likely to be receptive during oral sex if not both receptive and insertive. One potential clinical implication from these findings is the need to intensify oral screenings for STIs among YBTWSM.
Our findings also suggest the possibility that YBTWSM are more likely than YBMSM to have a greater number of male sex partners, who are insertive for anal sex, thereby augmenting the risk for rectal infections if condoms are not used consistently and correctly. Differences in reported condom use during anal receptive sex were not observed; however, this apparent protective behavior among the YBTWSM in our sample may explain the relative equivalence in laboratory-confirmed rectal infections between YBTWSM and YBMSM. Additionally, although YBTWSM reported significantly more frequent anal receptive sex, rates of condomless anal receptive sex remained equivalent to those reported by YBMSM. This may also explain the similar HIV infection rates observed for both groups. Notably, HIV rates among transwomen in our study contrast with the rates reported in the literature that place Black transwomen at a substantial higher risk of HIV infection. 13
Pre-exposure prophylaxis (PrEP) may be a particularly important prevention option for YBTWSM. Further, condom use remains an important STI and HIV prevention strategy for this vulnerable population, especially with respect to averting pharyngeal infections. Thus, STI/HIV prevention efforts to strengthen and reinforce condom use for anal receptive sex among YBTWSM are greatly warranted and should be continued, particularly in low-resources areas, where STI/HIV infection is common (i.e. the deep south).
The findings relative to the third study objective were particularly intriguing and have several implications. Collectively, these findings provide important evidence that YBTWSM may be engaging in sex with males at high risk of having HIV/STIs. This includes males who pay for sex, give drugs in exchange for sex, have recently been released from prison, are “anonymous”, and are “one night stand” partners. The corresponding findings relative to YBTWSM being more likely to depend on sex partners for money, food, shelter, etc. and being more likely to miss meals due to a lack of money support the hypothesis that the socioeconomic marginalization of YBTWSM may foster a reliance on alternative economies as a means to survive.
Limitations
In addition to the use of a convenience sample and a cross-sectional study design, four other limitations apply to the findings. First, the study assessment protocols were constructed prior to FDA-approval of PrEP; thus, study volunteers were not asked about their use of PrEP even though many enrolled in the study after approval occurred. Second, the study did not oversample YBTWSM and thus the relatively low number (i.e. 31) created a substantial imbalance between the two groups thus compromising statistical power. Unfortunately, however, oversampling would require extensive pre-screening – a somewhat personal set of questions would be asked and this may pose issues relative to ethics given that study enrollment had not yet occurred. Third, the use of only one clinic greatly precludes generalizations to other areas of the southern U.S. Clearly, an ideal study would use probability sampling across multiple cities/clinics located in the southern U.S. Finally, the lack of adequate sample size regarding YBTWSM may have led to power issues relative to interpreting interaction effects.
Implications and conclusions
One implication of the study findings is that clinics and clinicians may improve STI/HIV prevention efforts for YBTWSM by serving as a referral agent for transwomen to social services that may address issues of hunger, employment, and housing instability. Further, structural-level interventions may be vital for rectifying the observed disparities existing for YBTWSM, e.g. making legal name change easy, strengthening employment protection policies for transwomen, and providing gender-affirming healthcare services. Taken as a whole, our study findings highlight the possibility that although YBTWSM and YBMSM may both constitute the bio-behavioral category of “men who have sex with men” their unique lived experiences may yield significantly different STI and HIV risk profiles, and they may engage with sex partners in markedly different ways which may decrease and/or increase STI and HIV risk. The unique relational risks experienced by YBTWSM warrant more in-depth investigation, including qualitative research that uncovers disclosure-related issues relative to being transgender. The findings also extend past research with non-clinic-based samples of transwomen that collectively describes a syndemic of health issues and health risk behaviors among transwomen.24,35–38
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the National Institutes of Mental Health, R01MH092226.