
Abstract
Previous studies have demonstrated a link between protease inhibitor (PI)-based therapy and lipid dysregulation. The main objective of this study was to examine whether cocaine use may modify PI-associated dyslipidemia in adults. Between June 2003 and June 2014, 957 human immunodeficiency virus (HIV)-infected participants in Baltimore, Maryland were enrolled in a study that investigated HIV/antiretroviral therapy-associated comorbidities. Multiple linear and logistic regression models were fitted to examine the associations between PI therapy and lipid profiles for the pooled sample and cocaine use subgroups, respectively. Total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), TC/high-density lipoprotein cholesterol (HDL-C) ratio, and atherogenic index of plasma (AIP) levels were positively associated with duration of PI-based therapy in long-term cocaine users (all p < 0.05). However, longer-term PI therapy was significantly associated with increased HDL-C in non-chronic cocaine users (β = 0.109, SE = 0.042, p < 0.05). The participants who received PI therapy ≥12 months and used cocaine ≥15 years were more likely to have hypertriglyceridemia (OR = 2.82, 95% CI = 1.63, 4.88) and abnormal AIP (OR = 1.73, 95% CI = 1.08, 2.79) as compared to their counterparts. Our findings showed that long-term cocaine use may exacerbate adverse effects of PI therapy on lipid metabolism, suggesting that reduced cocaine use may be considered an alternative approach to managing PI-associated dyslipidemia in chronic cocaine users with HIV infection.
Introduction
Affecting all age, gender, and racial groups in the US, 1 it is estimated that 1.1 million adults and adolescents in the US were living with HIV at the end of 2015. 2 Antiretroviral therapy (ART) introduced in the mid-1990s has significantly improved survival of people infected with HIV. 3 The life expectancy after HIV diagnosis in the US increased from 10.5 years in 1996 to 28.9 years in 2011,4,5 and half of HIV-infected people in the US were aged 50 years and older in 2015. 6 As HIV-infected people who receive ART live longer, non-AIDS chronic diseases have become common health problems in this population, 7 of which coronary artery disease (CAD) is currently a leading cause of mortality and morbidity among HIV-infected individuals. 8
Dyslipidemia is a major modifiable risk factor for CAD. 9 Mounting evidence has suggested ART regimens, particularly protease inhibitors (PIs), are associated with lipid dysregulation. 10 Laboratory and clinical studies have found that PIs may inhibit lipoprotein lipase, disrupt hydrolysis of triglyceride-rich lipoproteins, impair normal post-prandial free fatty acid and lipoprotein catabolism, and interfere with peripheral fatty acid trapping.11–13 The effects of PI-based regimens on lipid levels were stronger among African Americans than among whites. 14
Cocaine is one of the most widely used illicit drugs worldwide and in the US.15,16 It is also a highly prevalent substance used by HIV-infected people. 17 According to the 2016 National Survey on Drug Use and Health, approximately 1.9 million people over 12 years were current users of cocaine. 16 An interview among 1038 HIV-infected inpatients at public hospitals showed that 34% of the interviewees used cocaine/crack. 18 Cocaine use may not only increase the risk of HIV infection 19 but also may worsen disease progression and survival among HIV-infected people.20–22 For example, epidemiological studies have demonstrated significant associations between cocaine use and blood lipid changes.23–25 Nevertheless, very few studies examined possible modification effects of long-term cocaine use on PI-induced dyslipidemia in people with HIV infection. We have reported modification effects of chronic cocaine use on HIV/ART-associated subclinical CAD and myocardial steatosis in HIV-infected African Americans.26,27 The objective of this investigation was to assess whether cocaine use modifies the associations between PI therapy and lipid profiles in those with HIV infection, using only baseline cross-sectional data from a cohort of participants aged 21 years or older in Baltimore, Maryland, USA.
Materials and methods
Study participants
Between 2003 and 2014, 957 HIV-infected adults who did not have any evidence of clinical CAD or any symptoms believed to be related to CAD were enrolled in Baltimore, Maryland to participate in an observational study which aimed to investigate the associations of HIV infection, chronic cocaine use, antiretroviral regimens, and other risk factors with subclinical atherosclerosis. HIV infection was detected by ELISA and confirmed by Western blot test. None of the participants reported a prior history of statin use.
The study protocol was approved by the Institutional Review Board at the Johns Hopkins School of Medicine. All the participants provided the written informed consent. All the study procedures followed institutional guidelines.
Lipid profiles
Blood samples were obtained after overnight fasting. Serum was separated by centrifugation at 2500 r/min for 15 min at 4°C. Total cholesterol (TC), low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C), and triglycerides (TG) were measured with an analyzer (Hitachi 747, Roche, Englewood, NJ, USA). Ratios of TC/HDL-C and TG/HDL-C were calculated. The atherogenic index of plasma (AIP) was calculated by the formula: log(TG/HDL-C). 28 AIP is strongly correlated with lipoprotein particle size and has been considered as an important predictor of atherosclerosis and CAD. 29
According to the National Cholesterol Education Panel’s (NCEP) Adult Treatment Program-3 (ATP-III) guidelines, 30 hypercholesterolemia was defined as TC ≥200 mg/dL, high LDL-C was defined as LDL-C ≥130 mg/dL, low HDL-C was defined as HDL-C <40 mg/dL in men and <50 mg/dL in women, and hypertriglyceridemia was defined as TG ≥150 mg/dL. People with any aforementioned lipid abnormalities were considered to have dyslipidemia. High TG/HDL-C ratio was defined if the ratio ≥3.75 in men or ≥3 in women. 30 High TC/HDL-C ratio was defined if the ratio was ≥5 based on the World Health Organization criteria. 31 The 85th percentile of the pooled sample was used as the cut-off value for high HDL-C. AIP was defined as abnormal if >0.1. 29
Substance use and ART
During face-to-face interviews, participants were asked by trained research staff to answer questions on their sociodemographic characteristics, cigarette smoking and alcohol consumption, duration and frequency of cocaine and other illicit drug use, medical history, and medications including HIV regimens. Since self-reported substance use has been validated by urine and hair analysis,32,33 the information on substance use collected by a structured interview tool was used to assess drug use and chronic cocaine use. Cocaine use was defined as chronic use of cocaine by any route for at least six consecutive months and administered at least four times per month. Infrequent cocaine users (<4 times per month or <6 consecutive months) and never cocaine users were grouped as non-chronic cocaine users. Chronic cocaine users who also used other drugs, such as opiates, benzodiazepines, methamphetamine, or alcohol were included.
Self-reported medical history and medications administered were confirmed by medical chart reviews. ART regimens were categorized into three types: nucleoside reverse-transcriptase inhibitors (NRTIs), non-nucleoside reverse-transcriptase inhibitors (NNRTIs), and PIs. Durations of ART regimens were measured in months. According to its median duration, the duration of PI use was dichotomized as ≥12 months vs. <12 months.
Potential confounders
Body weight and height were measured by nurses at the clinical research unit and used to calculate body mass index (BMI, kg/m2). Serum 25(OH)D was measured using a chemiluminescence immunoassay (Diasorin Inc., Stillwater, MN, USA) and defined as deficiency if the value was <20 ng/mL. 34
Statistical analyses
Descriptive and regression analyses were conducted using SAS software (version 9.4; SAS Institute, Cary, NC, USA). Distributions of selected demographic and lifestyle characteristics were described using proportions. Medians and interquartile ranges (IQRs) were calculated for continuous variables such as age, serum 25(OH)D concentrations, BMI, and lipid profiles. All continuous variables of our interest were non-normally distributed, and thus they were compared across cocaine use subgroups using the non-parametric Kruskal-Wallis three-sample test. The categorical variables were compared by Chi square test. In our study population, the median duration of cocaine use was 15 years among chronic cocaine users. Therefore, chronic cocaine use was categorized as long-term use (≥15 years) and short-term use (<15 years).
The associations of duration of PI therapy with TC, LDL-C, HDL-C, and TG were examined using multiple linear regression models. Multiple logistic regression models were performed to examine the associations of PI therapy with hypercholesterolemia, hypertriglyceridemia, and dyslipidemia. All the models were fitted in the overall pooled sample, long-term cocaine use, short-term cocaine use, and non-chronic cocaine use subgroups, separately. Demographic and lifestyle covariates were selected as potential confounding factors in multiple linear and logistic regression models according to stratified analyses. Demographic and lifestyle covariates in the adjusted analyses included age, gender, current cigarette smoking, current alcohol use, serum 25(OH)D, BMI, duration of NRTI therapy, and duration of NNRTI therapy. All the tests were two-sided, and p < 0.05 was considered to be statistically significant.
Results
Selected characteristics by cocaine use status
Among the 957 HIV-positive participants with no history of statin use, 403 were long-term cocaine users, 62.5% were males, and 69.7% were current cigarette smokers (see Table 1). Approximately 96% of the participants were African Americans; therefore, race/ethnicity was not adjusted in the regression models. The median age was 46 (IQR: 41–51) years. The median serum 25(OH)D level was 17.0 ng/mL (IQR: 11.0–26.0 ng/mL). Long-term cocaine users were significantly more likely to have greater serum 25(OH)D concentrations and currently smoke than short-term cocaine users and non-chronic cocaine users (both p < 0.05). Gender, current alcohol consumption, BMI, and durations of ART did not significantly differ across three cocaine use subgroups (all p > 0.05).
Characteristics of study participants by cocaine use status (n = 957).a
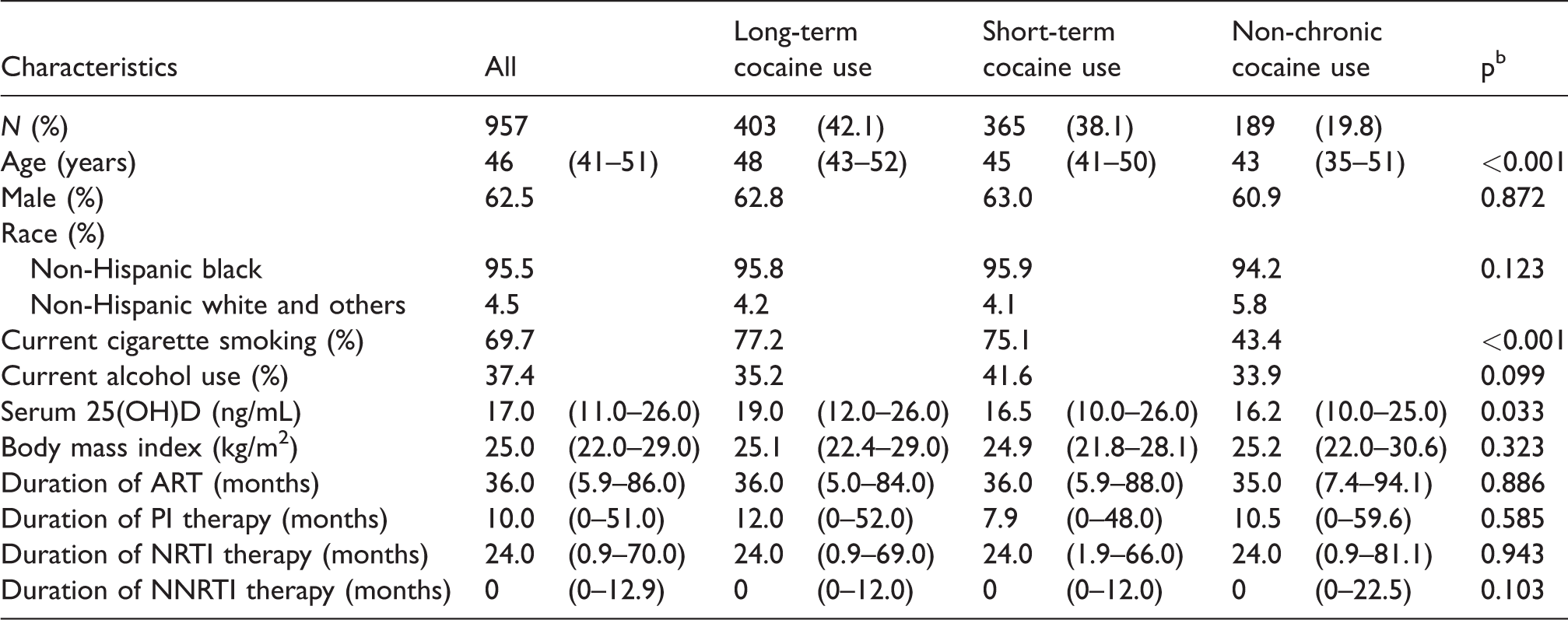
ART: antiretroviral therapy; PI: protease inhibitor; NRTI: nucleoside reverse-transcriptase inhibitor; NNRTI: non-nucleoside reverse-transcriptase inhibitor.
aMedian (interquartile range) was presented for continuous variables, and proportion (%) was presented for categorical variables.
bNon-parametric Kruskal-Wallis three-sample test was used to compare continuous variables. Chi square test was used to compare categorical variables.
Lipid profiles by cocaine use status
Lipid profiles were presented for all subjects and by cocaine use status in Table 2. The median serum TC, LDL-C, HDL-C, and TG concentrations were 160.0 mg/dL (IQR: 137.5–185.0 mg/dL), 83.5 mg/dL (IQR: 64.0–103.0 mg/dL), 49.0 mg/dL (IQR: 38.0–61.0 mg/dL), and 108.5 mg/dL (IQR: 76.0–152.5 mg/dL), respectively. As compared to long-term cocaine users, non-chronic cocaine users had statistically significantly greater TC and LDL-C concentrations (both p < 0.05). The prevalence rates of hypercholesterolemia, hypertriglyceridemia, and dyslipidemia did not significantly differ across three cocaine use subgroups (all p > 0.05).
Lipid profiles of study participants by cocaine use status.a
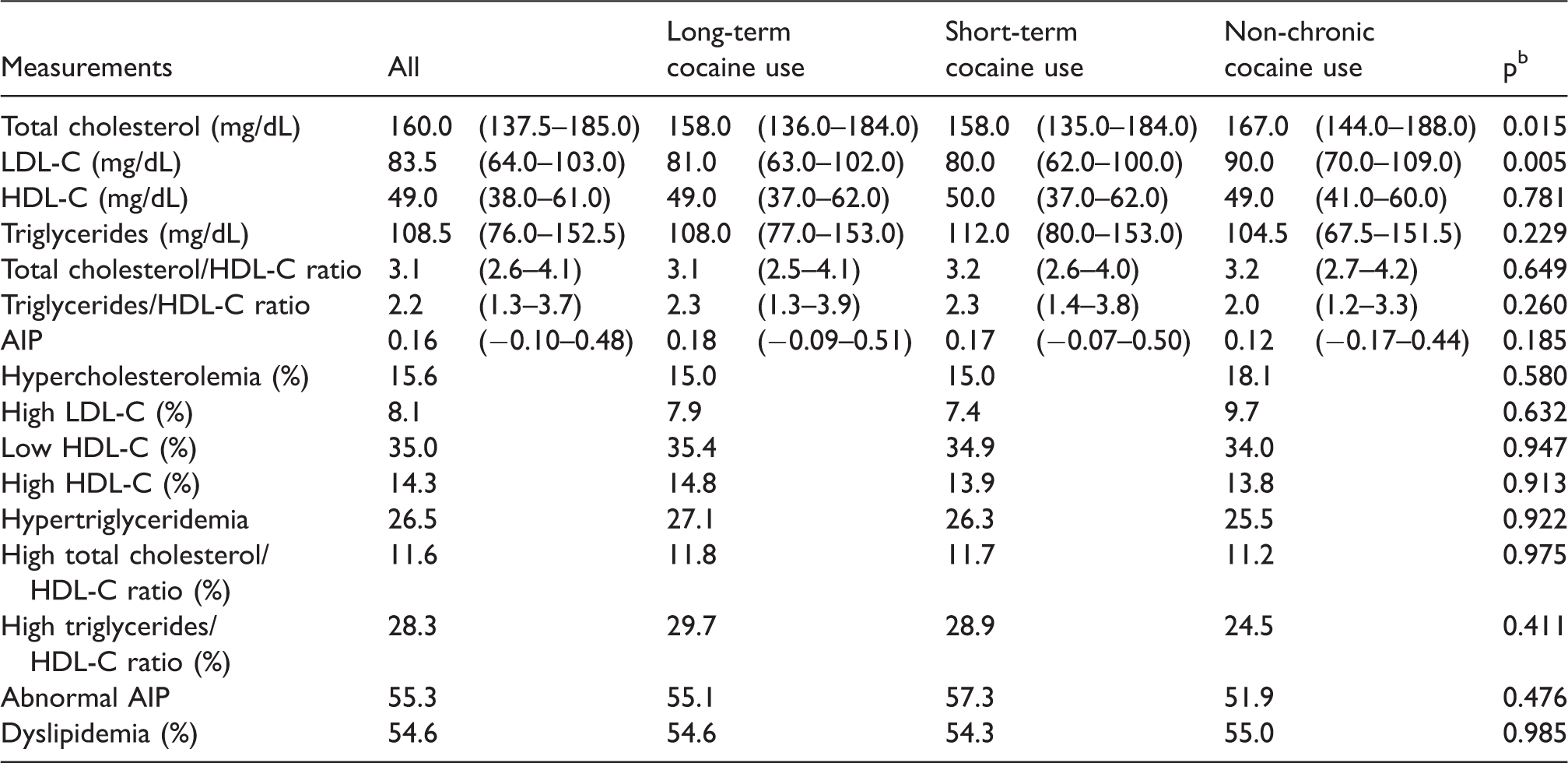
LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; AIP: atherogenic index of plasma.
aMedian (interquartile range) was presented for continuous variables, and proportion (%) was presented for categorical variables.
bNon-parametric Kruskal-Wallis three-sample test was used to compare continuous variables. Chi square test was used to compare categorical variables.
The associations between duration of PI therapy and lipid profiles, stratified by cocaine use status
The associations between duration of PI therapy and lipid measurements are presented in Tables 3 and 4. After controlling for various covariates (see Table 3), TC concentrations were significantly associated with the lengths of PI therapy (in months) in the overall sample (β = 0.072, SE = 0.033, p < 0.05). According to the stratified analyses, TC, LDL-C, TC/HDL-C ratio, and AIP levels were positively associated with duration of PI-based therapy in long-term cocaine users (β = 0.141, SE = 0.061, p < 0.05 for TC; β = 0.121, SE = 0.050, p < 0.05 for LDL-C; β = 0.006, SE = 0.002, p < 0.05 for TC/HDL-C ratio; and β = 0.002, SE = 0.001, p < 0.05 for AIP). However, none of the lipid measurements was associated with PI therapy in the subgroup of short-term cocaine users, and furthermore, longer-term PI therapy was significantly associated with increased HDL-C in non-chronic cocaine users (β = 0.109, SE = 0.042, p < 0.05).
Linear regressions for the associations between duration of protease inhibitor (PI) therapy (months) and lipid profiles by cocaine use status.
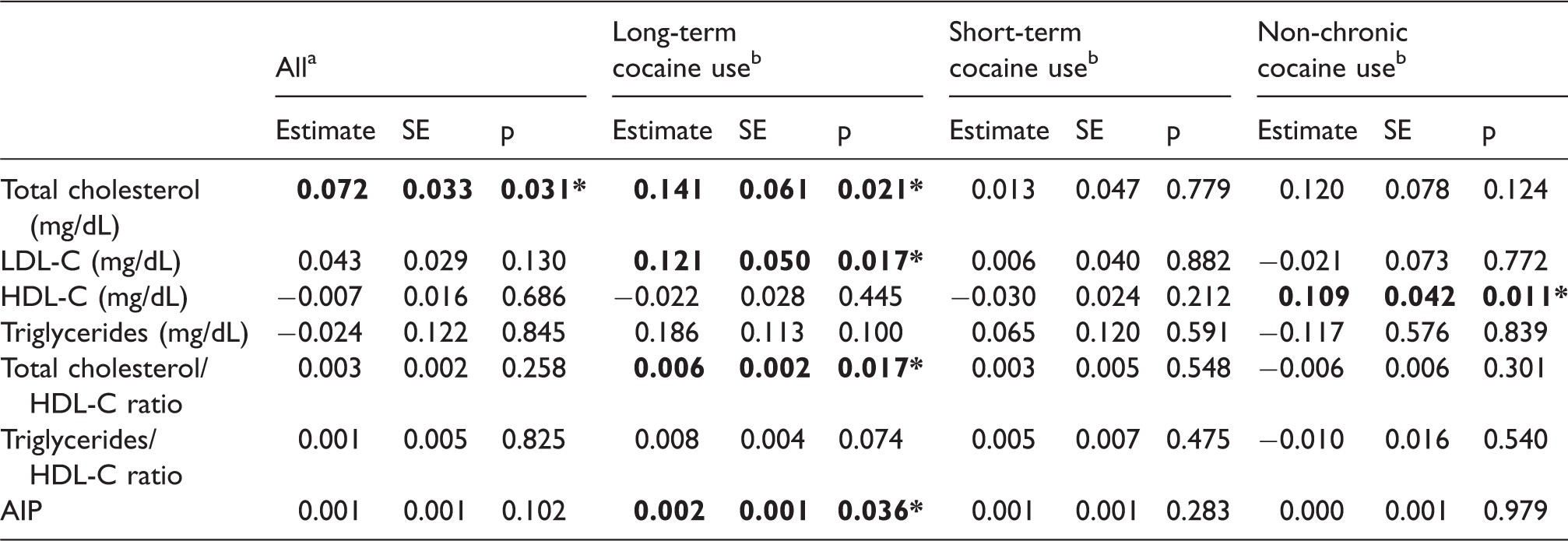
LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; AIP: atherogenic index of plasma.
aLinear regression models were adjusted for age, gender, cigarette smoking, alcohol use, cocaine use, serum 25(OH)D, BMI, duration of NRTI therapy, and duration of NNRTI therapy.
bLinear regression models were adjusted for age, gender, cigarette smoking, alcohol use, serum 25(OH)D, BMI, duration of NRTI therapy, and duration of NNRTI therapy.
*p<0.05.
Logistic regressions for the associations between duration of protease inhibitor (PI) therapy (≥12 months vs. <12 months) and lipid profiles by cocaine use status.

LDL-C: low-density lipoprotein cholesterol; HDL-C: high-density lipoprotein cholesterol; OR: odds ratio; CI: confidence interval.
aLogistic regression models were adjusted for age, gender, cigarette smoking, alcohol use, cocaine use, vitamin D deficiency, BMI, duration of NRTI therapy, and duration of NNRTI therapy. Study participants with PI therapy <12 months were the reference group.
bLogistic regression models were adjusted for age, gender, cigarette smoking, alcohol use, vitamin D deficiency, BMI, duration of NRTI therapy, and duration of NNRTI therapy. Study participants with PI therapy <12 months were the reference group.
*p<0.05, **p<0.01.
According to logistic regression models, PI therapy was significantly associated with increased risk of hypertriglyceridemia (unadjusted OR = 1.86, 95% CI = 1.39, 2.49; adjusted OR = 1.90, 95% CI = 1.35, 2.69) and abnormal AIP (unadjusted OR = 1.39, 95% CI = 1.08, 1.80; adjusted OR = 1.39, 95% CI = 1.02, 1.90) in the overall sample (see Table 4). ORs of other covariates were presented for selected lipid profiles in the supplementary table (Supplementary Table 1). The participants who were exposed to PI regimens longer than 12 months and used cocaine greater than 15 years were more likely to have hypertriglyceridemia (unadjusted OR = 2.18, 95% CI = 1.39,3.42; adjusted OR = 2.82, 95% CI = 1.63, 4.88) and abnormal AIP (unadjusted OR = 1.46, 95% CI = 0.98,2.17; adjusted OR = 1.73, 95% CI = 1.08,2.79). Significant associations between PI therapy ≥12 months and high HDL-C were detected in those who had not used cocaine chronically (unadjusted OR = 2.10, 95% CI = 0.90, 4.92; adjusted OR = 3.35, 95% CI = 1.10, 10.18) but not in those with short-term cocaine use.
Discussion
To our knowledge, this is the first study to examine whether long-term cocaine use exacerbated the PI-induced dyslipidemia in individuals with HIV infection. We found that (1) duration of PI-based therapy was positively associated with TC, LDL-C, TC/HDL-C ratio, and AIP levels in long-term cocaine users and was also positively associated with HDL-C concentrations solely in non-chronic cocaine users (all p < 0.05); (2) long-term cocaine users who were on long-term PI-based therapy were more likely to have hypertriglyceridemia and abnormal AIP, while non-chronic cocaine users who received PI therapy longer than 12 months were less likely to have suboptimal HDL-C levels (all p < 0.05); and (3) none of the lipid measurements was significantly associated with the duration of PI therapy in short-term cocaine users (all p > 0.05).
The mechanisms of PI-associated dyslipidemia have not yet been fully understood. PI regimens have high affinity for the catalytic site of HIV-1 protease enzyme. 10 The latter is homologous with regions of cytoplasmic retinoic-acid binding protein type 1 (CRABP-1) and low-density lipoprotein-receptor-related protein type 1 (LRP1).10,35 CRABP-1 and LRP1 are two human proteins that regulate lipid metabolism. PI regimens may bind to CRABP-1 and LRP1 and result in dyslipidemia by decreasing differentiation of peripheral adipocytes, reducing triglyceride storage, increasing lipid release, and inhibiting hepatic uptake of chylomicrons.36,37 It was also hypothesized that PI may inhibit mitochondrial protease processing, impair mitochondrial function, and induce lipodystrophy syndrome. 38
Our data indicated that HIV-infected people with long-term duration of PI use were at significantly increased risks for abnormal TC levels and hypertriglyceridemia. Biomedical and clinical studies have provided compelling evidence for the adverse effects of PI-based regimens on lipid metabolism. Our findings were consistent with those of previous studies. A randomized trial among 422 ART-naïve patients observed significant increases in TC and LDL-C levels after the patients received a PI regimen (p < 0.05). 39 A recent systematic review based on 88 studies published in peer-reviewed journals reported that PI use for a long time (e.g. ≥1 year) was associated with hypertriglyceridemia, elevated LDL-C levels, and accumulation of apolipoprotein E and apolipoprotein CIII-containing lipoproteins. 40
A major finding of this investigation was that the aforementioned PI-associated lipid dysregulations predominantly affected those with long-term cocaine use but not short-term or non-chronic cocaine users. Higher HDL-C levels were significantly associated with the duration of PI therapy in non-chronic cocaine users, but not in chronic cocaine users. We also found that the participants with long-term PI therapy and long-term cocaine use were more likely to have abnormal AIP. AIP strongly correlates with cholesterol esterification rates in apoB-lipoprotein-depleted plasma and lipoprotein particle size. 28 It is considered as a significant predictor of atherosclerosis and CAD. 41 The results derived from this investigation were consistent with our recently published findings, which have reported that cocaine use may aggravate ART-associated coronary stenosis and PI-associated myocardial steatosis.26,27 All these observations suggested that the adverse effects of long-term PI-based regimens on lipid metabolism may be exacerbated by chronic cocaine use, while reduced cocaine use may minimize such adverse effects or even promote cardioprotective effects of PI therapy by increasing HDL-C levels in those with HIV infection.
Biomedical and epidemiological studies have suggested that chronic cocaine use may alter blood lipid profiles.25,42,43 However, the mechanisms underlying the modification effects of chronic cocaine use on the relationships between PI therapy and dyslipidemia remain unclear. Animal studies showed that cocaine given chronically in the diet increased total lipids and triglycerides-rich pre-beta lipoprotein levels in the blood. 43 Gettler 42 reported significant hypocholesterolemia among cocaine abusers admitted to an inner city hospital. A recent study indicated that cocaine-dependent individuals had significantly higher TG levels compared to their normal counterparts. 25 PI regimens are primarily metabolized by the hepatic cytochrome P450 (CYP) enzymes including CYP3A enzymes. 17 CYP3A enzymes are also involved in cocaine metabolism. 44 It has been hypothesized that cocaine and PI regimens may interfere with each other via the CYP3A pathway, and result in adverse cocaine-PI interactions and toxic effects. 45
Despite a positive association between HDL-C levels and PI use in our non-chronic cocaine users, existing research on the effects of PI therapy on HDL-C concentrations has been inconclusive. A cross-sectional study found that HIV-infected patients with PI therapy had significantly lower HDL-C levels than PI-naïve patients and healthy men. 46 The multicenter AIDS Cohort Study reported that receiving PI therapy significantly increased TC and LDL-C levels except for HDL-C levels. 47 Such discrepancies across studies may be due to (1) differences in PI-based regimens that were examined 40 and (2) not accounting for substance use (e.g. cocaine use) and its potential modification effects. Future research, such as large-scale longitudinal studies and long-term clinical trials, is needed to confirm our results and examine the underlying mechanisms.
This study has several limitations. First, due to the cross-sectional nature of the data, we could not investigate longitudinal relationships of cocaine use and PI therapy with changes in lipid profiles. Therefore, causal relationships cannot be established based on our present findings, and longitudinal studies are needed to confirm our findings. Second, evidence has shown that increased intake of saturated fat and physical inactivity are related to dyslipidemia.48,49 Unfortunately, we did not collect data on participants’ usual dietary intake and physical activity. Since body weight status was highly correlated with unhealthy diet and physical inactivity,50,51 BMI was adjusted for in all the regression models instead. Third, all the participants resided in Baltimore city and some of them may use multiple drugs. Potential confounding effects of other illicit drugs were tested in our models, and none of them was statistically significant. Fourth, information on participants’ medications including HIV regimens was collected by face-to-face interviews. Although self-reported ART use was validated by medical chart review, there was no measure of adherence. The exact amounts of ART regimens taken by the participants remained unclear. Fifth, the participants’ drug use was self-reported in this study. Thus, the never use of cocaine cannot be validated. There was a lack of a structured interview to infer cocaine addiction from drug use in the past month. To solve this problem, we examined the impact of durations of cocaine use instead of cocaine addiction in this study. Lastly, multiple statistical tests were conducted in the study and provided a few significant results. Our study was exploratory not confirmatory. Therefore, we did not conduct adjustments for multiple comparisons to avoid additional problems that “p-value correction” may cause.52,53 Some researchers advocated to interpret the magnitude of the effect sizes rather than p-values alone. 52 The OR is a widely used measure of effect size in epidemiological studies. According to Chen et al.’s 54 computation, an OR of 2.50 was equivalent to Cohen’s d = 0.5 (medium) for a disease with a prevalence of 10%, suggesting at least some moderate associations between PI use, HDL, and hypertriglyceridemia observed in our study.
Conclusion
Despite the fact that long-term PI exposure has been reported to be associated with elevated TC, LDL-C, and hypertriglyceridemia, this study provided evidence that long-term cocaine use may exacerbate PI-associated adverse effects on lipid metabolism in chronic cocaine users with HIV infection. Longitudinal studies and clinical trials are warranted to confirm our findings. Furthermore, since our recent studies have revealed that cocaine abstinence/reduced use led to lowered endothelial dysfunction and even coronary plaque regression,21,55 given the high prevalence of cocaine use in HIV-infected people and low statin adherence in substance users,17,56 reduced cocaine use should be considered an alternative to statins or novel ART drugs in the management of PI-associated dyslipidemia in HIV-infected chronic cocaine users.
Supplemental Material
Supplemental material for Impact of cocaine use on protease inhibitor-associated dyslipidemia in HIV-infected adults
Supplemental material for Impact of cocaine use on protease inhibitor-associated dyslipidemia in HIV-infected adults by Ji Li, Hong Lai, Shaoguang Chen and Shenghan Lai in International Journal of STD & AIDS
Footnotes
Acknowledgements
We thank staff and participants of the study for their contributions. We also thank the anonymous referees for their comments and suggestions to help improve the manuscript. The funding source had no role in the design and conduct of the study; management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision about the manuscript for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grant U01DA040325 from the National Institute on Drug Abuse, National Institutes of Health.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.