
Abstract
This study aimed to identify factors associated with repeat syphilis infection in North East England, in order to inform local prevention and control opportunities. We undertook a case–case study comparing individuals diagnosed with single or multiple episodes of syphilis infection within genitourinary medicine (GUM) clinics in NE England (12 clinics serving a population of 2.5 million). Study cases were verified as having had true re-infection by a GUM clinician (using serological and/or clinical parameters) and control cases (3 per case) frequency matched to cases by age and year of presentation. The odds of exposure to sexual behavioural and clinical factors were compared for cases and control cases using stepwise multivariable logistic regression. We included 66 cases and 235 control cases. The majority of cases (62/66) and control cases (165/235) were men who had sex with men (MSM). Data were missing for 0–64% of cases across different variables. Following multivariable analysis HIV seropositivity (OR 23.3, 95% CI 4.32–125.9), failure to attend follow-up (OR 4.63, 95% CI 1.11–19.31), stage of infection and deprivation were associated with re-infection (p < 0.001). In this study, HIV seropositivity and failure to attend follow-up were associated with re-infection with syphilis. Actions targeted at these groups may help to reduce ongoing transmission.
Keywords
Introduction
A recent increasing trend in syphilis diagnoses has been reported in Europe 1 and other parts of the world with less notable increases in other sexually transmitted infections (STIs). 2 In England, the incidence of syphilis amongst individuals accessing sexual health services increased from 5.0 per 100,000 in 2010 to 8.1 per 100,000 in 2014, 3 and white men who have sex with men (MSM) appeared to be disproportionately affected. 3 Repeat infection with STIs is thought likely to contribute to persistence of infection within a population. 4 A number of studies suggest that those with repeat syphilis infection may represent a high-risk, core group of individuals who are at ongoing risk of infection and transmission to others.5–7
Although previous studies have attempted to look at factors associated with a repeat diagnosis of syphilis, cross study comparisons are limited by variations in demographics and behaviours amongst different population groups. The epidemiology of STIs is complex with multiple factors such as changes in disease prevalence, sexual behaviours, configuration and access to services influencing observed trends. 4 Regular assessment of surveillance data is therefore important in continually informing control measures. 4 Enhanced surveillance of syphilis was established in the North East of England (NEESS) in 2002, with the aim of developing further understanding of the epidemiology of infection amongst specific behavioural risk groups. There are 12 Genitourinary Medicine (GUM) clinics serving a population of approximately 2.5 million, which report newly-diagnosed episodes of infection to this system. In addition, GUM clinics report all new diagnoses of syphilis to a national patient-level electronic dataset. Since, 2008 this dataset (Genitourinary Medicine Clinic Activity Dataset – GUMCAD) contains anonymised individual returns, but prior to 2008 only aggregated returns were available. Previous (unpublished) analysis of these data suggests that the majority of diagnoses of syphilis made amongst residents of North East England were made at a GUM clinic in North East England and that these data are therefore likely to provide a representative sample of syphilis diagnoses in the area. The number of episodes of syphilis reported to NEESS increased from 102 in 2003 to 172 in 2014 and crude analysis suggested that approximately 5% of individuals with syphilis infection reported between 2002 and 2014 had more than one episode of syphilis infection during this period. The aim of this study was to identify factors (present at the time of initial diagnosis) that are associated with repeat diagnosis of syphilis, in order to target appropriate control measures and reduce the burden of infection in the North East (NE) of England.
Methods
A pseudoanonymised dataset of all episodes of syphilis infection that presented between 1 January 2002 and 31 December 2014 was extracted from NEESS. In order to maximise data completeness, episodes of syphilis with a date of presentation on or after 1 January 2008 were matched to those reported to the GUMCAD dataset (SHHAPT a codes A1-A6), using the unique GUM clinic number. b Any previously unidentified episodes were added to NEESS.
Research & Development management approval for participation in this study was sought from six acute Trusts covering all 12 GUM clinics in North East England. A retrospective case–case study design was applied. Cases were defined as any individual aged 18 years or more, referred to NEESS from a participating GUM clinic with more than one episode of syphilis infection (any stage of infection) between 1 January 2002 and 31 December 2014. Repeat episodes were identified separately using three different sets of criteria for exact matching (i) GUM clinic number and date of birth (DOB), (ii) Soundex number c and DOB, (iii) gender, ethnicity and DOB. Cases from the third category were reviewed and included if the GUM clinic number and/or Soundex number were similar (taking into account the possibility for typographical errors). Control cases were defined as any individual, aged 18 years or over, referred to NEESS from a participating GUM clinic with only one recorded episode of infection (any stage of infection) between 1 January 2002 and 31 December 2014. Any control cases with a recorded history of previous syphilis infection (part of the NEESS dataset) were excluded.
Rothman’s Episheet 8 for case-control studies uses an estimated exposure prevalence, odds ratio (OR) and number of cases to estimate a required sample size. Preliminary analysis of NEESS data indicated that approximately 60 cases of re-infection would be identified, the majority of which were likely to be MSM. Paz-Bailey et al. 9 estimated that 13% of HIV-positive aware MSM, 12% of those that were HIV-negative and 33% of those that were HIV-positive but unaware, engaged in unprotected anal sex, respectively. There is reportedly a high prevalence of HIV co-infection amongst those with syphilis with estimates ranging from 13% to 17%5,7,10 and higher in groups such as MSM.6,11 Assuming that those who are HIV-positive but unaware are likely to be most representative of those with more risky sexual practices and perhaps therefore those at risk of repeat infection with syphilis, the prevalence of unprotected anal sex in this group was used as a proxy estimate of the prevalence of exposure to sexual behavioural factors for this study. At least two controls per case were required in order to have approximately 80% power with which to detect an OR of three. Given that the sample size was likely to be further reduced by stratification of data on analysis, three control cases per case were selected.
Control cases were frequency matched to cases by year of diagnosis at first episode of infection (calculated using the date of presentation recorded in NEESS or where this was missing, the date on which the surveillance form was completed) and 10-year age grouping (18–27, 28–37, 38–47 and 48–57 years). Only adult (≥18 years of age) cases and control cases were included since one of the main exposures of interest was sexual behaviour. A random sub-sample of three control cases per case was selected within each year and age-group category.
Exposure information reported to NEESS at the time of the first recorded episode was extracted into an Excel data sheet. Exposure variables included age at attendance, gender, ethnicity, deprivation (defined by index of multiple deprivation [IMD] quintile based on lower super output area [LSOA] of residence) and rural urban status (defined by RUC classification based on LSOA of residence), behavioural factors (sexual orientation, contact meeting place [e.g. bar/internet], any concurrent STI, number of sexual partners in the three and 12 months prior to presentation), and clinical factors (stage of infection, diagnosing clinic, date of presentation). Exposure information was verified by a lead clinician in the diagnosing GUM clinic using the clinical case notes and where available, missing data were updated. Additional exposure variables were also extracted from the clinical notes including: behavioural factors (type of sex, recreational drug use) and clinical factors (hepatitis B and C status, number of follow-up clinics scheduled and attended, and treatment regimen). Episodes were excluded if no exposure information could be identified. Cases were verified by lead clinicians and excluded if clinical parameters including quantitative changes in treponemal antibody titres (in accordance with guidance from the British Association for Sexual Health and HIV [BASHH]), 12 clinical history and examination findings suggested they were unlikely to represent true re-infection. Where episodes of infection were reported at more than one GUM clinic, lead clinicians at each clinic liaised with each other in order to verify cases.
All exposure variables were categorised into two or more mutually exclusive categories as appropriate and analysed as discrete variables. A priori confounding variables included gender, sexual orientation, IMD, HIV status and stage of infection.
Data were analysed using STATA 13.1. The prevalence of exposure to each variable of interest at the time of the first known episode of syphilis was compared amongst cases and control cases using univariate logistic regression, and expressed as an OR with 95% confidence intervals (CIs). Where effect sizes were inestimable due to zero counts, median unbiased estimates were calculated using exact logistic regression.
Stepwise multivariable logistic regression was used to further analyse the associations. Matched variables were included as covariates and pre-defined confounding variables or those variables which on univariate analysis had a positive effect (given the aim of identifying factors associated with infection) and a statistical association of p < 0.2. Variables were entered into the model in stages given the relatively large number of parameters estimated. The following criteria were used to define each stage; (i) p value <0.1, OR >2 and missing values <10%, (ii) p value <0.2, missing values <20%, and (iii) all remaining variables. Backward selection was carried out at each stage removing variables one by one (in order of p value) which were not confounding (did not change the adjusted OR of another variable by >20%) or associated with the outcome (p < 0.2 as determined by the likelihood ratio test), prior to entering the next group of variables. Linearity of age was checked using quadratic and cubic functions.
Results
A total of 1794 episodes of infection were identified from the NEESS and a further 188 episodes identified from GUMCAD (Figure 1). Approval was not obtained to participate in the study from one acute Trust and episodes of infection diagnosed in three GUM clinics were subsequently excluded. Eighty-seven cases (192 episodes of infection) were identified in the remaining dataset and 261 control cases selected. Following verification at GUM clinics, 61 case episodes and 26 control case episodes were excluded (Figure 1). Sixty-six cases and 235 control cases were included in the final analysis. The median duration of follow up was 7.9 years (interquartile range [IQR] 4.9–10.1 years) for cases and 7.9 years (IQR 4.7–10.2 years) for control cases.
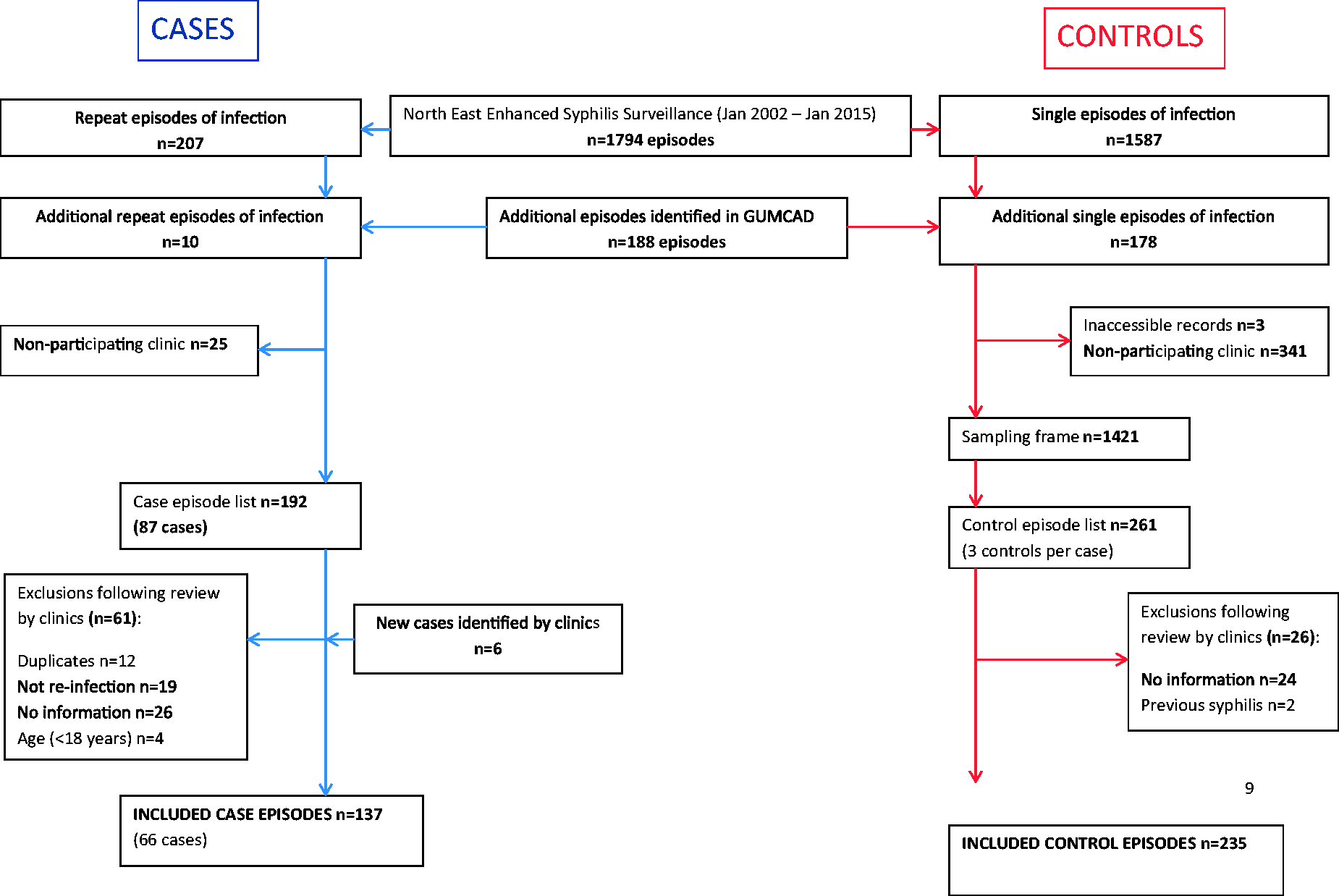
Selection of cases and control cases.
Sixty-one of the 66 cases had two recorded episodes of infection. The remaining five cases had three episodes. Time to first reinfection ranged from six months to 10 years (median 2.4 years, IQR 1.3–3.9 years). The prevalence of re-infection (defining the denominator from the complete uncleaned dataset i.e. the total number of control episodes [n = 1421] and cases [n = 87] identified prior to frequency matching and verification) was estimated to be 4% (66/1508).
The study population consisted primarily of white British (240/301) males (269/301). Just under half of the study population (128/301) were less than 28 years of age and three quarters (227/301) were MSM (homosexual or bisexual). Eighty percent (238/301) lived within an urban as opposed to a rural area. HIV status was recorded for most cases and control cases (281/301) and where recorded the majority (244/281) were seronegative. Completeness of data for other exposure variables varied from 36% to 100%.
Results of univariate logistic regression are shown in Tables 1 to 3. Being male (OR 9.9, 95% CI 1.32–73.78), homosexual (OR 6.16, 95% CI 2.14–17.71), bisexual (OR 9.63, 95% CI 2.76–33.51) or HIV seropositive (OR 4.47, 95% CI 2.15–9.29) was significantly (p < 0.05) associated with reinfection. Exposure to unprotected anal insertive sex (OR 2.35, 95% CI 1.16–4.78), meeting partners at a cruising venue (OR 2.40, 95% CI 1.13–5.49) reporting more than 20 sexual partners in the 12 months prior to diagnosis (OR 4.62, 95% CI 1.73–12.32) and failure to attend one or more follow-up appointments (OR 2.53, 95% CI 1.02-6.26) were also significantly associated (p < 0.05) with re-infection, although there was no clearly discernible trend with numbers of sexual partners.
Association between demographic characteristics and syphilis re-infection for individuals referred to the North East Enhanced Syphilis Surveillance System (NEESS), 1 January 2002–31 December 2014.
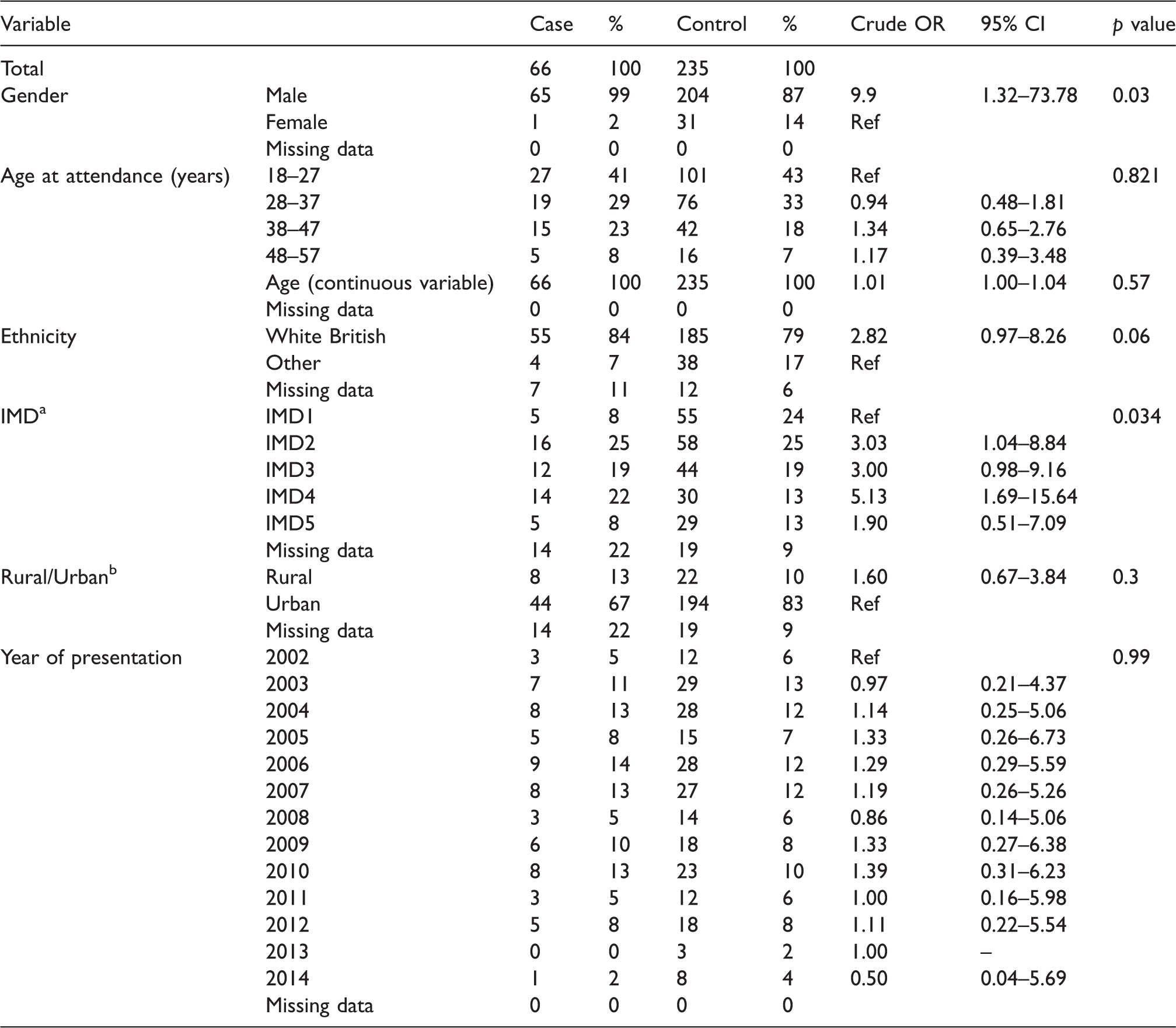
IMD: index of multiple deprivation; ONS: Office for National Statistics.
a2011 index of multiple deprivation within region quintiles (1 = most deprived, 5 = least deprived).
bONS 2011 rural urban classification based on lower super output area of residence (‘urban’ output areas defined as those in which the majority of the population live in a physical settlement with a population of 10,000 or more).
Association between sexual behaviours reported at the time of diagnosis and syphilis re-infection for individuals referred to the North East Enhanced Syphilis Surveillance System (NEESS), 1 January 2002–31 December 2014.

HBV: hepatitis B virus; HCV: hepatitis C virus; STI: sexually transmitted infection.
aMedian unbiased estimate calculated using exact logistic regression.
Association between clinical factors and syphilis re-infection for individuals referred to the North East Enhanced Syphilis Surveillance System (NEESS), 1 January 2002–31 December 2014.

aSix of the 10 clinics had fewer than 20 cases and/or control cases and were therefore categorised together (clinic 0) and compared with the remaining four clinics.
A total of 14 variables were included in the multivariable analysis; 11 variables (gender, ethnicity, deprivation [IMD], sexual orientation, oral sex, anal insertive sex, HIV status, number of sexual partners in the 3 months prior to diagnosis, meeting partners at a cruising venue, stage of infection, non-attendance at one or more follow-up clinic [DNA]) identified from the univariate analysis (OR >1, p < 0.2), diagnosing clinic and the two matching factors (age and year of presentation). Five variables were included in the final model (deprivation [IMD], HIV status, DNA, stage of infection and presentation year). Adjusted ORs for four of these remained statistically significant (p < 0.05), three of which had a positive association with repeat infection (Table 4). The remaining variable (presentation year) had a non-significant association (p = 0.5)
Association between demographic and clinical exposures and syphilis re-infection for individuals referred to the North East Enhanced Syphilis Surveillance System (NEESS), 1 January 2002–31 December 2014, following stepwise multivariable logistic regression.
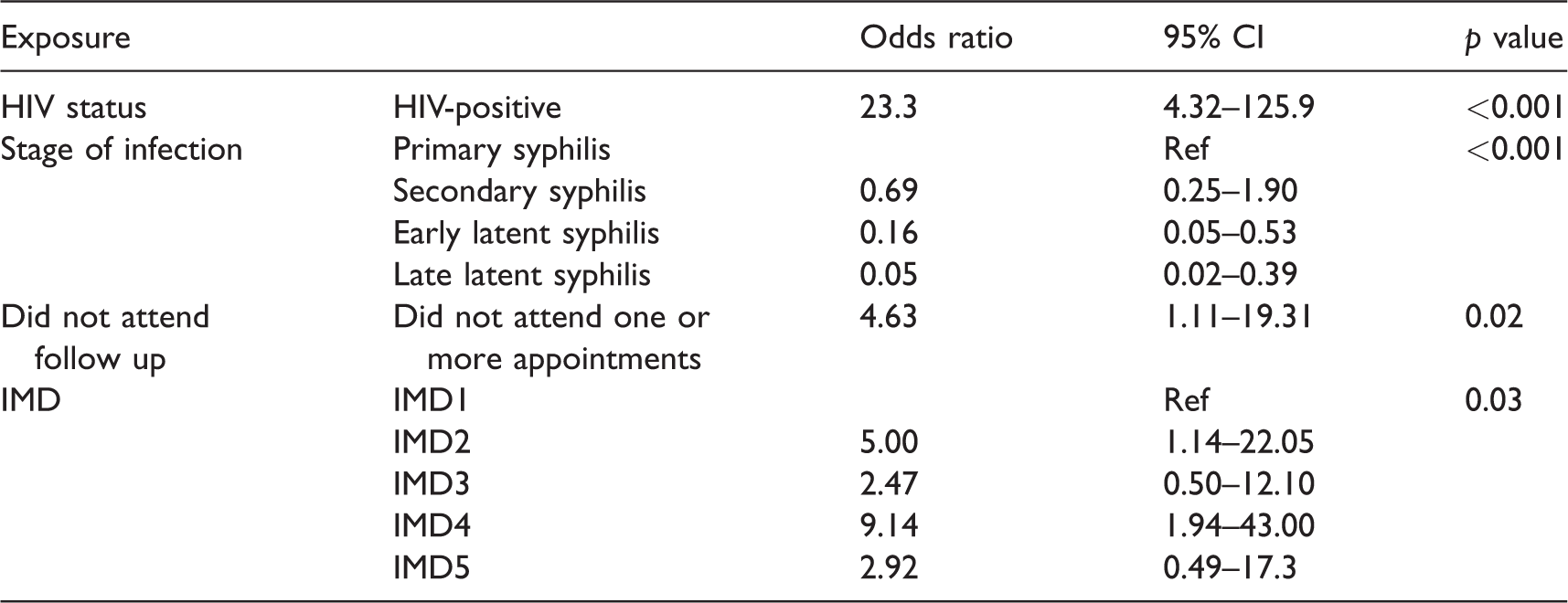
IMD: index of multiple deprivation.
Discussion
Recent efforts to control syphilis appear to have had limited success given the observed increase in cases. Repeat syphilis infection is an emerging issue which may contribute to ongoing transmission. A number of other studies have considered factors associated with repeat diagnosis of syphilis, primarily conducted in America and Canada.6,7,13,11,14 In this study, the population consisted mostly of young, white MSM, which is consistent with the findings of others 15 and the demographics of syphilis cases in the UK. The estimated proportion of cases with re-infection (crude average 5.9 years follow-up per individual) was 4% and is in keeping with estimates from other studies (2.5% to 12%).6,7,13,11,14 A number of variables were associated with re-infection but following multivariable analysis only three had a significant positive association, the strongest of which was for HIV seropositivity.
An association between HIV seropositivity and re-infection has consistently been found.6,7,13,11,14 Associations with other sexual behaviour factors such as the number of sexual partners7,11 and a history of other STIs 7 have also been demonstrated although less consistently described with some studies suggesting no association. 14 This inconsistency may in part be due to difficulties in obtaining complete exposure information regarding sexual practices or differences in sexual behaviours amongst different population groups. Comparisons across studies are further compounded by reliance upon serological outcomes to define re-infection and treatment failure. 16 It is nevertheless notable that the association with HIV seropositivity remains despite the fact that NE England is considered to have a relatively low prevalence of HIV infection (0.65 per 1000 population) in comparison to the United Kingdom as a whole (1.36 per 1000 population). 17 Surveillance data suggest that sex between men is the most probable route of HIV infection in NE England 17 and there may be an ongoing risk of transmission of both HIV and syphilis in this group.
The association between HIV infection at the time of diagnosis and repeat syphilis might be explained either by a true increase in prevalence amongst those who are HIV seropositive, or as a result of differences in sexual practices, susceptibility to infection (perhaps as a result of underlying immunocompromise), or differences in testing practices. There is some evidence that syphilis may facilitate both transmission and acquisition of HIV infection, 18 but it is less clear from existing literature whether the reverse is true. Some authors have suggested that receipt of highly active antiretroviral treatment (HAART) following diagnosis of HIV infection is associated with acquisition of syphilis and that this may in part be due to immune modulation, but further evidence is required. 2 In this study, data were not collected about immunocompromise and therefore it was not possible to explore this hypothesis further.
British HIV Association (BHIVA) guidelines suggest that syphilis serology should be documented at baseline in all HIV-positive individuals and at three-monthly intervals if there are risk factors for acquisition, e.g. frequent partner change. 19 Testing and detection of infection may therefore be more frequent amongst those most at risk of repeat infection who are HIV-positive. Indeed, Malek et al. 20 estimated that re-infection rates for gonorrhoea and Chlamydia (two of the most commonly diagnosed bacterial STIs) are higher in HIV-positive MSM when compared with HIV-negative/undiagnosed MSM, which might in part be explained by differences in testing. 20 In this analysis there was an association between re-infection and not attending follow-up which suggests that more frequent testing may be a less likely explanation. Malek et al. 20 also estimated that a higher proportion of syphilis diagnoses in MSM in the UK occur amongst HIV-infected MSM when compared with other STIs which suggests that factors other than differences in testing practices may be at play. It was not possible to determine the reason for non-attendance from the data analysed in this study and whether or not it might reflect differences in risk perception of affected individuals or service provision. The provision of sexual health services in the UK has changed considerably over the last 20 years and an increasing proportion of STI-related care may be provided by non-specialist services. Care for HIV-infected individuals may be provided either in a GUM clinic or a dedicated HIV and infectious diseases unit and it is possible that testing practices for other STIs may vary between different providers. It is therefore important to fully understand the referral pathway, testing and follow-up practices in this group in order to further interpret the potential effect of any differences in screening practices.
Previous studies have suggested that those with syphilis infection and particularly HIV and syphilis coinfection may exhibit different sexual practices which pre-dispose them to infection. One study, for example, described a high frequency of unprotected anal sex when compared to those without syphilis infection. 21 A statistically significant positive association with unprotected anal insertive sex was noted in the univariate analysis of this study and may reflect differences in behaviours amongst those at risk of re-infection with syphilis, although this association did not remain following multivariable analysis. HIV status may act as a marker for certain sexual practices confounding the association between sexual practices and syphilis re-infection. Indeed, there is suggestion that some HIV-positive MSM may engage in serosorting, 22 having unprotected sex with other HIV-positive MSM where they feel there is no further risk of transmission of HIV. There are also beliefs that the risk of HIV transmission may be altered by ‘strategic positioning’ of partners (i.e. participating in insertive as opposed to receptive unprotected anal intercourse with the intention of reducing the risk of HIV infection) 23 perhaps influencing differences in sexual practices. Some have suggested that recent upsurges in STI diagnoses may be attributed to such seroadaptive behaviours and that changes in community factors such as use of internet apps where HIV status can be readily disclosed may facilitate this. 24 This would not however explain the apparent disproportionate increase in syphilis when compared with other STIs. Unfortunately, in this study, data for many of the variables concerning sexual practices and meeting venues were relatively incomplete and information was not captured about app use, limiting the ability to explore this further. This is nevertheless an important area and methods of increasing data completeness should be considered. Questions regarding social media/app use have also since been added to NEESS.
There are a number of limitations to this study. It is possible that individuals may have had episodes of infection out-with the study period, although attempts were made to control for any differential effect of this by matching cases and control cases by duration of follow-up. Cases may not have been reported to NEESS and attempts were made to control for this by matching data with the national dataset. The number of additional episodes identified was small (188 episodes between, 2008 and 2014) suggesting that NEESS data are largely complete. Individuals may also have presented to clinics outside NE England although previous (unpublished) analyses of surveillance data suggest that the number of diagnoses made at GUM clinics outside the region is small (3/187 cases diagnosed in 2013) and so it is likely that NEESS data are representative of diagnoses in NE England. Given the need for clinical interpretation in defining re-infection there is a risk of misclassification which may result in under or over estimation of cases. Attempts to minimise this were made by referring to one lead clinician in each clinic to verify cases although this was done retrospectively and may be limited by the quality of data recorded in clinical records. Some individuals may provide different demographic details at each clinic visit, limiting the ability with which to detect repeat diagnoses, although this is difficult to control for. Recall bias may have occurred for reported exposures, but there is no reason to believe that this would result in a differential bias between cases and control cases. Data regarding specific sexual practices and meeting venues were relatively incomplete limiting the power with which to detect any association with repeat infection. This may reflect difficulties in recalling such exposures or a reluctance to disclose information and methods to improve ascertainment should be considered in future studies. There may also be some over or under estimation of exposure due to exclusion of episodes for which there was no available information or repeat episodes which were thought unlikely to represent re-infection. There was a higher proportion of cases that were MSM when compared with controls. This may indicate a difference in engagement with services and hence likelihood of diagnosis with re-infection but is controlled for to some extent by the inclusion of sexuality as a potential confounding variable.
Conclusion
Syphilis infection in the North East of England primarily affects young, white MSM and there is a strong association between HIV seropositivity and repeat syphilis infection. Failure to attend follow-up was significantly associated (p = 0.02) with repeat infection even when adjusted for HIV seropositivity and the reasons underpinning this should be further explored. There is some suggestion that sexual practices may differ amongst those with repeat infection although no statistically significant associations (p < 0.2) were demonstrated following multivariable analysis. Data regarding sexual behaviours were relatively incomplete and methods to improve capture of such information should also be considered in order to help target future control measures.
Footnotes
Acknowledgements
The authors thank Dr Babiker Elawad, Consultant in Genitourinary Medicine, Northumbria Healthcare Foundation Trust and Dr Samantha Bracebridge, Field Epidemiology Training Programme Director, Public Health England. The authors also thank all members of participating GUM clinic teams who contributed to this research and report to NEESS.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was granted for this study by the NRES Committee North East – York (REC reference: 14/NE/1160) and research and development management approval obtained from all participating NHS trusts.