
Abstract
In India, while an overall reduction in HIV is achieved among most key populations, the continued higher prevalence among people who inject drugs (PWIDs) is an area of concern. This paper analyses unsafe injecting and sexual risk behaviours in male PWIDs according to HIV status and also examines the determinants of HIV infection in this high-risk group. Data from India’s Integrated Biological and Behavioural Surveillance, conducted across 29 Indian states and Union Territories among 19,902 male PWIDs, were used. Informed consent was obtained and men aged 15 years or more, who used psychotropic substances or drugs in the past three months for non-medical reasons were recruited for the survey. Results from the multivariable analysis suggest that drug use debut at age 25 years or above (adjusted odds ratio [AOR]: 1.41, confidence interval [CI]: 1.05–1.88), engagement in drug use for a longer duration (AOR: 1.81, CI: 1.32–2.48), injecting three times or more per day (AOR: 1.53, CI: 1.1–2.12), sharing of needle/syringes (AOR: 1.34, CI: 1.02–1.76), self-reported sexually transmitted infections (AOR: 1.55, CI: 1.12–2.14) and higher self-risk perception for exposure to HIV (AOR: 2.08, CI: 1.58–2.75) increase the likelihood of HIV infection. Sustained higher prevalence, unsafe injecting and risky sexual practices are major challenges which may prevent India from reaching the ‘end of AIDS’ by 2030. This underscores the need for adoption of a tailored, evidence-driven HIV prevention approach that adequately addresses local needs to limit the spread of HIV within this population, and thereby prevents the onward transmission of HIV to the general population.
Introduction
Injecting drug use is a public health problem affecting individuals and economies.1–6 Globally, people who inject drugs (PWIDs) account for 8% new HIV infections. 6 Sharing of needles/syringes and contaminated equipment is the primary risk factor for HIV exposure,7,8 and via sexual transmission, the virus can potentially pass on to the general population. 7 Due to sharing of contaminated injecting equipment, PWIDs are also at risk of acquiring hepatitis B and C virus.3,5,9 Additionally, the structural factors such as politico-legal environment, sociocultural ethos, illegal drug distribution, harassment, stigma, discrimination and lack of social support systems play a decisive role in increasing the vulnerability of this high-risk population. 10
In India, the HIV epidemic remains concentrated among key populations (KPs), including female sex workers (FSWs), men who have sex with men (MSM), Hijra/transgender people and PWIDs. Injecting drug use is one of the main drivers of the HIV epidemic in the country.11,12 With an estimated population of 177,000, PWIDs form the third largest risk group after FSWs and MSM. 12 The Indian National AIDS Control Program identifies them as a core group requiring targeted interventions including harm reduction strategies. 13 HIV prevalence among PWIDs in the last two rounds of HIV Sentinel Surveillance (HSS) was 9.2% (2008–9), and 7.14% (2010–11).14,15 The 2014–15 Integrated Biological and Behavioural Surveillance (IBBS) conducted among male PWIDs found an HIV prevalence of 9.9%, which is the highest across the different high-risk groups. 12 The states with the highest prevalence in this group were Bihar, Uttar Pradesh and Uttarakhand (27.2%), followed by Delhi and Rajasthan (21.8%), Chhattisgarh and Madhya Pradesh (13.6%), Manipur (12.1%) and Mizoram (10.0%). 12 HSS data also show that HIV prevalence in PWIDs rose in the last two rounds in Uttar Pradesh, Chhattisgarh, Uttarakhand and particularly in Mizoram. Antenatal prevalence is also on the rise in some states where injection drug use prevalence is very high such as Uttar Pradesh, Delhi and Rajasthan. While the HIV prevalence among most of the KP groups has reduced,14,15 the continued high prevalence among PWIDs and diffusion of the virus due to injection drug use across different states have raised concerns on the overall epidemic scenario in the country.11,16–21
Studies from India have found that several factors increase the risk of HIV among PWIDs categorised mainly with regard to injecting practices or sexual behaviours. Descriptive studies suggest that the sharing of needles/syringes and use of contaminated injecting equipment was common.22–27 Likewise, higher risk for HCV and HBV has also been documented in several states, indicating high levels of needle/syringe and equipment sharing.9,28–30 Longer duration of injecting and irregular supply of needles/syringes was found to be associated with HIV and HCV.9,31 PWIDs with unsafe injecting practices were shown to have multiple sexual partners, use condoms inconsistently and engage in risky sexual practices.10,13,18,26,32 Dual risk behaviours of PWIDs make their sexual partners highly vulnerable to HIV. Studies among spouses/regular partners of PWIDs have documented the higher prevalence of HIV and inconsistent use of condoms.23,26,27,33,34 IBBS data also show that consistent condom use by male PWIDs with regular partners is very low overall. Less than one in ten PWIDs use condoms consistently with regular partners in high PWID prevalence states like Uttar Pradesh, Uttarakhand, Bihar and Rajasthan. 12 Further, HIV infection risk depends on type of drug(s) used, and injection of opioid pharmaceuticals alone or together with antihistaminic and/or sedative synthetic drugs is on the rise. Their use is associated with higher injection-related risk and complications.23,25,34,35 Other risk factors for HIV exposure were a history of incarceration and tattoos, and being in prison. 23 In contrast, exposure to focussed HIV prevention interventions has been documented to increase safer injecting and protective sexual behaviours among PWIDs.16,19,36
Many of the earlier studies among PWIDs are region specific and lack the critical national perspective, which is important for a country like India. Given that HIV prevalence continues to be high in PWIDs and that the injecting drug use epidemic in some states outside the north-eastern region is on the rise,14,15 it is crucial to re-examine HIV-related risk behaviours among PWIDs by using data from India’s 2014–15 IBBS which is the largest and most recent providing geographically-representative estimates. This paper attempts to analyse unsafe injecting and sexual risk behaviours in male PWIDs according to HIV status in India and also examines the determinants of HIV infection in this high-risk group. The results of this analysis will be useful to understand how the relevant policies and programmes have made an impact on the targeted respondent groups as well as it would help to identify the gaps to mitigate the challenges going forward by the policymakers and programme managers aimed at reducing risk behaviours and strengthening existing programmes.
Methods
Data source, setting and sample
Data for the current analysis were derived from a probability-based, cross-sectional, IBBS survey, conducted among 19,902 male PWIDs in 2014–15, in 53 randomly selected domains across 29 states and Union Territories in India. Eligible respondents included (1) men, aged 15 years or more; (2) who used any psychotropic (addictive/mind-altering) substance or drugs in past three months for recreational or non-medical reasons through injections and (3) provided informed consent for behavioural and biological data collection. Time location and conventional cluster sampling methods were employed to recruit respondents depending mainly on site characteristics. Behavioural information was gathered by trained investigators using a structured questionnaire covering various thematic areas: demographics and injecting practices, sexual behaviour, knowledge on sexually transmitted infection (STI)/HIV/AIDS, stigma and exposure to prevention interventions. Further, blood specimens collected using dried blood spot methods were tested for HIV following two test protocols. The respondents were compensated for their time and effort (Rs 100) and their travel expenses to the study site were reimbursed. Ethical clearance for the survey was obtained from the ethics committees of participating Indian Council of Medical Research institutes and the National AIDS Control Organization. The detailed survey methodology is available elsewhere. 12
Measures
Dependent variable
The dependent measure considered for the analysis in this study was HIV status, determined based on a laboratory test. Two test protocols were used in IBBS for testing: the first test tested all specimens, and only reactive samples were subjected to the second test. Those reactive in both tests were labelled as HIV infected. For the current analysis, those infected (HIV-positive) were coded as ‘1’ and those uninfected (HIV-negative) as ‘0’.
Independent variables
The independent variables considered were profile of respondents, injecting practices, sexual behaviours, HIV knowledge and programme exposure. The profile information included age of respondent (in years), literacy (illiterate/literate), marital status (never married, currently married and widowed/separated/divorced) and main occupation (categorised as labourers/non-labourers). The drug use-related behaviour were age at initiation of injecting drug use (≤24 years/25+ years), duration of injecting drug behaviour (≤4 years/5+ years), most often injected drug in last three months (heroin/brown sugar, Buprenorphine, Spasmo Proxyvon, sedatives [Diazepam/Calmpose, etc.], etc.), frequency of injecting (≤1 time/day, 2 times/day, 3+ times) and borrowed/lent used needles/syringes. The sexual behaviours considered were age of sexual debut (≤17/18+ years); having regular, paid and casual female partners; ever had male/Hijra partners and consistent condom use with different partners. The other independent variables included having comprehensive HIV knowledge, self-risk perception (high/moderate risk for HIV and low risk/no risk); ever tested for HIV; contacted at least two times by a peer educator or outreach worker in last month; received at least 30 new needles/syringes in last month; received at least ten condoms in last month, and exposure to any HIV/AIDS services in last 12 months; and reporting having suffered from an STI in last 12 months (see description in Tables 1 and 2)
Sample characteristics, contextual factors and HIV prevalence, male PWIDs, IBBS, 2014–15.a
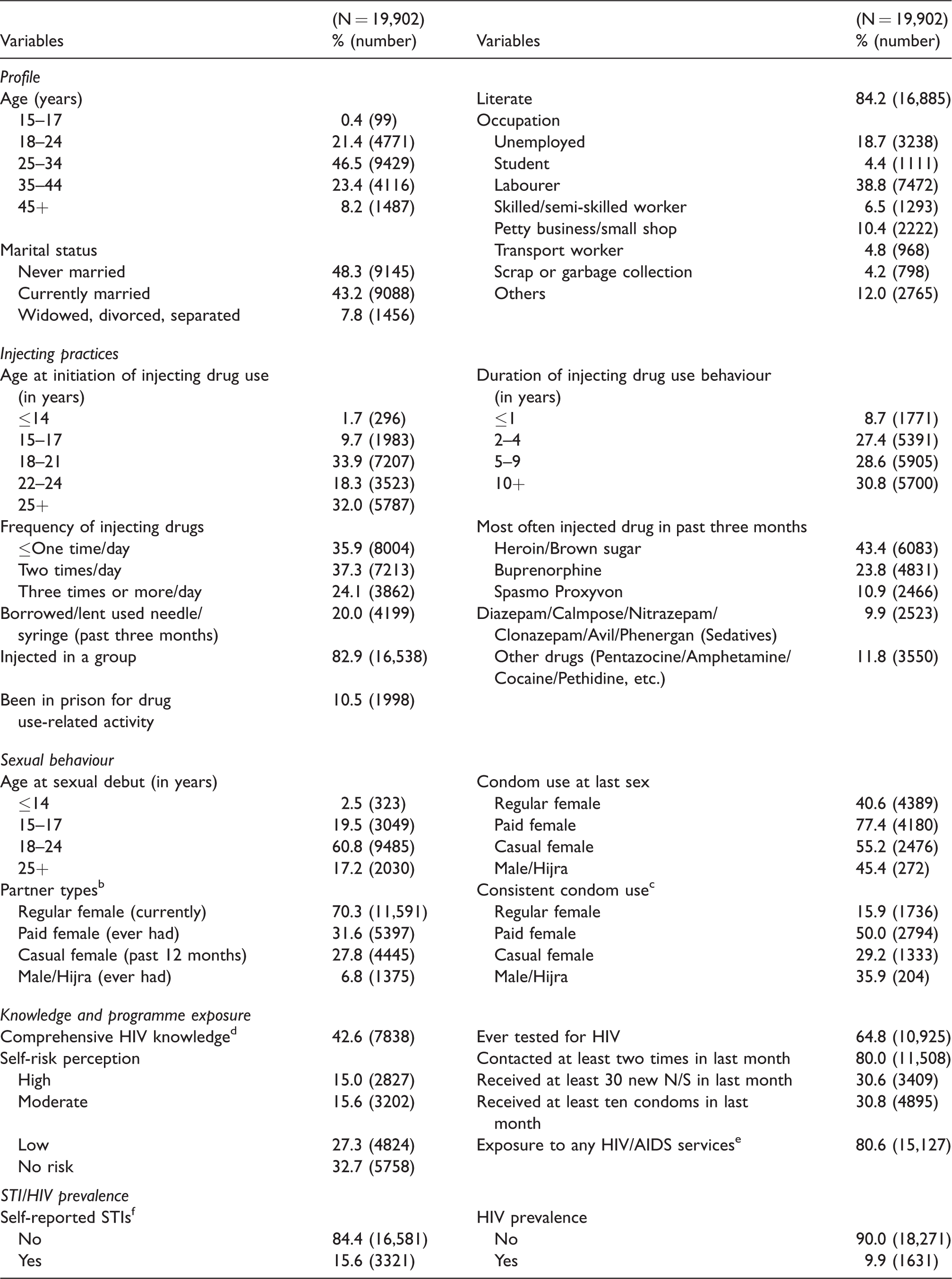
IBBS: Integrated Biological and Behavioural Surveillance; PWIDs: people who inject drugs; STI: sexually transmitted infection; N/S: needles/syringes.
aAll proportions presented are weighted and totals may not add up to 100% due to missing values, others or no response categories.
bRegular (spouse or girlfriend with whom the respondent has a steady relationship), Paid (whom the respondent paid in cash to have sex with), Casual (non-paid female partners, other than the regular).
cUse of condoms at each sex act (every time) during past 12 months.
dDefined as (i) knowing two major ways of preventing the sexual transmission of HIV (using condoms and limiting sex to one faithful, uninfected partner), (ii) rejecting two most common local misconceptions about HIV transmission and (iii) being aware that a healthy-looking person can be infected with HIV.
eIf they reported that they had received one or more of the following services: received new needles/syringes, received condoms, received information on STI/HIV/AIDS, seen demonstration on condoms from peer educator or outreach worker or received oral substitution therapy, received abscess management, referred for overdose management, referred to other services (ICTC, detox centres), received check-ups, counselling and free medicine for STI, received help and support for physical or sexual violence and when faced with trouble from police.
fAmong those who reported suffering from any one of the STI symptoms (genital ulcer/sore, urethral discharge or genital warts) in past 12 months.
Association between HIV status and related risk behaviours, male PWIDs, IBBS, 2014–15.a

CI: confidence interval; IBBS: Integrated Biological and Behavioural Surveillance; PWIDs: people who inject drugs; STI: sexually transmitted infection.
aAll proportions presented are weighted, and totals may not add up to 100% due to missing values, others or no response categories.
bUnemployed, student, skilled/semi-skilled workers, petty business/small shop, a transport worker, scrap or garbage collection and others.
cRegular (spouse or girlfriend with whom the respondent has a steady relationship), Paid (whom the respondent paid in cash to have sex with), Casual (non-paid female partners, other than the regular).
dUse of condoms at each sex act (every time) during past 12 months.
eAmong those who reported suffering from any one of the STI symptoms (genital ulcer/sore, urethral discharge or genital warts) in past 12 months.
fDefined as (i) knowing two major ways of preventing the sexual transmission of HIV (using condoms and limiting sex to one faithful, uninfected partner), (ii) rejecting two most common local misconceptions about HIV transmission and (iii) being aware that a healthy-looking person can be infected with HIV.
gIf they reported that they had received one or more of the following services: received new needle/syringes, received condoms, received information on STI/HIV/AIDS, seen demonstration on condoms from peer educator or outreach worker or received oral substitution therapy, received abscess management, referred for overdose management, referred to other services (ICTC, detox centres), received check-ups, counselling and free medicine for STI, received help and support for physical or sexual violence and when faced with trouble from police.
Statistical analysis
The data from all states were merged, and appropriate national weights were calculated and applied. Therefore, results are presented for the overall sample. Missing or “don’t know” cases were excluded from the analysis; such cases were few. The bivariate and multivariable analyses were undertaken to understand the association between HIV infection as the outcome and the profile, behavioural and programme exposure variables as independent predictors. The factors significantly associated (p ≤ 0.05) with HIV prevalence in bivariate analysis were retained in the final multivariable model. However, regardless of the statistical significance, after assessing for multicollinearity, consistent condom use variables and some programme exposure indicators were dropped from the model. STATA 13.0 was used for the analysis.
Results
The overall sample included 19,902 male PWID respondents, of whom 1631 (9.9%) tested positive for HIV. Most respondents were aged between 25 and 34 years (46.5%), literate (84.2%), never married (48.3%) and worked as labourers (38.8%) or were unemployed (18.7%). The median age of initiation of drug use was 22 years, and the median duration of injecting drug behaviour was six years. Heroin/brown sugar (43.4%) and Buprenorphine (23.8%) were the drugs reported to be injected most often. Most respondents reported having a regular female partner (70.3%); fewer said that they had paid (31.6%) and casual (27.8%) partners or male/Hijra partners (6.8%). Consistent condom use was low overall, especially with regular (15.9%) and casual female partners (29.2%) and with male/Hijra partners (35.9%) (see Table 1).
HIV infection and its association with other risk factors
The factors found to be associated with increased odds of HIV infection were drug use debut at age 25 years or above (41.0% versus 32.5%; adjusted odds ratio [AOR]: 1.41, confidence interval [CI]: 1.05–1.88, p = 0.022), injecting heroin/brown sugar (37.9% versus 44.1%; AOR: 1.55, CI: 1.02–2.35, p = 0.039), and Buprenorphine (40.0% versus 21.8%; AOR: 2.67, CI: 1.73–4.12, p = 0.001), engaging in injecting drug use behaviour for five years or more (73.8% versus 60.7%; AOR: 1.81, CI: 1.32–2.48, p = 0.001), injecting drugs three times or more per day (33.4% versus 23.6%; AOR: 1.53, CI: 1.10–2.12, p = 0.039), having borrowed/lent used needles/syringes in past three months (26.7% versus 19.2%; AOR: 1.34, CI: 1.02–1.76, p = 0.033), perceiving high/moderate self-risk of exposure to HIV (51.1% versus 31.8%; AOR: 2.08, CI: 1.58–2.75, p = 0.001), having been contacted at least twice by peer educator or an outreach worker in last month (86.6% versus 79.2%; AOR: 1.52, CI: 1.05–2.19, p = 0.024) and reported to have suffered from at least one STI symptom in past 12 months (21.7% versus 14.8%; AOR: 1.55, CI: 1.12–2.14, p = 0.007) (see Table 2). However, respondents who were literate (71.1% versus 85.8%; AOR: 0.69, CI: 0.50–0.95, p = 0.024), reported having had a sexual debut after 18 years of age (72.9% versus 78.6%; AOR: 0.68, CI: 0.50–0.92, p = 0.014), having a regular (63.2% versus 71.6%; AOR: 0.60, CI: 0.43–0.84, p = 0.003) and casual (18.9% versus 29.2%; AOR: 0.54, CI: 0.40–0.73, p = 0.001) female partners were at lower odds of HIV infection compared to their counterparts (see Table 2).
Discussion
This analysis is based on in-depth analysis of data which was gathered through the largest surveillance survey conducted in the world. The IBBS in India was conducted among male PWIDs with an overall sample size of 19,902 respondents. Consistent with the existing evidence on injection drug use, we found that engaging in drug use behaviour for a longer duration, higher frequency of drug use coupled with unsafe injecting practices were important risk factors associated with HIV infection. Having regular or casual sex partners was not associated with HIV infection. However, self-perceived high or moderate risk of HIV and suffering from STIs were found to be associated with increased risk of HIV infection.
HIV infection is an outcome of many contributing factors, and individual risk behaviours are at the core alongside factors operating at the structural level. Engaging in injecting drug use behaviour for at least five years or more, injecting three times or more per day and borrowing/lending used needles/syringes were the factors having a higher likelihood of HIV infection. Our findings are in concurrence with those of other studies among PWIDs in India and elsewhere, and these risk factors have been commonly reported.23,25,29,30,37,38 To reduce the risk of HIV transmission from sharing of needles/syringes or other contaminated equipment, targeted prevention interventions need to be implemented at a wider scale as their coverage is inadequate. IBBS found that service coverage varied considerably across states, with less than 70% of respondents having received any HIV service in the last 12 months in high prevalence states such as Uttar Pradesh, Rajasthan, Chhattisgarh and Madhya Pradesh. Only 5% of respondents reported having received 30 sterile needles/syringes per month in Uttar Pradesh, while the national average was 30%. 12 In a study across north-eastern states of India, lack of access to new needles/syringes and inconsistent supply from intervention projects were the main reasons reported for re-use of injecting equipment. 22 Further, in IBBS, 80% of PWIDs said they were visited or contacted by outreach worker or peer educator at least twice a month. The findings from the current analysis suggest that this group was more likely to be HIV infected which suggests that the programme has been able to reach out to male PWIDs at higher risk. However, less than a third of respondents in the study indicated they received at least 30 needles/syringes or a minimum of ten condoms a month. The reach of these essential commodities/services needed to prevent HIV transmission is clearly insufficient, both overall as well as in key states where injecting drug use is driving the epidemic. 12 The services/commodities being provided also need to be rationalised in terms of quantity. This shortcoming compromises the effectiveness and impact of HIV prevention programmes and represents a major barrier in ending AIDS. Existing evidence suggests that the repeated peer-led outreach activities are effective in promoting safe injecting practices.19,36,39 Likewise, the role of needles/syringes exchange programmes, opioid substitution and antiretroviral therapy in reducing HIV7,40 are well established and documented. What is required is an assessment of the existing implementation mechanisms to understand the insufficient reach of services/commodities so that overall coverage and service delivery may be improved and efficient implementation mechanisms may help in reducing the risky injection practices and preventing infections in sexual partners of male PWIDs.
Sexual transmission from or among PWIDs is also a significant risk factor for HIV.23,33,34 This study found that male PWIDs, despite having regular and casual female sex partners in past 12 months, were not at an increased risk of HIV infection. This suggests that sharing of contaminated injecting equipment is a more important determinant of HIV infection. These findings are similar to a multi-site assessment where having up to three sex partners was associated with lower risk of HIV. 38 An earlier study among PWIDs also found that sex and condom use with sex workers were not related to increased risk but injecting multiple times was associated with HIV infection. 23 However, condom programmes targeted at PWIDs are nevertheless essential to prevent transmission of HIV to their female and male sexual partners. In IBBS, condom use with both casual and regular partners was low with nearly 70% of respondents who reported having used condoms inconsistently with their casual partners and only 15% having used condoms consistently with their regular partner. 12 Sexual transmission risk for PWIDs themselves can also not be ruled out entirely, because of a relatively high self-reported STI rate (15.6%), with those who reported having had at least one STI symptom more likely to be HIV infected. These findings underscore the need for comprehensive multi-level combination prevention interventions for risk reduction among PWIDs. Although HIV testing was not found to be a critical determinant in this analysis, programmes need to continue fostering testing uptake in line with India’s test and treat policy. One-third of the PWIDs in this sample never tested for HIV and this is a potential risk group completely missed out by the programme.
Further, this study found that PWIDs who most often injected heroin/brown sugar, and Buprenorphine (most commonly used drug in IBBS) were at higher risk of HIV infection compared to those who injected another types of drugs. Other recent studies found that unsafe injecting practices were higher among pharmaceutical opioid injectors than heroin users 41 High use of stimulants (cocaine and methamphetamine) has also been documented in states with emerging epidemics. 25 This differential risk needs to be considered, as it has implications for prevention programmes given the increasing non-medical use of pharmaceutical drugs as reported in many Indian states.25,41,42 The perceived high/moderate risk of HIV was also found to be associated with HIV infection. Lack of self-efficacy has often been noted to reduce adherence to treatment or service uptake. 43 In this case, the perceived higher risk for HIV exposure could be positively used to bring change or modify unacceptable behavioural practices.
These are findings from the largest survey conducted in India across 29 states which have implications for HIV prevention programmes among PWIDs. However, like all studies, this study also has some limitations. First, since the study design is cross-sectional, it suffers from issues related to social desirability bias and inability to draw inferences on causality. Second, the findings in this paper are based on a pooled analysis of data collected in different states, yet there are substantial geographical differences in HIV estimates across regions and states, and these may have affected the estimates. However, to account in for this variability, national weights were calculated and used for the pooled analysis. Lastly, the methodology used in the 2014–15 IBBS differs from that used in other behavioural or bio-behavioural studies conducted in India, and the scale of IBBS is much larger making comparisons difficult.
Conclusion
The sustained higher prevalence of HIV among male PWIDs is a persistent challenge for the National AIDS response. If unattended this could be the primary barrier to achieving ‘End of AIDS’ by 2030. The data from the 2014–2015 IBBS suggest that engagement in drug use for a longer duration, injecting multiple times, sharing of needles/syringes, injecting heroin/brown sugar or Buprenorphine, having an STI and higher perceived self-risk of HIV exposure increase the likelihood of HIV infection in male PWIDs. The findings indicate the need for improving the coverage and impact of prevention interventions among PWIDs, especially through scale-up of needle/syringe programmes and provision of condoms. Unless tailored and evidence-driven interventions adapted to local epidemic dynamics context are designed and adequately implemented, it will be difficult to limit the rapid spread of HIV within this population and onward transmission to their sexual partners.
Footnotes
Acknowledgements
The authors wish to thank the researchers/staff of the State AIDS Control Societies and the Research Institutes for their relentless support during the different phases of the IBBS. Finally, we are grateful to the respondents who took their time and participated in the survey.
Authors’ contributions
PK, BS, SR contributed to the conception, design, data analysis, writing and finalisation of the manuscript. SA and SV critically reviewed and supported in finalisation of the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.